Measles Vaccination Coverage Analysis among Nomadic Communities, Kunene Region of Namibia, 2010 – 2014
*Corresponding Author(s):
Sheehama JUnam School Of Medicine, Oshakati, Namibia
Tel:+264 652232247 / +264 814348018,
Email:jsheehama@unam.na
Abstract
Measles a highly infectious disease caused by Paramyxovirus, in 2012, accounted for 1,22,000 deaths worldwide. In Namibia measles is targeted for elimination and the strategies for elimination include vaccination, case management and surveillance. Since 2010 there have been several outbreaks of measles in Kunene Region of Namibia, among the nomadic communities living in this area mostly. Data on cases were line listed but were not analysed. We analysed this data to determine the trends of measles cases, and risk factors so as to provide information for appropriate intervention. We conducted a descriptive analysis, reviewed the line list and case based forms of measles cases from Khorixas, Opuwo and Outjo district from January 2010 to December 2014. The information for the suspected cases were collected by using the following variables; age in years, sex, district, number of measles doses, laboratory result, source of vaccination information. The database is managed by the Health Information Officer who updates the database as new cases are reported. There is no mechanism to confirm that the variables are appropriately coded. We exported the excel line list to Epi-Info 7, cleaned the data and analysed by person, place and time. We calculated simple frequencies and proportions.
Keywords
Khorixas; Kunene; Measles; Opuwo; Outjo; Vaccination
INTRODUCTION
In Namibia, measles is listed as one of the priority diseases, conditions and events for Integrated Disease Surveillance and Response, under the category of epidemic prone diseases [4]. Measles immunisation coverage is one of the indicators for National Development Goals (NDG), goal 4, reduce child mortality [5]. In Namibia measles is targeted for elimination and the strategies for elimination include vaccination, case management and surveillance. The Kunene Region population is 81,423 people in the Kunene Region, the health services are provided through hospitals, health centres, clinics and outreach services. Kunene has three district hospitals, three health centres and 1,512 outreach points and the outreach points receive visits from a team from each district hospital at least once a month.
Kunene region is vast, remote and sparsely populated with very poor infrastructure, geographical barriers that are a huge challenge for health service delivery. The region is also prone to outbreaks like cholera and measles. At this point measles disease is still of big concern in the Kunene Region as it continues to the cause of morbidity in this where it has annual and seasonal outbreaks. From 2010 to 2014, there have been several outbreaks of measles in Kunene Region, among the nomadic communities living in this area mostly. Even if measles is a vaccine preventable disease, the disease outbreaks are frequent in Opuwo District. In 2006 the national immunisation coverage for measles was at 83%, while Kunene Region and Opuwo District was 60% and 40% respectively [6]. Data on cases were line listed but were not analysed. We analysed this data to determine the trends of measles cases, and risk factors so as to provide information for appropriate intervention. In this study we analysed the surveillance data which were obtained from the District Health Information System (DHIS) from the Epidemiology Division of the Kunene Region.
The main objective for the surveillance system is to gather information on disease in order to facilitate planning and take action, for immunisation coverage and vaccine efficacy. The disease is reported to the district office by the health facility where the suspected case is seen. The reporting facility should fill in the case investigation form and take specimen which is then sent to the laboratory in Opuwo for testing. According to the Namibia 2011 Population and Housing Census Main Report [7], Kunene Region has a total population of 92988 people in 2014, of which the children under five years of age are 15808.
METHODS
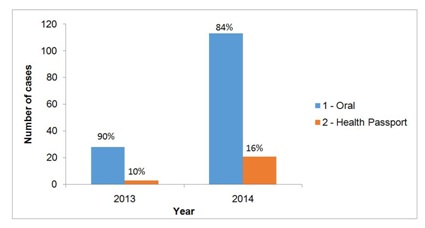
We conducted a descriptive analysis. We reviewed the line list and case based forms of measles cases from Khorixas, Opuwo and Outjo District from January 2010 to December 2014. A measles case is any person in whom a clinician suspects measles infection with fever and maculopapular rash. The information for the suspected cases were collected by using the following variables; age in years, sex, district, number of measles doses, laboratory result, source of vaccination information. Using a patients’ health passport of information is significant, which is health/medical record book for issued to any person visiting the public health facilities in Namibia, that document the services he or she received from the health facilities.
The database is managed by the Health Information Officer who updates the database as new measles cases are reported. There is no mechanism to confirm that the variables are appropriately coded. We exported the excel line list to Epi-Info 7, cleaned the data and analysed by person, place and time. We calculated simple frequencies and proportions.
RESULTS
|
Sex |
Frequency |
Percent |
|
Female |
181 |
54% |
|
Male |
152 |
46% |
|
Total |
333 |
100% |
The modal age was 7 years, the minimum and maximum ages were 1 month and 61 years respectively (Figure 1). A total of 181 (54%) cases were female; 130 (39%) were in 5 to 9 years age group, and 234 (70%) came from Opuwo District. Only 96 (29%) cases were vaccinated, while the national immunisation coverage for measles was at 83%, while Kunene Region and Opuwo District was 60% and 40% respectively and the majority of cases did not carry health passport.
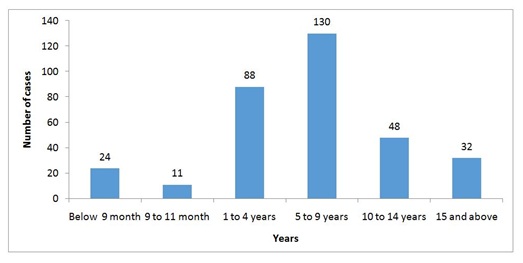
Figure 1: Measles cases in Kunene Region by age group, January 2010 - December 2014.
The majority of cases were in the 5 to 9 age group 130 (39%) cases followed by the 1 to 4 age group with 88 (26%) cases. The modal age was 7 years and the minimum and maximum ages were under 1 month and 61 years respectively (Figure 1). The attack rate among the less than 5 years age group was 0.78%. The vulnerable of child growth period 5 - 9 years I mostly affected which require more hygiene care to this group of children.
A large percentage of cases (70%) came from Opuwo district, followed by Outjo district with 16% while Khorixas district had 14% (Figure 2). This can be very much based on the health attitude seeking behaviours of the people, mostly preferring to seek health services at the regional hospital other than a district hospital. Opuwo population remain the capital city of the nomadic people in Kunene region, while Outjo and Khorixas remain more habitats for the township house hold.
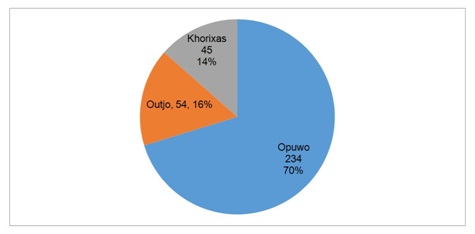
Figure 2: Distribution of measles cases in Kunene Region by Districts, January 2010 - December 2014.
Overall, the graph shows an increasing trend from 65 cases in 2010 to 133 cases in 2014, however there was fewer cases observed in 2012 and 2013 of 29 and 31 respectively (Figure 3). But the rise has increased significantly in 2014, which rise concerns on the quality of public health services and community health education. The health funds has been surging since 2013, as a number of community worker trained for Kunene region mostly remain unemployed. This fact of no-funds to employ the community based health workers who are very much important for better hygiene and health promotion in these communities.
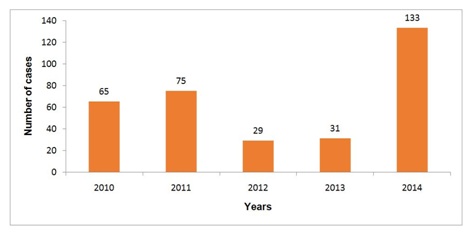
Figure 3: Trends of measles in Kunene Region, January 2010 - December 2014.
The threshold which is the presence of a single infected individual that is not sufficient to be classified as an outbreak, is mostly in the month of December each year (Figure 4). This the period having low number of possible cases which we define as the number of infected individuals needed for the disease to spread in an approximately deterministic manner. The measles cases have an association to seasonal period of harsh cold weather starting mostly with June, cold front and people ignore personal hygiene.
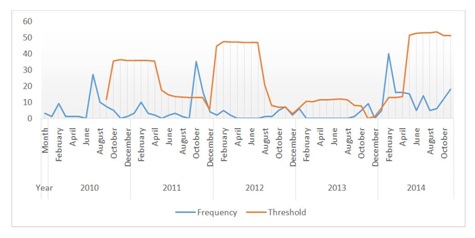
Figure 4: Epidemiological threshold and frequency of measles cases in Kunene Region, January 2010 - December 2014.
In 2010, there was a peak of cases observed in July; in 2011 the peak was in October, in 2012 and 2013 fewer cases were observed, and in 2014 there was a peak in February (Figure 5). Overall there were more cases in the month of February and in October.
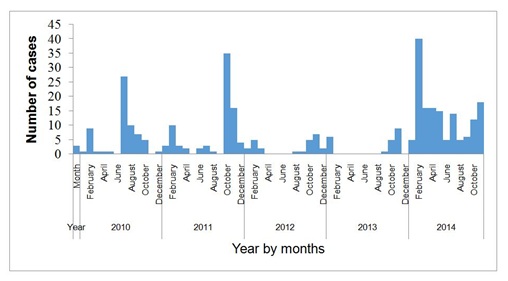
Figure 5: Epidemiological week of measles cases in Kunene Region, January 2010 - December 2014.
Only about 1.5% of the cases have received all three measles doses, 7% received two doses, 20% received one dose, and 20% did not receive any dose (Table 2). More than 50% had unknown immunisation status.
|
Number of Measles Doses |
2010 |
2011 |
2012 |
2013 |
2014 |
Total (%) |
|
Zero |
6 |
26 |
8 |
6 |
19 |
65 (19.5%) |
|
One |
20 |
27 |
6 |
1 |
12 |
66 (20.0%) |
|
Two |
9 |
1 |
1 |
2 |
10 |
23 (7.0%) |
|
Three |
3 |
1 |
0 |
1 |
0 |
5 (1.5%) |
|
Unknown |
27 |
20 |
14 |
21 |
92 |
174 (52.0%) |
A total of 84 cases tested IgM positive, while 4 were positive for rubella. About 70% were negative (Figure 6).
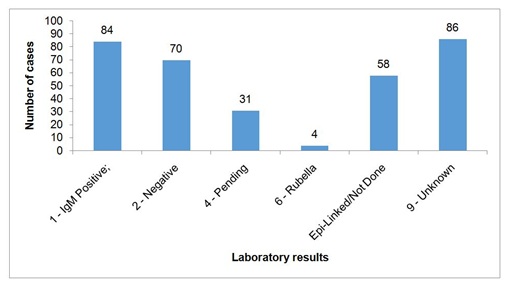
Figure 6: Laboratory results for measles cases, Kunene Region, January 2010 - December, 2014.
The immunisation status of 58 (79%) of the cases was unknown, 10 (14%) were not immunised and only 5 (7%) were immunised (Figure 7). Fourteen percent of the cases tested positive while 47 percent of the laboratory results were pending.
DISCUSSION
Parental factors such as knowledge, attitude, education, and socio-economic status affect immunisation coverage [8]. It was highlighted in the Millennium Development Goals report for 2008 that the target for immunisation of one-year-old children coverage for 2012 is likely to be met but there are considerable regional disparities in immunisation coverage [5]. Most of the cases that tested negative were immunised. One measles attack confers lifelong immunity in an individual.
Long distance to the health facilities and terrain makes it difficult for parents and care taker to take their children for immunisation. This is one of the contributing factors in Kunene region which is the second largest region in Namibia and it has a sparsely distributed population. Most of the residence of Kunene stays in mountain areas with no proper road making it hard to reach health facilities or health workers to reach them. There is also one case whose laboratory result is positive but the health passport indicates that the case was vaccinated.
LIMITATION
RECOMMENDATIONS
Also the recommendation to carry out a study to determine the immunisation coverage in the district and determine the vaccine effectiveness among these communities. The laboratory test and services to these remote health facilities need to be done in a reasonable time, meaning we need to increase the testing capacity of the rural health facilities laboratories.
CONCLUSION
REFERENCES
- Mitchell R, Kumar V, Fausto N, Abbas A, Aster J (2011) Pocket companion to Robbins and Cartran: Pathologic Basis of Disease. In: Pathologic Basis of Disease. (8th edn), Elsevier Saunders, Amsterdam, Netherlands. Pg no: 800.
- Heymann DL (2008) Control of Communicable Diseases Manual. (19th edn), American Public Health Association, Washington DC, USA. Pg no: 729.
- Choe YJ, Eom HS, Bae GR (2014) Vaccine associated measles in the low-incidence country of Korea over a 10-year period. Jpn J Infect Dis 67: 180-183.
- (2011) National Technical Guidelines for Integrated Disease Surveillance and Response. 2nd edition, Ministry of Health and Social Services. Pg no: 319.
- Namibia (2013) Millennium Development Goals. National Planning Commission Republic of Namibia, Pg no: 1-114.
- Tjiveze K (2012) Factors associated with the measles immunisation coverage in the Opuwo health district, Kunene region, Namibia. University of Namibia. Windhoek, Namibia.
- (2011) Namibia 2011 Population and Housing Census Main Report. Namibia Statistics Agency. Pg no: 212
- World Health Organization (2018) Measles. World Health Organization, Geneva, Switzerland.
- Sartorius B, Cohen C, Chirwa T, Ntshoe G, Puren A, et al. (2013) Identifying high-risk areas for sporadic measles outbreaks: Lessons from South Africa. Bull World Health Organ 91: 174-183.
Citation: Nghoshi SS, Sheehama J, Antara S (2018) Measles Vaccination Coverage Analysis among Nomadic Communities, Kunene Region of Namibia, 2010-2014. Adv Microb Res 2: 005.
Copyright: © 2018 Nghoshi SS, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.