Meningitis with Infarcts Is it Always Tubercular?
*Corresponding Author(s):
Ravindra B KambleDepartment Of Radiology And Department Of Neurology, Vikram Hospital, Bangalore, India
Tel:+91 9845781307,
Email:drravindra31@rediffmail.com
Letter to Editor
Sir,
We report a case of multiple brain infarcts caused due to complication of pneumococcal meningitis in a young boy. Physicians are aware of tubercular meningitis with arteritis and infarcts but bacterial meningitis with infarcts appears to be overlooked. Also, it mimics acute ischemic infarct and the diagnosis can be missed unless contrast study is done. 14 year old boy presented with head ache and neck rigidity since 3 days without any neurological deficits. Clinical diagnosis of meningitis was done and patient was referred for imaging. Initially Plain CT scan (64 slice Siemens Somatom) of brain was done which was normal. Next day MRI (Siemens Avanto 1.5t) with contrast was done which showed areas of restricted diffusion involving midbrain, vermis, bilateral temporal, bilateral globus pallidus, left periatrial and left fronto-parietal lobe. It showed T2 and flair hyperintensities in same areas. Post-contrast imaging showed meningeal enhancement with exudates in the interpeduncular cistern, bilateral Sylvian fissures, left parietal sulci, prepontine cistern, pineal recess and left trigonal ventricular wall. MR angiogram was normal. Imaging diagnosis of meningitis (and ventriculitis) with acute infarcts due to arteritis was made (Figure 1). Later CSF analysis showed protein -370mg/dl, sugar-10mg/dl, chloride-11mmol/L and culture showed growth of streptococcus pneumoniae. Patient was immediately started with appropriate antibiotics and subsequently patient recovered well.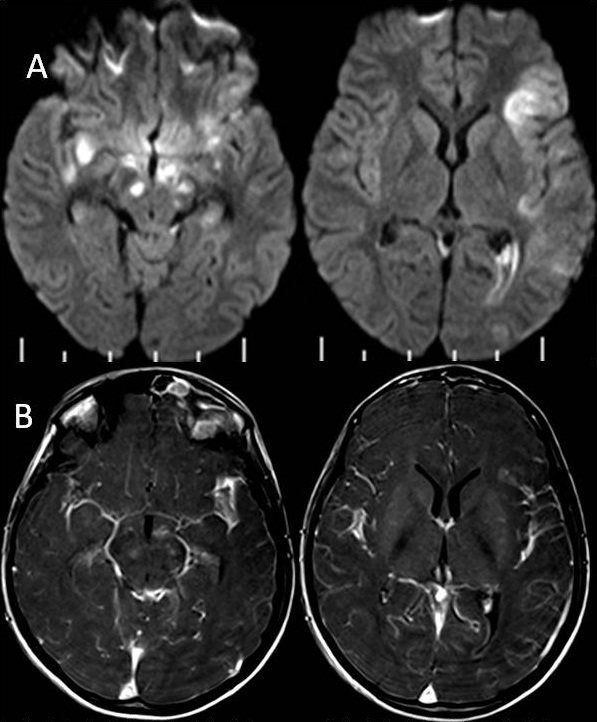
Figure 1:Diffusion weighted image in A showing multiple areas of restricted diffusion and areas of meningeal and ependymal enhancement as shown in post contrast T1W image in B.
Streptococcus pneumoniae is one of the cause of bacterial meningitis causing occasional complications like brain abscess, encephalitis, infarcts and encephalomyelitis. Pneumococcal meningitis is an important cause of bacterial meningitis causing vasculitis and infarcts [1]. Immunologically mediated vasculitis with thrombosis and cytotoxic edema are causes described in pneumococcal meningitis and infarcts and diffusion weighted imaging shows restricted diffusion suggesting cytotoxic edema in acute infarcts [2]. However diffuse intra cerebral intravascular coagulopathy could also be another cause of infarct apart from vasculitis [3]. Similar findings are also observed in severe cases of tuberculous meningitis where diffusion abnormalities appears earlier than conventional imaging [4]. Pneumococcal meningitis can mimic tubercular meningitis on imaging with exudates and acute infarcts however clinical and historical correlation will help. Careful clinical assessment and MRI with diffusion and contrast imaging study can lead to proper diagnosis of pneumococcal meningitis which is potentially a treatable disease.
REFERENCES
- Mukai K, Yasuda T, Hara K, Funakawa I, Terao A (1996) [Adult pneumococcal meningitis complicated by cerebral infarction: a case report]. Rinsho Shinkeigaku 36: 110-113.
- Jorens PG, Parizel PM, Demey HE, Smets K, Jadoul K, et al. (2005) Meningoencephalitis caused by Streptococcus pneumoniae: a diagnostic and therapeutic challenge. Diagnosis with diffusion-weighted MRI leading to treatment with corticosteroids. Neuroradiology 47: 758-764.
- Vergouwen MD, Schut ES, Troost D, van de Beek D (2010) Diffuse cerebral intravascular coagulation and cerebral infarction in pneumococcal meningitis. Neurocritical care 13: 217-227.
- Shukla R, Abbas A, Kumar P, Gupta RK, Jha S, et al. (2008) Evaluation of cerebral infarction in tuberculous meningitis by diffusion weighted imaging. J Infect 57: 298-306.
Citation: Kamble RB (2015) Meningitis with Infarcts: Is it Always Tubercular? J Clin Stud Med Case Rep 2: 018.
Copyright: © 2015 Ravindra B Kamble, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.