Spontaneous Pneumothorax in Young Female Secondary to Lymphangiomyomatosis
*Corresponding Author(s):
Abhishek R KeraliyaDepartment Of Imaging, Dana Farber Cancer Institute, Massachusetts, United States
Tel:6175436171,
Email:abhishekkeraliya@gmail.com
Abstract
Lymphangiomyomatosis (LAM) is an uncommon cause of secondary spontaneous pneumothorax seen exclusively in women during the reproductive years. Varying sized parenchymal cysts distributed evenly throughout the lungs is the main finding of LAM on HRCT chest. Pleural effusion and pneumothorax are other findings seen on CT chest in patients with LAM. We report a case of LAM in a young female presenting as spontaneous pneumothorax.
Keywords
INTRODUCTION
Spontaneous pneumothorax occurs without an apparent cause and can be classified as either primary or secondary. Primary spontaneous pneumothorax is commonly seen in adolescent males without underlying lung disease. Secondary spontaneous pneumothorax occurs with an underlying lung abnormality. It usually occurs in older people with in the setting of a variety of pulmonary diseases commonly chronic obstructive pulmonary disease. Lymphangiomyomatosis (LAM) is an uncommon cause of secondary spontaneous pneumothorax seen exclusively in young women. LAM is extremely uncommon disease occurring sporadically or in association with tuberous sclerosis. Pneumothorax is common in LAM and is seen in around 40% patients of sporadic LAM. High degree of suspicion is required to diagnose LAM in young females presenting with pneumothorax.
CASE REPORT
A 35 year woman without significant past medical history, presented with sudden onset left sided chest pain and difficulty in breathing. No history of smoking or recent use of hormonal contraception was reported. Her symptoms were not synchronous with menses. Clinical examination revealed decreased air entry on left side of chest. CT chest reveals presence of air in the left pleural cavity (maximum thickness 1.3 cm) suggestive of small pneumothorax (Figure 1). No evidence of mediastinal shift is seen. Multiple varying sized thin walled well defined round to oval cysts (>10) are seen involving both lungs surrounded by normal parenchyma (Figure 2 A&B). The presence of multiple parenchymal cysts in a young woman confirmed the diagnosis of Lymphangiomyomatosis (LAM). The patient was given symptomatic treatment with supplemental oxygen and she improved in 2 days. Follow up X-ray chest showed resolution of pneumothorax. Detailed clinical evaluation including dermatologic and retinal examination did not reveal any evidence suggestive of tuberous sclerosis. Ultrasound evaluation of abdomen reveals no evidence of associated lymphangioleiomyoma, lymphadenopathy or angiomyolipoma. Patient is currently on clinical follow up including pulmonary function tests for assessment of progression of disease.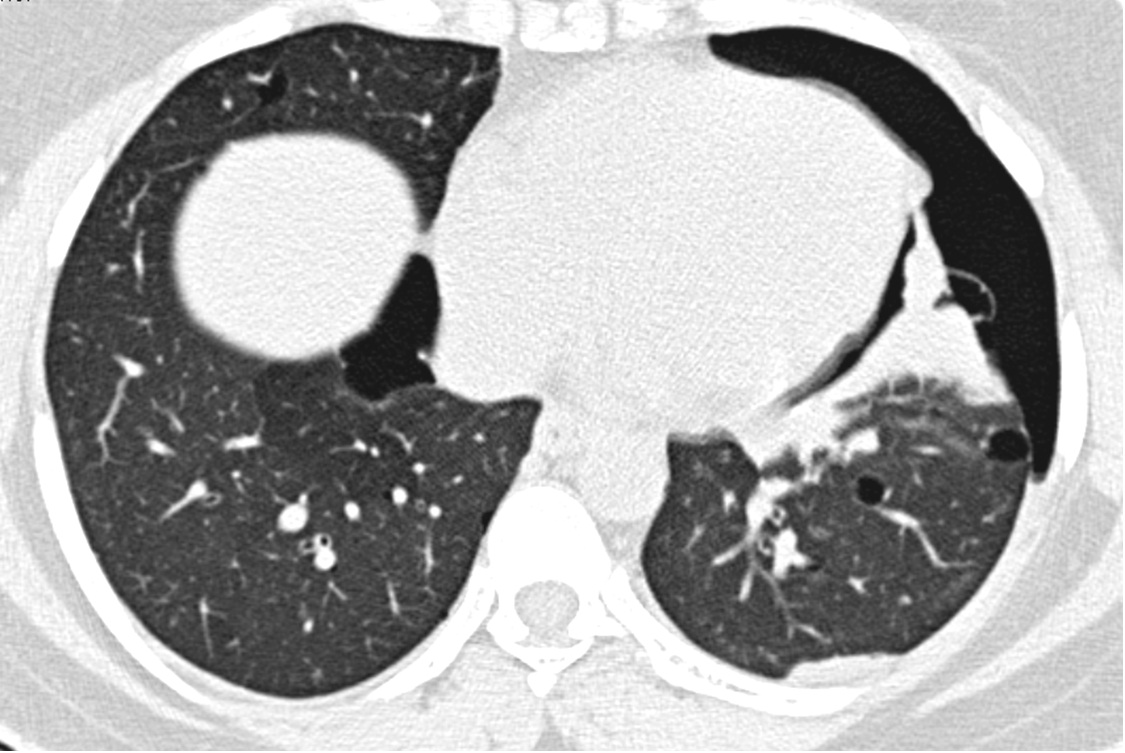
Figure 1: CT chest scan showing left pneumothorax with presence of subpleural cysts.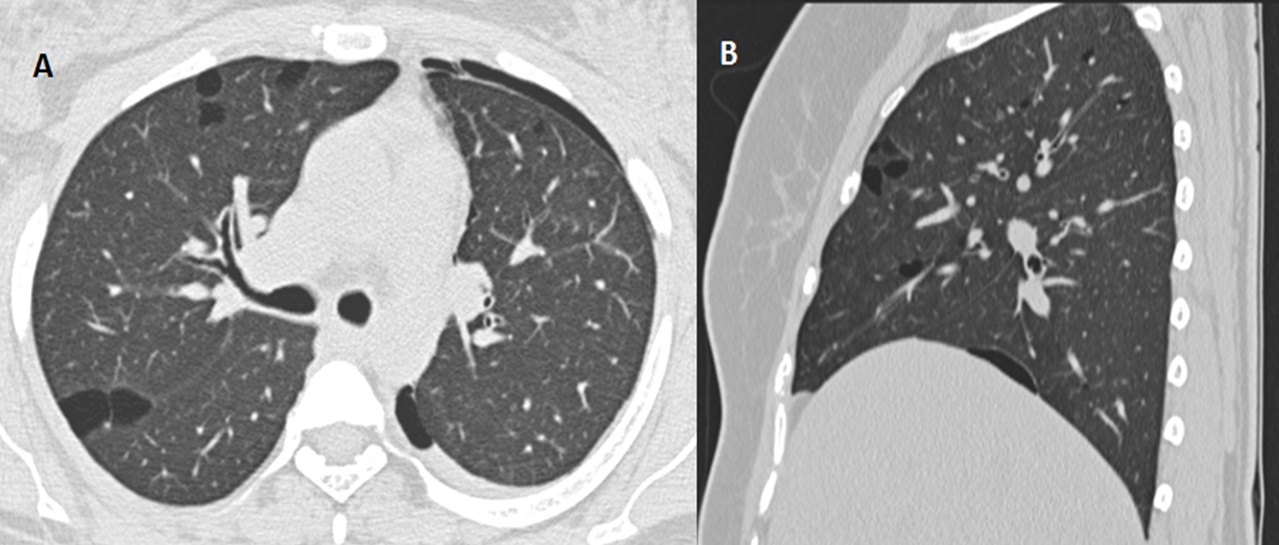
Figure 2: Multiple well defined thin walled parenchymal cysts seen on axial (A) and sagittal (B) CT chest.
DISCUSSION
LAM is an uncommon cause of spontaneous pneumothorax, though pneumothorax is seen commonly in LAM. LAM is a rare multisystem disorder seen exclusively in women during their reproductive years characterized by abnormal proliferation of smooth muscle cells in lymphatics, blood vessels and airways. Slow deterioration of lung function is the usual course. Rapid progression of LAM can occur in patient with hormonal contraception and pregnancy with increased risk of pneumothorax. Characteristic HRCT scan with appropriate clinical history confirms the diagnosis of LAM. Biopsy should be performed only when HRCT or clinical findings are conflicting as it has no role establishing the prognosis.
Varying sized well defined parenchymal cysts distributed evenly throughout the lung with intervening normal parenchyma are the main finding of LAM on high resolution chest CT. Pleural effusion and pneumothorax are associated findings seen on CT chest in patients with LAM [1-3]. Screening CT of abdomen and pelvis is recommended at initial diagnosis of LAM for associated lymphangioleiomyoma, lymphadenopathy or angiomyolipoma. LAM can be seen in approximately 30 to 40% patients with tuberous sclerosis. In addition to typical lung cyst, Multifocal Micronodular Pneumocyte Hyperplasia (MMPH) is seen in tuberous sclerosis characterized by multiple tiny randomly distributed lung nodules.
Pulmonary cyst appears as a round parenchymal lucency or low-attenuating area with a well-defined interface with normal lung on HRCT. Cysts have variable wall thickness but are usually thin-walled (<2 mm). Diagnosis of LAM also requires exclusion of other cystic lung diseases. The differential diagnosis of lung diseases manifesting as diffuse parenchymal cysts includes LAM, Langerhans Cell Histiocytosis (LCH), follicular bronchiolitis, Lymphoid Interstitial Pneumonia (LIP). In addition, a number of diseases can mimic cysts on HRCT imaging including cystic bronchiectasis and emphysematous changes. The LCH is the main differential diagnosis to be considered in patient with LAM. The LCH is characterized by presence of nodules and cysts having upper lobe predilection with relative sparing of lung bases and costophrenic angles, whereas cysts in LAM show diffuse parenchymal distribution without lobar predilection. In addition, cysts in LCH tend to be more irregular in contour, while they are more regular round or ovoid shaped in LAM [4-6]. Patient should be counseled about increased risk of pneumothorax with estrogen containing pills and during pregnancy. First episode of pneumothorax is usually treated conservatively. However recurrent pneumothorax is common and usually treated by pleurodesis or pleurectomy.
To conclude, thin walled parenchymal cysts with intervening normal lung parenchyma, pleural effusion and pneumothorax are characteristic HRCT findings of LAM. Possibility of LAM should be kept in mind in young women presenting with spontaneous pneumothorax.
REFERENCES
- Abbott GF, Rosado-de-Christenson ML, Frazier AA, Franks TJ, Pugatch RD, et al. (2005) From the archives of the AFIP: lymphangioleiomyomatosis: radiologic-pathologic correlation. Radiographics 25: 803-828.
- Oh YM, Mo EK, Jang SH, Yoo CG, Kim YW, et al. (1999) Pulmonary lymphangioleiomyomatosis in Korea. Thorax 54: 618-621.
- Johnson SR, Cordier JF, Lazor R, Cottin V, Costabel U, et al. (2010) European Respiratory Society guidelines for the diagnosis and management of lymphangioleiomyomatosis. Eur Respir J 35: 14-26.
- Hansell DM, Bankier AA, MacMahon H, McLoud TC, Müller NL, et al. (2008) Fleischner Society: glossary of terms for thoracic imaging. Radiology 246: 697-722.
- Seaman DM, Meyer CA, Gilman MD, McCormack FX (2011) Diffuse cystic lung disease at high-resolution CT. AJR Am J Roentgenol 196: 1305-1311.
- Hartman TE (2001) CT of cystic diseases of the lung. Radiol Clin North Am 39: 1231-1244.
Citation: Keraliya AR, Naphade PS (2015) Spontaneous Pneumothorax in Young Female Secondary to Lymphangiomyomatosis. J Clin Stud Med Case Rep 2: 008.
Copyright: © 2015 Abhishek R Keraliya, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.