ABSTRACT
Objective: To determine the prevalence of Glenohumeral Internal Rotation Deficit (GIRD) in adolescent water polo players.
Design: Cross-sectional study.
Setting: High-School Pool Deck.
Patients/Participants: 21 high school athletes.
Main outcome measures: Pre-examination questionnaire, DASH survey and physical examination measuring rotation of the dominant and non-dominant shoulder were completed.
Results: Average internal rotation deficit for the dominant shoulder was 16.5 ± 5.9 with three participants (14%) meeting the definition of GIRD with an internal rotation difference of 25° or more. 13 participants (62%) met the total arc definition of GIRD (greater that 10 arc difference when comparing dominant to non-dominant shoulders). The mean DASH score for our study population was 6.3 ± 8.6. Analysis was performed and the variables of age, years playing, hours swimming, preseason training hours, and throws per week were evaluated for any relationship to glenohumeral internal rotation. None of the above variables had any significant relationship to the development of GIRD, but preseason-training hours per week approached significance (p=0.09).
Conclusion: Our data revealed that 14% of the participants met the definition for GIRD. Preseason training hours approached significance for the development of GIRD, suggesting that higher repetitions of overheard throwing may lead to a decrease in glenohumeral internal rotation. Evaluation of the DASH scores revealed no association between the players with GIRD. Proper preparation, identification of rotational limitations, and treatment of players with GIRD is important to help prevent potential injuries.
KEYWORDS
Glenohumeral Internal Rotation Deficit - GIRD; Overhead athlete; Shoulder; Thrower’s shoulder; Water polo
Introduction
The glenohumeral joint consists of dynamic and static stabilizer, which works, in concert to allow for stability and mobility through a large arc of motion, in recent years there has been significant focus on shoulder motion, particularly in overhead throwing athletes. Many articles have evaluated both adolescent and adult athletes in sports such as baseball, tennis, swimming, handball and volleyball for the prevalence of Glenohumeral Internal Rotation Deficiency (GIRD), its etiology and subsequent prevention and/or treatment [1-5] ,Several theories have been proposed, including boney and soft tissue changes [6-9]. It has been shown that appropriate recognition, training, and therapy can stop the progression of GIRD and decrease the prevalence of injuries [4,10-12]. Failure to recognize GIRD can put the shoulder “at risk” for injury, most notably, the posterosuperior labrum, the undersurface of the posterior supraspinatus tendon, and the anterior inferior capsular structures [9,12-14].
Although many well designed studies have evaluated adolescent baseball players and elite water polo players for GIRD [1,2,14], we are not aware of any studies evaluating adolescent water polo players. This study evaluated high school water polo players for shoulder ROM, prevalence of GIRD and various patient specific variables in an effort to delineate potential causes of GIRD in this population. We hypothesized that adolescent water polo players would have GIRD in their throwing arm and a difference in their arc of motion as compared to the contralateral shoulder. In addition, we hypothesized that increasing age, years playing, hours swimming, and number of throws per week would correlate with a higher prevalence of GIRD and a higher Disabilities of the Arm, Shoulder and Hand (DASH) outcome measure [1,2,4].
Materials and Methods
Participants
After obtaining institutional review board approval, correspondence elucidating the study was submitted to local area high schools and parents of water polo players. Twenty-one local high school players were voluntarily enrolled in the study. Ages of the participants ranged from 14-18 years with a mean age of 15.7 years. There were 17 males and 4 females, all right hand dominant. For the purposes of this study we did not exclude any participants, as our inclusion criteria were athletes less than 18 years old, uninjured, present and practicing at the day of our visit to the pool deck.
Testing
Prior to physical examination each player was provided with a questionnaire to determine: age, years of participation (in water polo), hand dominance, estimated number of throws per week, number of hours swimming per week, and participation in preseason sports specific training (which included core exercises and stretching). In addition, each player completed the DASH outcome questionnaire [15]. Although not specific to the overhead athlete, the DASH score is known to be a reliable tool for assessing upper extremity disability and can be applied to the overhead athlete [3,16].
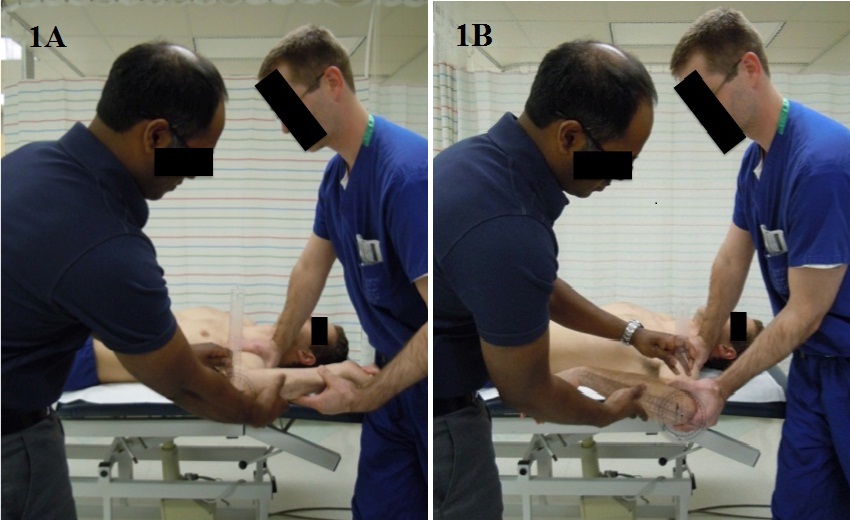
All study participants were examined on the pool deck prior to any stretching or warm-up. Examinations were performed supine and all measurements made with a long arm goniometer by a certified sports medicine physical therapist. The glenohumeral joint was abducted to 90 degrees, the elbow flexed to 90 degrees, and internal and external rotation was measured for both the dominant and non-dominant shoulders. The reference points for measurement were the shaft of the ulna and tip of the olecranon as the center or rotation. Conventional reference points for rotation were followed with 0 degrees indicating neutral position of the forearm (shaft of the ulna perpendicular to the ground). For all measurements, the scapula was stabilized to eliminate scapulothoracic motion and the forearm was held in neutral rotation. Each shoulder was then tested for passive range of motion using standard goniometric technique [17]. A single measurement for both external and internal rotation was done. Maximum rotation was determined by the initiation of scapular motion (Figure 1a and b).
Definition of GIRD
Participants were determined to have exhibited GIRD if their throwing shoulders displayed a 25° or more loss of IR compared with their non throwing shoulders or if there was a greater that 10° arc difference when comparing dominant to non-dominant shoulders [13,18].
Statistical Analysis
All statistical comparisons were performed with Statistical Package for the Social Sciences v 12 (SPSS, Inc. Chicago, Illinois). For categorical comparisons, Chi-square or the Fisher’s exact test (as appropriate) was utilized to evaluate differences in proportions. For continuous variables, Mann-Whitney U was utilized when the data was not normally distributed or variances were not homogenous. ANOVA was utilized as appropriate. Descriptive statistics (mean, standard deviation, percentages) were calculated. Alpha was set at p ≤ 0.05 to declare significance. Total arc range of motion, internal rotation deficit for each shoulder and DASH scores were calculated. Data was analyzed for correlation consisting of a p ≤ 0.05 for GIRD and increasing age, years playing, hours swimming, and number of throws per week.
Results
Twenty-one players in total were evaluated 17 males and 4 females. All participants were right hand dominant. The mean age was 15.7 ± 0.9 years (range 14-18). The mean number of years playing was 3.0 ± 1.4 years (range 0.5-5). On average the players swim 12.9 ± 3.1 hours each week (range 8-20 hours) and spend 1.7 ± 3 hours (range 0-10) each week participating in sport specific training. When evaluating throws, 19% of the participants threw less than 100 balls per week, 57% threw 101-200 balls per week, 5% threw 201-300 balls per week, and 19% of the participants threw greater than 300 balls per week.
Range of motion evaluation of the dominant (throwing) shoulder revealed mean external rotation of 93.6° ± 11.9° and internal rotation of 40.7° ± 10.9°. Range of motion of the non-dominant shoulder showed mean external rotation of 95.3° ± 10.8° and internal rotation of 57.3° ± 12.8°. The total arc range of motion for the dominant and non-dominant shoulders was 134.4° ± 14.9° and 153.1° ± 11.2° respectively. The mean arc difference when comparing the dominant to non-dominant shoulders was 19.5° ± 9.6° with the dominant arm having less arc range in all participants. The average internal rotation deficit for the dominant shoulder was 16.5° ± 5.9° with three participants (14%) meeting the definition of GIRD [1-5,9,12,13] with an internal rotation difference of 25° or more. When evaluating the difference in total arc between dominant and non-dominant shoulders, 13 participants (62%) met the alternative definition of GIRD (greater than 10° arc difference when comparing dominant to non-dominant shoulders). The mean DASH score for our study population was 6.3 ± 8.6.
Analysis was performed and the variables of age, years playing, hours swimming, training hours, and throws per week were analyzed for any relationship to glenohumeral internal rotation. None of the above variables had any correlation with the development of GIRD. However, training hours per week approached significance (p=0.09) but did not achieve significance based on our alpha value of 0.05. Furthermore, there was no correlation between athletes with GIRD and an increased DASH score when utilizing the classical GIRD definition.
Discussion
Numerous past studies [1-5] have evaluated and reported on the rotational differences between the dominant and non-dominant arms in overhead athletes. Many have evaluated athletes that participate in tennis, baseball, swimming, handball and volleyball but we are unaware of any studies evaluating adolescent water polo players. This is the first study to our knowledge evaluating glenohumeral internal rotation deficit in adolescent water polo players. Our examinations showed that 14-62% of the participants met the definition for GIRD (depending on the definition utilized). We hypothesized that increasing age, years playing, hours swimming, and number of throws per week would correlate with a higher prevalence of GIRD and a higher (DASH) outcome measure. Our study, however, did not find any correlation between any of the studied variables.
Our study focused on adolescent water polo players and the majority of clinical data available for GIRD in the adolescent population frequently focuses on baseball [18-20] (Table 1). The cause of GIRD has yet to be definitively established but theories include either an adaptive or developmental causation. Nakamizo et al., evaluated 25 little league pitchers in a biomechanical study [1]. In their study group 40% of the pitchers measured had GIRD and that these players had increased external rotation in their throwing arm as compared to non-throwing controls. They suggested that the development of GIRD happens earlier than previously thought. Meister et al., also evaluated GIRD in little league players [2]. They examined 294 players and determined that the biggest decline in motion occurred in players between 13-14 years old. In addition, they found that there is a linear decrease in range of motion as compared to age, but did not elucidate the cause.
Stretching, strengthening, and rehabilitation of shoulder dysfunction have been the mainstay for prevention of injury in many athletes. Kibler has written numerous articles outlining the importance for proper evaluation and treatment of shoulder injuries [10,11]. Therapy fundamentals include a proximal-to-distal framework with focus on proper scapular function before glenohumeral function. The importance of closed chain axial loading exercises for early shoulder rehabilitation is an essential component of a rehabilitation program. Litner et al., evaluated the effects of a stretching program for professional pitchers with GIRD [4]. The authors felt that GIRD is a soft tissue adaptation and, in their study, found that participation in an internal rotation-stretching program (cross-body posterior capsular stretch) can counteract the development of internal rotation deficit. Izumi et al., performed a cadaveric study on the effectiveness of stretches on the posterior capsule [6]. By evaluating 8 different stretching positions they postulated that internal rotation of the glenohumeral joint at 30° of elevation in the scapular plane provided the greatest stretch of the middle and lower capsule, while internal rotation at 30° of extension provided the greatest stretch of the upper and lower capsule.
We recognize that this study has limitations. First, there was no control group. With this additional information, we would be able to determine if our study population had an increased risk for development of GIRD as compared to the non-throwing athlete. Second, our study numbers were small. With a larger population, we might be able to determine if any other parameters would approach or become statistically significant. Thirdly, all of our participants swim for many hours each week. It is difficult to determine if their involvement in swimming has any role in their shoulder examination and further evaluation of age matched swimmers would help determine the role of swimming in the players’ development of GIRD. Another limitation of this study is the lack of analysis of intra-rater reliability and maybe a focus of future study. Finally, this was a single day study with a single measurement. This introduces measurement error and could be addressed by doing multiple measurements and averaging the results. Strengths of the study include elimination of measurement error by using a standardized, and well accepted, measurement technique with an evaluator doing the examination and a single sports medicine certified physical therapist measuring the motion. A further strength was the blinding of the evaluators to the players’ age, hours swimming, years playing, number of balls thrown per week, hand dominance, hours training, and DASH scores.
Conclusion
This is the first study to our knowledge evaluating glenohumeral internal rotation deficit in adolescent water polo players. The examinations showed that 14-62% of the participants met the definition for GIRD (depending on the definition utilized). Analysis of age, years playing, number of balls thrown per week, hours of swimming per week all showed no correlation with the development of GIRD in our population. The cause of GIRD in our population is unknown, however, increasing preseason-training hours approached correlation with GIRD, suggesting a possible causal relationship. In addition, evaluation of the DASH scores revealed no association with the development of GIRD. Further evaluation with a larger group may help elucidate risk factors for the development of GIRD in water polo players.
Previous studies evaluating GIRD in overhead throwing athletes indicate that rotational changes occur early in the athlete’s career. In addition, they stress that proper preseason preparation, identification of rotational limitations, and treatment of players with GIRD is important to help prevent injuries. Our study shows that there is a high prevalence of GIRD in adolescent water polo players in similar proportion to other adolescent and elite throwing athletes. The clinical significance of this finding is unclear in our population. It has been shown by others that by initiating internal rotation stretching exercises in overhead throwing athletes that the prevalence of GIRD can be decreased and this may have a role in adolescent water polo players.