I often get asked why I educate perioperative staff so much. Maybe it is because I am a surgical tech (I still scrub as much as I can overseas), maybe it is because I have found them to be some of the funniest, most resilient staff to interact with in my 20 years of being in the Operating Room. Maybe it is because teaching is good for my business; the relationships I form help sow the seeds for future revenue. These are all perks, but they aren’t why I do it. I do it because people are starving.
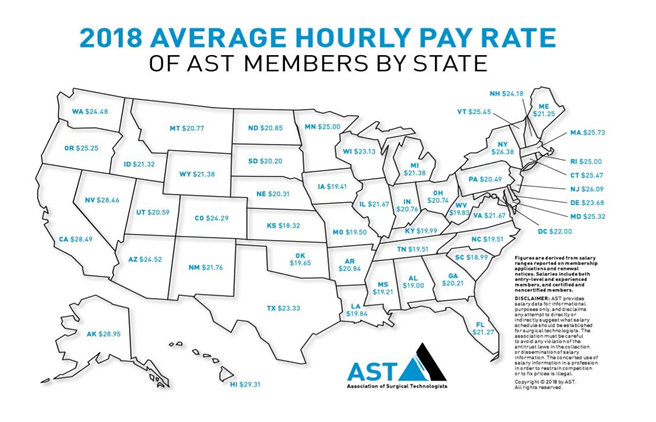
I don’t mean that as hyperbole, and I don’t mean that to be alarmist. I literally mean that some of your hospital staff, RIGHT NOW, cannot afford dinner. The Association of Surgical Technologists put out a map in 2018 of what average salaries looked like state-to-state:
In my state of California, the average pay for a surgical technologist is $28.49/hr. The lowest reported average was found in Kansas at $18.32/hr, though I have received reported lows of $13.78 (Altoona, PA).
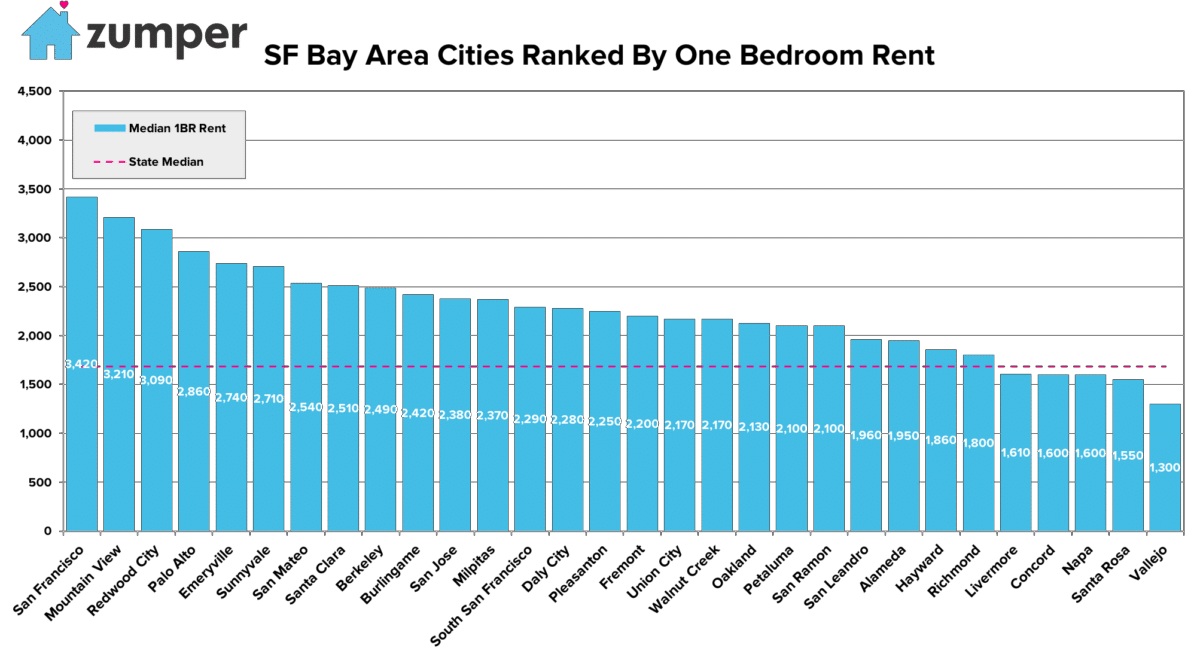
Now, $28.49/hr may sound like a decent amount of money to some, but when you consider that the median home price in California is $550,000 (zillow.com) and my current geographic region of the SF Bay Area actually has a median home price of well over $1M (zillow.com), it is no surprise that our Surgical Techs struggle to buy a home. So let’s forget about buying a home. What about rent? Check out the stats from 2017 for a one bedroom in the bay area:
That’s right. A one bedroom in the bay area can set you back as much as $3300/mo, while the mean for the state is still hovering around $1600/mo. This is probably why the poverty line in the bay area was adjusted to $117,400 by Housing and Urban Development (HUD) in 2018. So, if a CST in California is pulling down $28.49 @ 40 hours a week that equates to $54,700.80 gross. Let that sink in. The person that is asked to set up for surgery and keep a sterile field, understand and follow various types of surgical procedures and specialties, assist during complex and delicate operations, often cannot afford rent. Well below 50% of what is considered in poverty. Not “getting by”, poor.
If you are thinking, “well that’s no big deal, they can get a second job. Most surgical techs I know have more than one gig”, you’re right, but there are complications with that because of call responsibilities. When I was scrubbing I worked 12 hour shifts with a variable schedule, never working the same 3 days of the week. On top of that, call shifts demanded that I be available to the hospital even when I was off, leaving little flexibility to be committed to another facility. Mandatory overtime is also a reality. It happened to me more than once; that nightmare scenario at the end of a 12-hour shift where the night tech calls in sick, and I am not allowed to leave. We were a trauma center; it was mandatory to stay in order to care for patients. Hello overtime, goodbye family and sleep.
With the unpredictable reality of working in an operating room, the only options for people who work multiple jobs are to go per diem (forfeit benefits, lessen commitment to facility), work in surgery centers (usually lower pay, no call), or try and coordinate less call (a financial hit). None of these are optimal; in a perfect world we would just pay surgical techs a living wage.
So, why do I teach so much? Because on top of all of this stress, Surgical Techs are expected to follow the RN model of keeping up their certification through Continuing Education Units (CEU) or re-testing. Certified Surgical Technologists are required to submit 30 CEU every 2 years (effective Jan 2020, https://www.nbstsa.org), and those all cost money if not supplied by their hospital through in-services. If they choose to re-certify by taking their test over again with the Association of Surgical Technologists (AST), the fee is $399 for active members ($80 membership), or $499 for non-members. I have heard comments from techs I work with grappling with whether to pay rent, or re-certify.
As an Orthopedic trauma rep with a passion for education and deep ties to the OR community, I take it on as a personal duty to supply these critical staff members with free CEU, a hot breakfast, and knowledge that they can take with them for the length of their careers. Knowledge isn’t just power, it’s a lifeline. So, as a medical device professional that doesn’t educate (I admit, it isn’t for everyone) or a surgeon/administrator, why does this financial context matter?
Know your audience. The financial struggles of Surgical Techs often go unspoken and unseen. It gets swept under the rug because it can be an uncomfortable power dynamic. I remember vividly being a young surgical tech and getting harshly criticized by a surgeon for filling up a syringe to the full 10cc; he wanted it filled to 7cc. The surgeon stated that the full 10cc made his hand stretch too much, saying “this is what you get paid for, can’t you see how hard I’m straining? Pay more attention!!”. It was my first time working with him. He then bought a pony in between cases (seriously...it was for his daughter, and coordinated the sale over the phone while I turned over the room. We waited for 30 minutes for him to finish the purchase). He came back and complained about the logistics of having to transfer thousands of dollars over for the transaction. I was just hoping I had enough gas in my tank to come back later that night if I got called in on my call shift. Surgeons deserve to make what they make, but the discrepancy in compensation does require some awareness to have a harmonious team. So, the next time you are about to discuss the high-priced repair for your car, or the irritation that you experienced with logistics on your vacation, consider some of the quotes below I have heard from Surgical Techs; the people next to you passing sutures, holding down sterility, and turning your room over: “I had to take $10 out of savings to by eggs, bread, and milk”, “Got extra at lunch and took it home for dinner. Gotta feed the fam somehow” “Many times I have stolen a muffin from the doctor’s lounge so my kid has breakfast in the am. I’ve gotten myself used to surviving on a cereal that again, I stole, in the am and no lunch or dinner. I’ll be ok but my kid has to eat. Single mom without life support right here”
Don’t apologize for what you earn, but be self-aware, and be an advocate.
Figures
Julia Greenspan, Santa Cruz De La Sierra, Bolivia Medical Mission 2019