Localised, Isolated Amyloidosis of the Nose and Paranasal Sinuses
*Corresponding Author(s):
Polina IvanovaDepartment Of Ent, University Hospital Saint Marina, Medical University Of Varna, Varna, Bulgaria
Tel:+35 9896863941,
Email:ppivanovax@gmail.com
Abstract
Amyloidosis is mainly a systemic disease, hence primary localised amyloidosis of the nose and sinuses may occur. Symptoms may include epistaxis, nasal obstruction, facial deformity and vision changes.
We present a case of isolated, localised sinonasal amyloidosis in 81-year old woman and a brief literature review. After an extensive evaluation process and a histology verification the final diagnosis was concluded - sinonasal amyloidosis. Treatment with radiotherapy showed excellent outcomes as the process was halted and the patient reported improved breathing.
Localised amyloidosis is a benign, slowly growing process. Although it is a rare condition, nasal amyloidosis must be considered in the differential diagnosis of nasal obstruction.
Keywords
INTRODUCTION
CASE REPORT

Figure 1: Image of patient’s face deformity regarding the nasal bridge.
The evaluation process included routine blood test, which did not present anything abnormal. Anterior rhinoscopy revealed a bulging mass engaging the nasal meat uses. Further, a Computed Tomography (CT) scan was appointed. The findings showed an advanced neo-process, presenting as heterogeneous mass, engaging the nasal meat uses at the level of the middle and superior turbinates, spreading along the frontal sinuses, with destruction of the base of the latest, an osteolysis of the nasal bones bilaterally and the anterior walls of the anterior ethmoidal sinuses, and a suspicion for the zone of destruction in the medial wall of the right orbit (Figure 2). For further diagnostics, a biopsy was performed under endoscopic control and local anaesthesia with 2% Lidocaine. The histological examination displayed fragmented parts of tissue with respiratory epithelium, sub mucosal diffuse deposits of eosinophilic, amorphous fissured material, consistent with an amyloid structure; a periglandullar inflammation (Figure 3). Further investigations performed by the internal medicine specialists did not show systemic involvement.
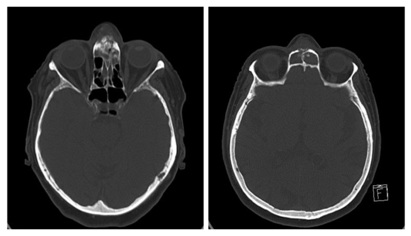
Figure 2 (left): Axial CT image of the patient showing engagement of the nasal meat uses.
Figure 2 (right): Axial CT image of the patient showing engagement of sinus frontal is with osteolysis.
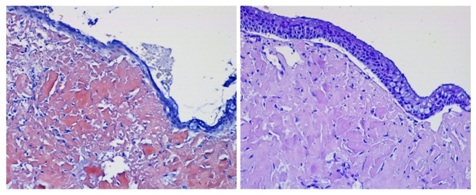
Figure 3 (left): Histology of amyloidosis from tissue section from the nasal meat uses after straining with Congo × 100.
Figure 3 (right): Histology of amyloidosis from tissue section from the nasal meat uses after straining with H&E × 100.
RESULTS
The patient received a full course of external beam radiotherapy with a total amount of 36 Grey. A following CT-scan was performed 9 months after the diagnosis and the treatment with radiation. The findings revealed no enlargement of the process. External radiotherapy appears to halt the progression of isolated localised sinonasal amyloidosis. The patient also reported improved nasal breathing.
DISCUSSION
Amyloidosis is a rare disease with an incidence of 12 cases per million populations per year [2]. The main subtypes of amyloidosis are primary AL amyloidosis, secondary Amyloid A (AA) amyloidosis, familial amyloidosis, and ß2-microglobulin-related amyloidosis. The diagnosis of amyloidosis is based on clinical organ involvement and histological evidence of amyloid deposits [3].
Rarely, however, amyloidosis may be present in a localised form. When occurring on a localised basis in the head and neck region, it can involve the orbit, sinuses, nasopharynx, oral cavity and larynx, the latter of which is the most common head and neck presentation of localised amyloidosis.
Isolated local nasal amyloidosis is extremely rare and idiopathic. In the literature are reported very few cases regarding localised nasal amyloidosis. The youngest patient described in the literature that we occurred with localised nasal amyloidosis was 8 years old, whereas our patient is one of the oldest with the age of 81 years [4]. Another young female patient was at the age of 14 years [5]. A clear definition, in reference with age group or gender predominance, has not been found yet. As seen from the previous cases every age group may be affected by the disease.
With so few information from the literature review, little is known of this specific condition, its aetiology and the initial factors. Given that the most common localization of localised amyloidosis is at mucous membranes in contact with the environment, it has been suggested there is an antigenic induction of amyloidogenic plasma cell clones [6]. A chronic inflammation has often been encountered also as an etiological factor [7].
Localised amyloidosis usually presents as one solitary volume occupying lesion, although multiple nodules may appear. The symptoms may vary depending on location of the formation. In its localised form amyloidosis resembles a malignant process. Calcifications are also common, radiologic appearance may include micro calcifications, increasing the suspicion of malignancy. In sinonasal amyloidosis symptoms usually are unspecific such as nasal obstruction, recurrent epistaxis, mucoid discharge, Eustachian tube disorder, facial deformity, as in our case the patient the complaints were nasal obstruction and facial deformity. Localised AL amyloidosis can be treated with radiation therapy and depending on the localisation; some forms may be amenable to surgery. The overall survival of localised AL amyloidosis is excellent and strikingly different from systemic AL amyloidosis. Progression to systemic disease is an exceptionally rare occurrence [8].
CONCLUSION
CONSENT
ACKNOWLEDGEMENT
CONFLICT OF INTEREST
REFERENCES
- Kasper DL, Fauci AS, Hauser SL, Longo DL, Jameson JL, et al. (2015) Harrison’s principles of internal medicine. (19th edn). McGraw Hill Education, New York, USA.
- Khan MF, Falk RH (2001) Amyloidosis. Postgraduate Medical Journal 77: 686-693.
- Real de Asúa D, Costa R, Galván JM, Filigheddu MT, Trujillo D, et al. (2014) Systemic AA amyloidosis: Epidemiology, diagnosis, and management. Clin Epidemiol 6: 369-377.
- Mufarrij AA, Busaba NY, Zaytoun GM, Gallo GR, Feiner HD (1990) Primary localised amyloidosis of the nose and paranasal sinuses. A case report with immunohistochemical observations and a review of the literature. Am J SurgPathol 14: 379-383.
- Nakayama, Otori N, Komori M, Takayanagi H, Moriyama H (2012) Primary localised amyloidosis of the nose. Auris Nasus Larynx 39: 107-109.
- Krishnan J, Chu W, Elrod JP, Frizzera G (1993) Tumoural presentation of amyloidosis (amyloidomas) in sof tissues. A report of 14 cases. Am J Clin Pathol 100: 135-144.
- Toyoda M, Ebihara Y, Kato H, Kita S (1993) Tracheobronchial AL amyloidosis: Histologic, immunohistochemical, ultrastructural, and immunoelectron microscopic observations. Hum Pathol 24: 970-976.
- Mahmood S, Sachchithanantham S, Bridoux F, Lane T, Rannigan L, et al. (2013) Risk of progression of localised amyloidosis to systemic disease in 606 patients over 30 years. Blood Nov 122: 3143.
Citation: Iliev G, Ivanova P, Kerimov K, Genova P, Kalchev K (2019) Localised, Isolated Amyloidosis of the Nose and Paranasal Sinuses. J Otolaryng Head Neck Surg 5: 025.
Copyright: © 2019 Georgi Iliev, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.