Rehabilitation Services, Self-Advocacy and Psychosocial Adaptation as Determinants of Employment among Persons with Spinal Cord Injury
*Corresponding Author(s):
Veronica I UmeasiegbuSchool Of Rehabilitation Services And Counseling, College Of Health Affairs, University Of Texas Rio Grande Valley, Texas, United States
Tel:+1 9566652949,
Email:veronica.umeasiegbu@utrgv.edu
Abstract
Objectives
The purpose of this study was to investigate the factors that determine employment in adults with Spinal Cord Injury (SCI).
Methods
Participants were community-dwelling adults with SCI from three states of the United States. Participants included 101 adults who have lived with SCI for at least one year before the onset of the study. Cross-sectional design through the use of questionnaire was used in this research. Participants were recruited through purposive sampling. Descriptive analysis, correlation analysis, regression analysis, and path analysis were used to analysis the study data.
Results
The results of this study suggest that age, education, and psychosocial adaptation are the predictors of employment in this sample of persons with SCI.
Keywords
INTRODUCTION
Employment is central and critical for overall wellbeing of individuals. The significance of employment to life satisfaction has been found to be a critical factor to adjustment after a disability [4]. Historically, employment of persons with disabilities in general, and among people with SCI in particular, is considered an important rehabilitation goal, although difficult to achieve. For persons with SCI, employment is fundamental to regaining their lives after the injury. According to research, [5-7] return to work by persons with SCI is regarded a mark of successful rehabilitation and adjustment to the disability. Despite the importance and need for participation in the community such as in employment multiple barriers hinder such essential activity. These barriers to employment of persons with SCI include functioning limitations due to the SCI, negative societal attitudes toward disabilities, psychological and adjustment issues related to the disability [8], and lack of appropriate type of rehabilitation services (such as self-advocacy skills training; Umeasiegbu [7]). According to Craig, Perry, Guest, Tran, and Middleton [9] “restrictions in social participation can become significant barriers to employment or educational activity”.
Despite the importance of employment to overall wellbeing and high unemployment rate among individuals with SCI, little research attention has been committed to understanding the interactions between multiple environmental and personal factors such as rehabilitation services, self-advocacy, and psychosocial adaptation and how these factors facilitate or hinder employment of individuals with SCI. For example, very little is known about the impacts of self-advocacy after SCI. The unsatisfactory participation in employment calls for re-evaluation of the rehabilitation services that individuals with SCI receive after their injury and how rehabilitation outcomes can be improved. The objective of this study was to explore the associations between multiple variables (demographic characteristics, SCI-related variables, and rehabilitation-related variables) and employment among a sample of persons with SCI. The following research questions were investigated in this study:
1. What associations exist between SCI-related variables (level of injury, SCI-complications, use of wheelchair) and rehabilitation-related variables (received rehabilitation services, self-advocacy, and psychosocial adaptation) and employment among persons with SCI?
2. What demographic characteristics of persons with SCI predict employment among a sample of persons with SCI?
MATERIALS AND METHODS
Study design
Procedure
Instruments and measures
| Education | |||||
| Vocational/Technical School | Some College/Associate Degree | College Graduate | |||
| Gender | Male | Count | 2 | 20 | 12 |
| % within gender | 3.20% | 32.30% | 19.40% | ||
| % within education | 28.60% | 66.70% | 60.00% | ||
| % of total | 2.00% | 20.00% | 12.00% | ||
| Female | Count | 5 | 10 | 8 | |
| % within gender | 13.20% | 26.30% | 21.10% | ||
| % within education | 71.40% | 33.30% | 40.00% | ||
| % of total | 5.00% | 10.00% | 8.00% | ||
| Total | Count | 7 | 30 | 20 | |
| % within gender | 7.00% | 30.00% | 20.00% | ||
| % within education | 100.00% | 100.00% | 100.00% | ||
| % of total | 7.00% | 30.00% | 20.00% | ||
Community integration questionnaire
Self-advocacy questionnaire
Disability centrality scale
Received rehabilitation services scale
Data analysis
RESULTS
Descriptive statistics
| Characteristic | N | (%) | |
| Current age category | |||
| 21-29 | 9 | 8.9 | |
| 30-39 | 20 | 20 | |
| 40-49 | 21 | 21 | |
| 50-59 | 26 | 26 | |
| 60-69 | 16 | 16 | |
| 70 or older | 9 | 8.9 | |
| Age at injury category | |||
| 18-20 | 20 | 20 | |
| 21-29 | 28 | 28 | |
| 30-39 | 14 | 14 | |
| 40-49 | 16 | 16 | |
| 50-59 | 14 | 14 | |
| 60-69 | 4 | 4 | |
| 70 or older | 4 | 4 | |
| Gender | |||
| Male | 63 | 62 | |
| Female | 38 | 38 | |
| Race/Ethnic group | |||
| White | 84 | 84 | |
| African American | 13 | 13 | |
| Native American/American Indian/Alaskan natives | 1 | 1 | |
| Others | 2 | 2 | |
| Marital status | |||
| Married | 48 | 50 | |
| Never married | 30 | 31 | |
| Divorced | 6 | 6.2 | |
| Widowed | 8 | 8.2 | |
| Living with partner/significance other | 5 | 5.2 | |
| Education | |||
| 9th grade or less | 1 | 1 | |
| Grades 10-12 (some high school) | 5 | 5 | |
| High school graduate/GED | 20 | 20 | |
| Vocational/technical school | 7 | 6.9 | |
| Some college/associate degree | 30 | 30 | |
| College graduate | 20 | 20 | |
| Graduate school or professional school | 18 | 18 | |
| Residential location | |||
| Urban | 17 | 18 | |
| Suburban | 38 | 40 | |
| Rural | 40 | 42 | |
| Employment at injury | |||
| Full-time | 62 | 61 | |
| Part-time | 9 | 8.9 | |
| Student | 18 | 18 | |
| Unemployed (not student, not retired) | 9 | 9 | |
| Retired | 3 | 3 | |
| Employment after injury | |||
| Full-time | 17 | 17 | |
| Part-time | 11 | 11 | |
| Student | 3 | 3 | |
| Unemployed (not student, not retired) | 48 | 49 | |
| Retired | 20 | 20 | |
| Level of Injury | |||
| Cervical 1 (C1)-Cervical 3 (C3) | 10 | 9.9 | |
| C3-C7 | 36 | 36 | |
| Thoracic 1 (T1)-Thoracic 5 (T5) | 12 | 12 | |
| T6-T12 | 38 | 38 | |
| Lumbar region | 5 | 5 | |
| SCI-related complications | |||
| Pressure ulcer | 31 | 31 | |
| Low blood pressure | 15 | 15 | |
| Depression | 41 | 41 | |
| Infections | 37 | 37 | |
| Bowel and bladder problems | 64 | 63 | |
| Sexual dysfunction | 38 | 38 | |
| Pain | 65 | 64 | |
| Spasticity | 56 | 55 | |
| Respiratory problems | 6 | 5.9 | |
| Osteoporosis | 17 | 17 | |
| Diabetes | 1 | 1 | |
| Years since injury | |||
| 1-3 years | 12 | 12 | |
| 4-6 years | 22 | 22 | |
| 7-10 years | 20 | 20 | |
| 11-15 years | 15 | 15 | |
| 16 years and over | 31 | 31 | |
| Count | ||||
| Gender | Total | |||
| Male | Female | |||
| Emp at injury | Employed full-time (more than 30 hours a week) | 39 | 23 | 62 |
| Employed part-time (less than 30 hrs a week) | 7 | 2 | 9 | |
| Volunteer employment | 0 | 1 | 1 | |
| Unemployed, seeking employment | 3 | 0 | 3 | |
| Unemployed, not seeking employment | 2 | 2 | 4 | |
| Student | 10 | 7 | 17 | |
| Homemaker (manage home/family) | 0 | 1 | 1 | |
| Retired | 1 | 2 | 3 | |
| Employ Yes 1 no 0 | Total | ||||
| No | Yes | ||||
| Gender | Male | Count | 44 | 18 | 62 |
| % within gender | 71.00% | 29.00% | 100.00% | ||
| % within employ yes 1 no 0 | 60.30% | 66.70% | 62.00% | ||
| % of total | 44.00% | 18.00% | 62.00% | ||
| Female | Count | 29 | 9 | 38 | |
| % within gender | 76.30% | 23.70% | 100.00% | ||
| % within employ yes 1 no 0 | 39.70% | 33.30% | 38.00% | ||
| % of total | 29.00% | 9.00% | 38.00% | ||
| Total | Count | 73 | 27 | 100 | |
| % within gender | 73.00% | 27.00% | 100.00% | ||
| % within employ yes 1 no 0 | 100.00% | 100.00% | 100.00% | ||
| % of total | 73.00% | 27.00% | 100.00% | ||
Correlation analysis
| Measure | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
| LI | ||||||||||
| WC | 0.372** | |||||||||
| Emp-FT | -0.038 | 0.039 | ||||||||
| DCS | -0.161 | -0.033 | 0.313** | |||||||
| Comp | 0.048 | -0.084 | -0.201* | -0.504** | ||||||
| SAQ | 0.039 | 0.048 | 0.171 | 0.499** | -0.193 | |||||
| RSR | -0.057 | 0.174 | 0.217* | 0.265* | 0.014 | 0.241** | ||||
| CIQH | 0.049 | 0.183 | 0.207* | 0.200* | -0.246* | 0.134 | -0.024 | |||
| CIQS | -0.007 | -0.039 | -0.057 | -0.224** | 0.172 | -0.194 | -0.212* | -0.19 | ||
| CIQPD | 0.071 | 0.115 | .611** | 0.333** | -0.251* | 0.161 | 0.168 | 0.301** | -0.134 | |
| CIQ Total | 0.09 | 0.189 | 0.396** | 0.217* | -0.212* | 0.088 | -0.037 | 0.739** | 264** | 0.659** |
**p = 0.01, *p = 0.05
Reliability analysis
| Variable | No of Items | Cronbach’s Alpha |
| SAQ | 11 | 0.88 |
| RRSS | 9 | 0.84 |
| CIQ | 14 | 0.7 |
| DCS | 10 | 0.89 |
Path analysis
Research question 1 was investigated using path analysis. The researchers hypothesized that all the selected variables; level of injury, SCI-complications, use of wheelchair, received rehabilitation services, self-advocacy, and psychosocial adaptation will have direct association with employment after SCI. The results of several re-specifications of the hypothesized associations are represented in figure 1. After the re-specification of this model, the chi square test became nonsignificant (?2 (5) = 4.597, p = 0.467). The CFI = 1.000; TLI = 1.022, and RMSEA = 0.000, indicating that this model represents a good fit to the data. The re-specified model is shown in figure 1.
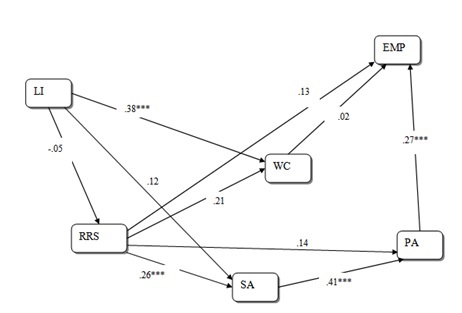
Note: LI = Level of Injury; RRS = Received Rehabilitation Services; WC= Wheelchair Use; SA = Self-Advocacy; PA = Psychosocial Adaptation; EMP = Employment
Regression analysis
DISCUSSION
Rehabilitation services, self-advocacy, psychosocial adaptation, and employment
A surprising result of this study is the lack of association between level of injury and employment. A review of the literature shows that several past studies had inconsistency in the reported relationships between severity of injury and employment. In some studies, it was reported that employment is not dependent on severity of injury [24,25], while in others contrary results were reported [26,27]. Since there is no consensus in the literature on the relationship between level of injury and employment, it is possible that there are some other unidentified variables that either mediate or moderate this relationship in certain situations. In this current study level of injury had a strong effect on wheelchair use, although this study did not explore details about this relationship such as whether this relationship differs between users of motorized wheelchairs and manual wheelchairs.
Strong positive associations are noted between received rehabilitation services and self-advocacy; between self-advocacy and psychosocial adaptation; and between psychosocial adaptation and employment. In the past, rehabilitation researchers have suggested that psychosocial adaptation to disability and chronic illness has a relationship with Quality of Life (QOL) [28-30]. In a study Livneh and Martz [31] posit that coping strategies and coping resources increase psychosocial adaptation to SCI. The findings of this current study aligns with previous literature. Particularly, the findings of our study suggest that self-advocacy (a form of coping strategy) has a direct association to psychosocial adaptation. This study has shown that since psychosocial adaptation correlates positively with both self-advocacy and employment; psychosocial adaptation can directly or indirectly increase community participation and hence QOL of persons with SCI. In other words, an individual with increased self-advocacy skills may adapts better to psychosocial impacts of SCI. Increased psychosocial adaptation will more likely lead to employment and employment retention, and hence increase in QOL.
This study suggests a strong positive association between received rehabilitation services and self-advocacy (see Figure 1). Received rehabilitation services also show minimal positive associations with wheelchair use, psychosocial adaptation, and employment. These minimal associations should be interpreted with caution due to small sample size and the self-report nature of the study. These associations underscore the importance of rehabilitation during inpatient and outpatient phases of SCI to employment post SCI. Unfortunately, very little is known in the research literature on comprehensive rehabilitations needs of individuals with SCI or the impacts of rehabilitation services on community participation such as employment of persons with SCI. According to Gutenbrunner, Blumenthal, Geng, and Egen [32] individuals with SCI need long term rehabilitation services that is interdisciplinary in nature. Such rehabilitation services include services that address community re-entry issues such as assistive technology, mental health issues, vocational rehabilitation, education, adaptation to living environment, and others. The results of this current study suggest that rehabilitation professionals who work with persons with SCI need to consider a wide range of variables in both acute and post-acute phases of rehabilitation in order to promote community participation such as employment. Exploring the relationships between this study’s variables (level of injury, SCI-related complications, and wheelchair use, self-advocacy, psychosocial adaptation, employment, received rehabilitation services, and community reintegration) in rehabilitation process can facilitate and increase positive rehabilitation outcomes. The results of this study can be valuable in addressing the psychosocial concerns of persons with SCI by rehabilitation counselors and other rehabilitation professionals. Areas of to focus on can include case management, self-advocacy training, vocational service, and adjustment counseling.
Demographic variables as predictors of employment
Furthermore, several prior studies have found a wide range of demographic variables to predict employment status. These variables include age, level of education, gender, severity of injury, and marital status [37-39]. With the exception of age and education, these demographic variables were not predictive of employment in this current study. James, DeVivo, and Richards [40] found a relationship between race and gender in employment; their study reported that White women were less likely than White men to be employed, whereas African American women were more likely than African American men to be employed. The inability of other demographic information to predict employment in this study could be the result of the small sample size (n = 101). Education is a key determinant of economic independence and quality of life. According to NSCISC (2016), “over half of persons with SCI are high school graduates (51.5%) at time of their injury” (p. 2). The report of the NSCISC is consistent with the finding in this study; 59.5% of the participants of this study have at least a high school diploma at the time of injury. According to Bryce et al., [41] “education has been found to be the factor most strongly associated with post injury employment. Only 5% of persons in the National SCI Database with less than 12 years of education were found to be employed” (p. 1315) compared to 68.8% among individual with SCI who had doctoral degrees.
LIMITATIONS
CONCLUSION
ACKNOWLEDGMENT
REFERENCES
- National Spinal Cord Injury Statistical Center (2016) Facts and figures at a glance. National Spinal Cord Injury Statistical Center, Birmingham, UK.
- Blake J, Brooks J, Greenbaum H, Chan F (2017) Attachment and employment outcomes for people with spinal cord injury: The intermediary role of hope. Rehabilitation Counseling Bulletin 60: 77-87.
- Richards JS, Kewman DG, Richardson E, Kennedy P (2010) Spinal cord injury. Frank RG, Rosenthal M, Caplan B (eds.). Handbook of rehabilitation psychology, Washington, D.C., USA.
- Crewe NM, Krause JS (2002) Spinal cord injuries. In: Brodwin MG, Tellez F, Brodwin SK (eds.). Medical, Psychosocial and Vocational Aspects of Disability (2nd edn). Elliott & Fitzpatrick, Inc, Attens, Georgia.
- Krause JS (1996) Employment after spinal cord injury: Transition and Life adjustment. Rehabilitation Counseling Bulletin 39: 244-255.
- Krause JS, Saunders L, Stalen D (2010) Race-ethnicity, education, and employment after spinal cord injury. Rehabilitation Counseling Bulletin 53: 78-86.
- Umeasiegbu VI (2013) Exploring the Use of the International Classification of Functioning, Disability and Health as a Community Reintegration Model After Spinal Cord Injury. University of Kentucky, Kentucky, USA.
- Yuen HK, Wolf BJ (2010) Factors that limit access to dental care for adults with spinal cord injury. Spec Care Dentist 30: 151-156.
- Craig A, Perry KN, Guest R, Tran Y, Middleton J (2015) Adjustment following chronic spinal cord injury: Determining factors that contribute to social participation. Br J Health Psychol 20: 807-823.
- Kline RB (2005) Principles and Practice of Structural Equation Modeling, (2nd edn), Guilford Press, New York, USA.
- Kline RB (2011), Principles and Practice of Structural Equation Modeling (3rd edn), Guilford Press, New York, USA.
- Chan F, Lee GK, Lee E, Kubota C, Allen CA (2007) Structural equation modeling in rehabilitation counseling research. Rehabilitation Counseling Bulletin 51: 53-66.
- Weston R, Gore Jr PA, Chan F, Catalano D (2008) An introduction to using structural equation modelings in rehabilitation psychology. Rehabilitation Psychology 53: 340-356.
- Wolf EJ, Harrington KM, Clark SL, Miller MW (2013) Sample size requirements for structural equation models: an evaluation of power, bias, and solution propriety. Educ Psychol Meas 76: 913-934.
- Schumacker RE, Lomax RG (2010) A Beginner's Guide to Structural Equation Modeling. Routledge, New York, USA.
- Willer B, Rosenthal M, Kreutzer J, Gordon WA, Rempel R (1993) Assessment of community integration following rehabilitation for traumatic Brain inj 8: 75-87.
- Gontkovsky ST, Russum P, Stokic DS (2009) Comparison of the CIQ and chart short form in assessing community reintegration in individuals with chronic spinal cord injury: A pilot study. Neuro Rehabilitation 24: 185-192.
- Hirsh AT, Braden AL, Craggs JG, Jensen MP (2011) Psychometric properties of the community integration questionnaire in a heterogeneous sample of adults with physical disability. Arch Phys Med Rehabil 92: 1601-1610.
- Adams KS (2007) Visibility of disability, attritional style, psychosocial adjustment to disability, and self-advocacy skill in relation to student adaptation to college. Florida State University Pro-Quest Database.
- Bishop M (2005) Quality of life and psychosocial adaptation to chronic illness and disability: Preliminary analysis of a conceptual and theoretical synthesis. Rehabilitation Counseling Bulletin 48: 219-231.
- 21. Bishop M, Shepard L, Stenhoff DM, Shepard L (2007) Psychosocial adaptation and quality of life in multiple sclerosis: Assessment of the disability centrality model. Journal of Rehabilitation 73: 3-12.
- Bishop M, Frain MP, Tschopp MK (2008) Self-management, perceived control and subjective quality of life in multiple sclerosis: An exploratory study. Rehabilitation Counseling Bulletin.
- Hatcher L (2013) Advanced Statistics in Research: Reading, Understanding, and Writing Up Data Analysis Results. Shadow Finch Media, Saginaw, USA.
- Krause JS, Crewe NM (1990) Long-term prediction of self-reported problems following spinal cord injury. Paraplegia 28: 186-202.
- Wang RY, Yang YR, Yen LL, Lieu FK (2002) Functional ability, perceived exertion and employment of the individuals with spinal cord lesion in Taiwan. Spinal Cord 40: 69-76.
- Krause JS, Broderick LE, Saladin LK, Broyles J (2006) Racial disparities in health outcomes after spinal cord injury: Mediating effects of education and income. J Spinal Cord Med 29: 17-25.
- Young ME, Alfred W (1994) Vocational status of persons with spinal cord injury living in the community. Rehabilitation Counseling Bulletin 37: 229-244.
- Livneh H, Bishop ML (2012) The psychological impact of chronic illness and disability. In: Parker RM, Patterson JB (eds.). Rehabilitation Counseling: Basics and Beyond (5th edn), Pro-ED, Texas, USA.
- Livneh H, Martz E, Wilson LM (2001) Denial and perceived visibility as predictors of adaptation to disability among college students. Journal of Vocational Rehabilitation 16: 227-234.
- Viney LL, Westbrook MT (1982) Patients’ psychological reactions to chronic illness: Are they associated with rehabilitation? Journal of Applied Rehabilitation Counseling 13: 38-44.
- Livneh H, Martz E (2014) Coping strategies and resources as predictors of psychosocial adaptation among people with spinal cord injury. Rehabil Psychol 59: 329-339.
- Gutenbrunner C, Blumenthal M, Geng V, Egen C (2017) Rehabilitation Services Provision and Payment. Am J Phys Med Rehabil 96: 35-40.
- Ramakrishnan K, Mazlan M, Julia PE, Latif LA (2011) Return to work after spinal cord injury: factors related to time to first job. Spinal Cord 49: 924-927.
- Reinhardt JD, Post MW, Fekete C, Trezzini B, Brinkhof MW (2016) Labor market integration of people with disabilities: Results from the Swiss spinal cord injury cohort study. PLos One 11:0166955.
- Tsai IH, Graves DE, Chan W, Darkoh C, Lee MS, et al. (2017) Environmental barriers and social participation in individuals with spinal cord injury. Rehabil Psychol 62: 36-44.
- Crewe NM (2000) A 20-year longitudinal perspective on the vocational experiences of persons with spinal cord injury. Rehabilitation Counseling Bulletin 43: 122-133.
- DeVivo M, Fine P (1982) Employment status of spinal cord injured patients 3 years after injury. Arch Phys Med Rehabil 63: 200-203.
- Hess D, Ripley D, McKinley W, Tewksbury M (2000) Predictors for return to work after spinal cord injury: a 3-year multicenter analysis. Arch Phys Med Rehabil 81: 359-363.
- Krause J, Sternberg M, Maides J, Lottes S (1998) Employment after spinal cord injury: differences related to geographic region, gender, and race. Arch Phys Med Rehabil 79: 615-624.
- James M, DeVivo MJ, Richards JS (1993) Postinjury employment outcomes among African-American and White persons with spinal cord injury. Rehabilitation Psychology 38: 151-164.
- Bryce TN, Ragnarsson KT, Stein AB (2007) Spinal cord injury. In: Braddom RL (ed.). Physical Medicine and Rehabilitation (3rd edn), Saunders Elsevier, Philadelphia, USA.
Citation: Umeasiegbu VI, Bishop ML (2017) Rehabilitation Services, Self-Advocacy and Psychosocial Adaptation as Determinants of Employment among Persons with Spinal Cord Injury. J Phys Med Rehabil Disabil 3: 020.
Copyright: © 2017 Veronica I Umeasiegbu, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.