Prevalence of Respiratory Disorders among Woodworkers in Jimma Town, Southwest Ethiopia
*Corresponding Author(s):
Wondu Reta DemissieDepartment Of Biomedical Sciences, School Of Medicine, Institute Of Health, Jimma University, Jimma, Ethiopia
Tel:+251913988722,
Email:majore04@gmail.com
Abstract
Wood dust is one of the most common sources of occupational exposures in the world. Occupational exposure to wood dust inhalation results in respiratory disorders. Jimma was the endemic and pioneer of different wood and wood products that creates work opportunity for many individuals but, simultaneous exposure to different respiratory impairments was inevitable.
Objective
The aim of the present study was to assess the prevalence of respiratory disorders among woodworkers in Jimma town, Ethiopia, 2018 G.C.
Method
A community based comparative cross-sectional study was conducted among woodworkers and non-woodworkers in Jimma town, 2018 G.C. Multistage random sampling technique was used to select the exposed study group and convenience sampling technique was used to select the non-exposed group. Spirometer and clinical presentation was used to identify respiratory disorders. A total of 140 study participants were enrolled in the study. Data were checked for completeness, entered into Epi data version 1.7 and exported to SPSS version 20 for further analysis. Descriptive statistics were computed and results were presented with narratives, tables or figures.
Results
The magnitudes of ventilatory impairments were higher among exposed group (44.2%) than non-exposed group (14.3%) specifically identified as restrictive disease (20% and 6.8%), obstructive disease (17.1% and 5.7%) and mixed pattern (7.1% and 0%] among woodworkers and control group respectively.
Conclusion:
In general the prevalence of respiratory disorders/ventilatory impairments was diagnosed among 41 respondents (29.3%) while the left 99 (70.7%) considered as normal pulmonary function. The burdens of respiratory disorders were higher (44.2%) among woodworkers when compared with control group (14.3%).
Keywords
INTRODUCTION
Among the identified occupational hazards, exposure to wood dust is responsible for development of varies respiratory disease [2]. Two million workers worldwide are regularly exposed to wood dust in the work place and claims for respiratory disorders [3-6].
Dusts from the wood and its components (cellulose, hemicellulose,lignin ,organic and inorganic compoundslike terpenes and its derivatives such as abietic acid, phenolic compounds, tannins, stilbenes and glycosides) are known for their sensitizing and irritating properties of the mucous membrane and evokes asthma [7,8]. Inhalation of dust via respiratory system accessed to the airways, airways epithelial cells, activate macrophages, dendritic cells and innate immune cells; then initiate responses in various populations of specific immune cells such as T helper cells, T cytotoxic cells and B cells; initiation of inflammatory immune responses, activation of immune cells and releases of many cytokines, chemokines and other inflammatory molecules with variable pathologic effects on lung to cause different respiratory diseases[8-11].
COPD is one of the chronic non communicable disease occurred associated with work related condition including exposure to wood dust [12-14].
There was also evidence of increased risk of lung cancer among workers with substantial cumulative exposure to wood dust [15,16].
Though limited, there are studies conducted in Jimma town to assess the magnitude work related respiratory disorders and the complex of diseases with comorbidities [17-20].But there is no any study conducted among woodworkers in Jimma town and Ethiopia further to assess respiratory disorders to our knowledge yet. Thus, the present study was aimed to assess the magnitude of respiratory disorders among woodworkers by taking the reference group from shop workers.
MATERIALS AND METHODS
Study area and period
According to Jimma town entrepreneur and food security agency in 2017/2018 report, there are 300 small-scale wood processing industries in the town involving 1012 male and 548 female woodworkers. The data was collected from April 5 to May 3, 2018 G.C among sampled woodworkers and non-exposed group (shopkeepers) for comparison by employing comparative cross-sectional study design.
Selection criteria
All individuals of both groups (exposed and non-exposed) with history of pulmonary tuberculosis, heart failure, common cold, history of smoking, any acute illness were excluded from the study as it affects the results of dynamic pulmonary function tests measured by spirometer.
Sample size determination
Sampling technique
Data collection tools and procedures
Airflow obstruction: was defined as FEV1 /FVC <70% and FVC (predicted) >80% [22,23].
COPD:is considered in any patient with dyspnea, chronic cough or sputum production, and/or a history of exposure to risk factors and diagnosed byspirometer result ofa post-bronchodilator FEV1/FVC < 0.70 [22,23]. It is characterized as onset in midlife, symptoms slowly progressive, long history of tobacco smoking, dyspnea during exercise largely irreversible airflow limitation [24].
Asthma: refers to a generalized obstruction of airways that caused by inhalation of substances at work place which usually reversible. Its onset is early in life (often childhood) with symptoms vary from day to day (at night/early morning), allergy, rhinitis, and/or eczema, family history of asthma [25,26].
Airflow restriction: was defined as FVC <80% predicted value and FEV1/FVC >70% [23,27].
Mixed pattern: refers to both obstructed and restricted ventilatory defect[22,23].
Data analysis
Ethical consideration
RESULT
Socio- demographic characteristics
|
Parameter |
Woodworkers (n=70) |
Non-woodworkers (n=70) |
P-value |
|
Age, mean ± SD in years |
27.86±7.886 |
26.49 ±5.378 |
0.209 |
|
Height, mean ± SD in cm |
169.74± 5.93 |
170.80±5.958 |
0.95 |
|
Weight, mean ± SD in kg |
59.89±5.77 |
59.99±5.599 |
0.917 |
|
BMI, mean ± SD |
20.7871±1.70 |
20.548±1.22 |
0.344 |
|
Duration of service, mean ± SD in years |
7.20 ± 5.45 |
7.45± 4.40 |
0.04 * |
|
*- Significant p-value. |
|
|
|
Prevalence of respiratory disorders/ventilatory impairments
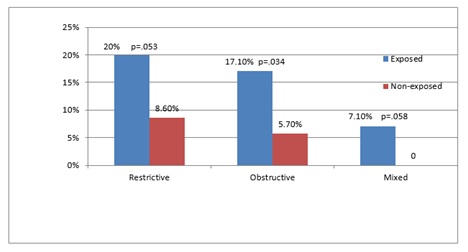 Figure 1: Magnitude of pulmonary function impairments among woodworkers and non-woodworkers in Jimma town, South West Ethiopia, 2018.
Figure 1: Magnitude of pulmonary function impairments among woodworkers and non-woodworkers in Jimma town, South West Ethiopia, 2018.|
Type of respiratory disorder |
Woodworkers (n=70) |
Non-woodworkers (n=70) |
Total |
P-value |
|
Number (%) |
Number (%) |
Number (%) |
||
|
Restrictive |
14 (20.0) |
6 (8.6) |
20 (14.3) |
0.053 |
|
Obstructive |
12 (17.1) |
4 (5.7) |
16 (11.4) |
0.034* |
|
Asthma |
8 (11.4) |
3 (4.3) |
11 (7.9) |
0.021* |
|
COPD |
4 (5.7) |
1 (1.4) |
5 (3.6) |
0.024* |
|
Mixed |
5 (7.1) |
0 (0.0) |
5 (3.6) |
0.058 |
|
Total |
31 (44.2) |
10 (14.3) |
41 (29.3) |
0.023* |
|
*- Significant p-value. |
|
|
|
|
Among total 16 respondents (11.4%) diagnosed by spirometer for airway obstruction, 11 (7.9%) were diagnosed clinically as asthma while the left 5 (3.6%) were determined as COPD. The burdens of asthma and COPD among woodworkers were higher (11.4% and 5.7%) than the control group (4.3% and 1.4 %) respectively as stated in Table 2.
DISCUSSION
Obstructive type of ventilatory impairment was diagnosed by spirometer among 16 respondents (11.4%) where higher prevalence was observed among woodworkers(17.1%) and 5.7% among non-woodworkers which was also in line with the study conductedin Ghana by Ennin IE et al who reported the highest magnitude of obstructive defects (37%) among woodworkers and22% among non-woodworkers [29] and the study conducted in Cameroon by Francis NDE et al who reported relatively lower burden of obstructive syndrome (6.2%) among woodworkers and 4.9% among non-woodworkers[28]. But the finding of the present study was against the study conducted by Baran et al who reported that none of the subjects were diagnosed with obstructive pattern among woodworkers [4]. This difference might be due to the difference in the exposed dust concentration, particle size, exposure time, and also due to a variety of background and individual factors (e.g., specific sort of wood, wood dust related biohazards or disease history or use of personnel protective equipment).
The present study tried to diagnose and discriminate the two types obstructive diseases (asthma and COPD) clinically as spirometer definition (Post-bronchodilator spirometer result) is not applicable because the respondents didn’t start medication; but spirometer result without post-bronchodilator was used as limitation. Accordingly, asthma and COPD were diagnosed among 8 (11.4%) and 4 (5.7%) of woodworkers respectively. The discriminated magnitude of asthma (11.4%) among woodworkers was also supported with the global and African estimated prevalence of asthma among woodworkers (5.6%-18%) and (3%-7%) respectively [7]. The finding of present study was also supported by the study conducted in south-eastern Nigeria that reported about 6.5% prevalence of occupational asthma among woodworkers [30]. But in contrast to the present finding in regarding to the magnitude of asthma (11.4%) diagnosed among woodworkers, Ameille et al reported lower magnitude of occupational asthma (3.7%) among woodworkers in France [31] probably due to socio-demographic difference in screening, safety and awareness about disease. The prevalence of COPD among woodworkers was 5.7% which is also in agreement with the study of Matheson MC et al who reported 3.4% prevalence of COPD among workers exposed to dust [32].
About 20 (14.3%) of the respondents were diagnosed with restrictive type respiratory disorders and higher magnitude (20%) was identified among woodworkers when compared to the control group (8.6%). The observed restrictive ventilatory defect difference between woodworkers and non-woodworkers may be attributed to inflammatory changes in lung parenchyma caused by the presence of wood dust, a condition that could cause pulmonary edema and fibrosis of lung tissue leading to a reduced FVC values. This finding was also consistent with study conducted in Ghana by Ennin IE et al who reported the magnitude of restrictive defect (32%) among woodworkers and 15% among non-woodworkers [29] and study of Francis NDE et al conducted in Cameroon who revealed that the burden of restrictive syndrome of 17% and 11.5% among woodworkers and non-woodworkers [28]. However, our study was in contrast to the study conducted in Poland by Baran S et alwho reported that none of the woodworkers developed a restrictive ventilatory defect on spirometer tests [4]. This could be due to difference in occupational health awareness for preventive measures such as utilization of protective devices, health seeking behavior and duration of wood dust exposure between the study areas.
In the present study, the prevalence of respiratory disorders/ ventilatory impairments was 44.2% and 14.3% among woodworkers and control group respectively. Among woodworkers the burden of restrictive, obstructive and mixed pattern was 20%, 17.1% and 7.1% respectively. In harmony with our study, the prevalence of respiratory impairment among exposed group (29.4%) as compared to 2.2% among unexposed controls was reported by Rastogi SK et al with pattern of restrictive type dominance (28.4%) observed among woodworkers [33].
CONCLUSION
ACKNOWLEDGEMENT
CONFLICT OF INTEREST
REFERENCES
- Hamalainen P, Takala J, Kiat TB (2017) Global estimates of occupational accidents and work-related illnesses 2017. World Congress on Safety and Health at Work: 1-21.
- Jacobsen G, Schaumburg I, Sigsgaard T, Schlunssen V (2010) Non-malignant respiratory diseases and occupational exposure to wood dust. Part II. Dry wood industry. Ann Agric Environ Med 17: 29-44.
- Schlünssen V, Schaumburg I (1998) Asthma, bronchitis and chronic obstructive pulmonary disease in occupational exposure to wood. Ugeskr Laeger 160: 609-615.
- Baran S, Swietlik K, Teul I (2009) Lung function: occupational exposure to wood dust. Eur J Med Res 14: 14-17.
- Carton M, Goldberg M, Luce D (2002) Occupational exposure to wood dust. Health effects and exposure limit values. Rev Epidemiol Sante Publique 50: 159-178.
- Black N, Dilworth M, Summers N (2007) Occupational exposure to wood dust in the British woodworking industry in 1999/2000. Ann Occup Hyg 51: 249-260.
- Chamba P, Nunes E (2016) Work-related asthma among workers in the wood-processing industry: a review: allergies in the workplace. Curr Allergy Clin Immunol 29: 110-117.
- Wiggans RE, Evans G, Fishwick D, Barber CM (2015) Asthma in furniture and wood processing workers: a systematic review. Occup Med 66: 193-201.
- Esmaeil N, Gharagozloo M, Rezaei A, Grunig G (2014) Dust events, pulmonary diseases and immune system. Am J Clin Exp Immunol 3: 20-29.
- Tanko Y, Olakunle Y, Jimoh A, Mohammed A, Goji ADT, et al. (2011) Effects of Wood Dust on Cardiopulmonary Functions and Anthropometric Parameters of Carpenters and Non-Carpenters in Sabon Gari Local Government Area, Kaduna State, Nigeria. Asian J Med Sci 3: 43-46.
- Ratnasingam J, Ioras F, Tadin I, Wai LT, Ramasamy G (2014) Respiratory Effects in Woodworkers Exposed to Wood and Wood Coatings Dust: A Regional Evaluation of South East Asian Countries. J Appl Sci 14: 1763-1768.
- Doney B, Hnizdo E, Graziani M, Kullman G, Burchfiel C, et al. (2014) Occupational risk factors for COPD phenotypes in the Multi-Ethnic Study of Atherosclerosis (MESA) lung study. COPD J Chronic Obstr Pulm Dis 11: 368-380.
- Fishwick D, Sen D, Barber C, Bradshaw L, Robinson E, et al. (2015) Occupational chronic obstructive pulmonary disease: a standard of care. Occup Med 65: 270-282.
- Trupin L, Earnest G, San Pedro M, Balmes JR, Eisner MD, et al. (2003) The occupational burden of chronic obstructive pulmonary disease. Eur Respir J 22: 462-469.
- Vallières E, Pintos J, Parent ME, Siemiatycki J (2015) Occupational exposure to wood dust and risk of lung cancer in two population-based case-control studies in Montreal, Canada. Environ Health 14: 1.
- Alonso-Sardón M, Chamorro AJ, Hernández-García I, Iglesias-de-Sena H, Martín-Rodero H, et al. (2015) Association between occupational exposure to wood dust and cancer: a systematic review and meta-analysis. PloS One 10: e0133024.
- Hassen KA, Ibrahim MS (2014) Exposure to occupational dust and changes in pulmonary function among cobblestone paving workers of Jimma, Ethiopia. Rev Ambiente Água 9: 19-26.
- Tefereedgn EY, Ayana AM, Tefereedgn EY, Ayana AM (2018) Prevalence of Asthma and Its Association with Daily Habits in Jimma Town, Ethiopia. Open J Asthma 2: 11-17.
- Reta W, Tadessa S, Tegene E (2018) The value of individual variables of BODE index and GOLD spirometry in stratifying the severity of COPD. Pulmonol Respir Res 6: 1.
- Demissie RW (2018) Prevalence of Cardiac Arrhythmias among Chronic Obstructive Pulmonary Disease Patients Admitted to Jimma University Medical Center. Biomed J Sci&Tech Res 10: 1-6.
- Miller MR, Hankinson J, Brusasco V, Burgos F, Casaburi R, et al. (2005) Standardisation of spirometry. Eur Respir J 26: 319-338.
- Vogelmeier CF, Criner GJ, Martinez FJ, Anzueto A, Barnes PJ, et al. (2017) Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2017 report. GOLD executive summary. Am J Respir Crit Care Med 195: 557-582.
- Mannino DM, Ford ES, Redd SC (2003) Obstructive and restrictive lung disease and functional limitation: data from the Third National Health and Nutrition Examination. J Intern Med 254: 540-547.
- Rabe KF, Hurd S, Anzueto A, Barnes PJ, Buist SA, et al. (2007) Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med 176: 532-555.
- Bernstein IL, Bernstein DI, Chan-Yeung M, Malo JL (2013) Definition and classification of asthma in the workplace. Asthma Workplace 3: 1-5.
- Toelle BG, Peat JK, Salome CM, Mellis CM, Woolcock A (1992) Toward a Definition of Asthma for Epidemiology. Am Rev Respir Dis 146: 633-637.
- Caronia JR, Jiang C, Lessnau KD (2018) Restrictive Lung Disease: Background, Pathophysiology, Etiology.
- Lofstedt HA, Hagstrom K, Bryngelsson IL, Holmstrom M, Rask-Andersen A (2017) Respiratory symptoms and lung function in relation to wood dust and monoterpene exposure in the wood pellet industry. Ups J Med Sci 122: 78-84.
- Ennin IE, Adzaku FK, Dodoo D, Adukpo S, Antwi-Boasiako C, et al. (2015) A study of lung function indices of woodworkers at the Accra timber market in Ghana. Donnish J Med Med Sci 2: 120-124.
- Aguwa EN, Okeke TA, Asuza MC (2007) The prevalence of occupational asthma and rhinitis among woodworkers in south-eastern Nigeria. Tanzan J Health Res 9: 52-55.
- Ameille J, Pauli G, Calastreng-Crinquand A, Vervloet D, Iwatsubo Y, et al. (2003) Reported incidence of occupational asthma in France, 1996-99: the ONAP programme. Occup Environ Med 60: 136-141.
- Matheson MC, Benke G, Raven J, Sim MR, Kromhout H, et al. (2005) Biological dust exposure in the workplace is a risk factor for chronic obstructive pulmonary disease. Thorax 60: 645-651.
- Rastogi SK, Gupta BN, Husain T, Mathur N (1989) Respiratory Health Effect from Occupational Exposure to Wood Dust in Sawmills. Am Ind Hyg Assoc J 50: 574-578.
Citation: Fentie D, Mariam TG, Mulat E, Demissie WR(2019) Prevalence of Respiratory Disorders among Woodworkers in Jimma Town, Southwest Ethiopia. J Pulm Med Respir Res 5: 022.
Copyright: © 2019 Dilnessa Fentie, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.