Reproductive Health Indicators Among Women with Celiac Disease in Sudan at Ibn Sina Specialized Hospital from December 2014 to June 2015
*Corresponding Author(s):
Salma M HassanSpecialist, Obstetrics And Gynecology, Sudan
Tel:+249911137869,
Email:loma.2009@hotmail.com
Abstract
Background: Celiac disease is an immune-mediated mucosal disorder primarily affecting the small intestine in genetically-susceptible individuals. It may be triggered by dietary exposure to gluten. In some patients, extra-intestinal or autoimmune changes may occur, as hepatobiliary, neurological, or endocrine disorders. The aim to study the reproductive health indicators among Sudanese female with celiac disease (15-45 years) and to determine menstrual pattern, infertility status as well as obstetrical outcome among those women at Ibn sina specialized hospital from December 2014 to June 2015.
Material and Methods: This is a descriptive analytic hospital based study, carried out at Ibn sina specialized hospital, conducted from December 2014 to June 2015, included 81 women, diagnosed as celiac disease, attended celiac clinic during the study period. The data was collected using a questionnaire by me after agreed informative consent and analyzed by computer using SPSS program (20).
Results: 32 (39.5%) of women were between 25-34 years and 58 (71.6%) of women were on strict gluten diet. 52 (64.1%) of women had menarche after age of 16, 30 (37%) experienced oligomenorrhoea and 2 (2.5%) had secondary amenorrhoea and their menstrual pattern was improved with gluten free diet(P value 0.002), 36 (44.4%)of women were married, 21 (58.3%) of these women experienced difficulty in conceiving which affected by the duration of their disease(P value 0.000), 23 (63.9%), 21 (58.3%) had past history of miscarriage and pregnancy induced hypertension respectively.
Conclusion: celiac disease has a significant role in women reproductive health, in the form of delay menarche, a change of menstrual pattern, difficulty in conceiving, and poor obstetric outcome such as miscarriage and pregnancy induced hypertension.
Keywords
INTRODUCTION
The estimated population prevalence of diagnosed CD in many Western countries approaches 1 percent. The highest prevalence rates of the disease are noted in the Saharawi people of Africa. The mean prevalence of CD is 5.6% according to literature (in North Africa). There is little information on CD prevalence in South Asia and unfortunately no incidence of CD in Sudan. There is a strong genetic tendency, 75 percent of monozygotic twins are concordant for the disease, compared to 10 percent of dizygotic twins; 10 percent of first degree family relatives of an index patient have CD, Human Leukocyte Antigen (HLA) alleles encoding the antigens DQ2 and DQ8 show the strongest association with CD; however, most individuals expressing DQ2 or DQ8 do not develop the disease. Geographic differences in disease prevalence are explained to an extent by genetic differences between populations. For instance, carriage of DQ2 and DQ8 is up to 40 percent in Caucasians and there is a very high carriage of DQ8 among the Saharawi, on the other hand, DQ2 is absent in the population of Burkina-Faso where celiac disease is also absent [3,4].
Celiac disease can develop at any age after people start eating foods or medicines that contain gluten. It is common in female more than male, it can occur at any age but the commonest age of presentation is in the early childhood and later in adulthood between 40 and 60 years old. The commonest presentation is iron deficiency anemia. Diarrhoea usually presents as well as constitutional symptoms of lassitude, weight loss, glossitis, angular stomatitis and symptoms relating to anemia, vitamin D deficiency or osteoporosis may be presenting problem in adults, others presentations in adults include depression and korsakoff-like syndrome [5].
Celiac disease is associated with reproductive disorders, including delayed menarche, menstrual disturbances, unexplained sub fertility, and endometriosis. There is an established relationship between overt CD and adverse reproductive consequences, including sub fertility, the relationship between silent CD and sub fertility has been more controversial [6].
In a case-control study on women with subfertility for unexplained reasons, 4.1% (4 out of 98 patients) of the cases were affected by CD in comparison to 0 out of 150 controls, even more recent studies have confirmed a higher CD incidence in women with subfertility problems, thus it seems possible that, in some patients, unexplained subfertility can be the consequence of a clinically silent disease, it being it’s first and, sometimes, only symptom. However, the correlation between subfertility and CD remains controversial [7].
Celiac women, even if affected by subclinical CD, have their menarche at an older age. A case-control study carried out on 180 women in Italy in 1990 reported that the menarche takes place at about 13.5 years of age among the celiac population, whereas in normal subjects this event occurs at 12 years of age. In more recent times, another study, on analyzing the menstrual history of 200 Brazilian women, proved a significant delay in puberty in celiac patients in comparison to the control group, including patients with Irritable Colon Syndrome (IBS) [7].
In celiac patients not complying with the gluten-free diet, a greater frequency of secondary amenorrhea has also been found. In one study, secondary amenorrhea was present in 38.8% of women with untreated CD, in comparison to 9.2% of non-celiac women used as controls [8].
Celiac disease, especially if untreated, appears to increase the risk of repeated miscarriages and premature deliveries, recurrent stillbirths and abnormalities of placentation that could lead to Intrauterine Growth Restriction (IUGR) and reduced birth weight, Pregnancy Induced Hypertensive (PIH) and birth defects, such as neural tube defects caused by poor absorption of such nutrients as folic acid, also it associated with orofacial defects and heart defects, also unexplained fetal death. In addition, adverse effects on the mother may also occur, as indicated by a recent German study which demonstrated that the rate of cesarean delivery is increased if the parents have CD [8].
Most of the CD related pregnancy problems seem to occur in women who have not yet been diagnosed with celiac, or in women who have been diagnosed but who are not following the gluten-free diet [9].
Pregnancy complications occur at a very high rate in women with CD, according to a comprehensive Italian study of reproductive life disorders in celiac women. Placental abruption occurred in more than 18% of the celiac women but only 1% of controls. PIH occurred in 10% of the celiac women and none of the control subjects [9].
Activation of CD during the puerperium has been hypothesized to be related to immunologic or hormonal factors, or both, the duration of breast-feeding was decreased in untreated mothers with CD, which was effectively corrected by treatment with a gluten-free diet [10].
Several studies have demonstrated implications of CD on the reproductive health of women. Studies evaluating the relationship between CD and adverse reproductive experiences, including sub fertility, recurrent pregnancy loss, and poor obstetric outcome have a number of limitations, including inconsistent and incomplete criteria for the diagnosis of CD and sub fertility. They have often involved small and underpowered sample sizes and have combined patients who presented with typical gastrointestinal symptoms and those with silent disease. Several reports have inappropriate control groups or no control groups at all [11].
It is challenging to identify women with silent CD and treat them with a gluten-free diet and nutrient supplements, which may lead to prevention of menstrual and other reproductive [12].
The earlier diagnosis and starting of treatment of celiac disease is the better outcome of women reproductive health. There are lack of information concerning this topics, it is possibly due to absence of previous studies that conducted in Sudan, regarding the celiac disease and I think, it is the high time to do more researches and work up to improve women reproductive health.
MATERIAL AND METHODS
The study included all females in the reproductive age (15-45 years) with CD during the study period whether single or married nullipara or multipara, who presented to the referred clinics of CD at Ibn sina specialized hospital.
The study excluded those who have co -existing diseases that may lead to fertility problems and seven women refused the study due to cultural issues.
The sample size was determined by using the above formula when:
D=Desire marginal error of precision level (0.05) at confidence level 95%.
Thus, a sample size which was;
N=Sample size.
P=Prevalence of the problem 5.6% (0.056)
Q=I-P (0.944)
Z=Standard normal deviation (1.96)
Estimated using the above formula:
N= (1.96)2 *0.056*0.944/ (0.05)2 = 81
Then the study sample included 81 women.
The sample was collected in convenient way from the celiac referred clinic. Data was collected through direct interview by me using a detailed and structured questionnaire included closed-ended questions covering the following areas: Socio-demographic, obstetrical and gynecological history, height and weight to determine the Body Mass Index (BMI). The data was analyzed using Statistical Package for Social Science (SPSS) software version 20. The results were presented in the form of frequency tables, cross tabulations and graphs (pie chart and bar chart) for each particular variable in the study objectives using the same (SPSS) software version 20.
Ethical clearance and approval for conducting this research was obtained from the general manager of the hospital and Research Ethical committee at SMSB, informed written consent was obtained from every respondent who agreed to participate in the study. Confidentiality of data from the patients was assured.
RESULTS
| Age | Frequency | percent |
| 15-24 | 19 | 23.5% |
| 25-34 | 32 | 39.5% |
| 35-45 | 30 | 37% |
| Residence | ||
| Urban areas | 55 | 67.9% |
| Rural areas | 26 | 32.1% |
| Body mass index | ||
| Under weight | 25 | 30.9% |
| Normal weight | 47 | 58% |
| Over weight | 4 | 4.9% |
| Obese | 5 | 6.2% |
| Marital Status | ||
| Single | 45 | 55.6% |
| Married | 36 | 44.4% |
| Total | 81 | 100% |
46 (56.8%) of women had CD for 5 to 10 years, while 24 (29.6%) had CD for less than five years and 11 (13.6%) had CD for more than 10 years (Figure 1), more than half of women used to have restriction of gluten from their meals 58 (71.6%) while 23 (28.4%) of women were not on gluten free diet (Figure 2).
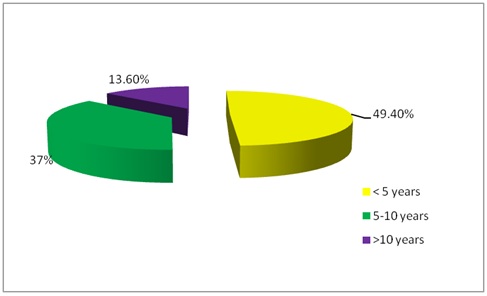 Figure 1: Distribution of cases according to their duration of disease, at Ibn sina specialized hospital from December 2014 to June 2015.
Figure 1: Distribution of cases according to their duration of disease, at Ibn sina specialized hospital from December 2014 to June 2015.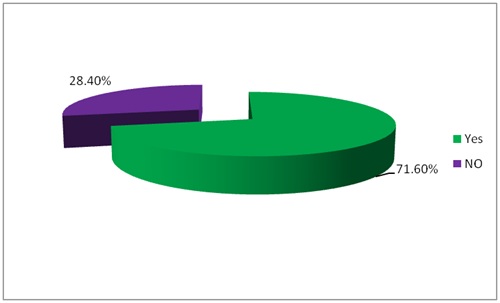 Figure 2: Distribution of cases according to restriction on gluten free diet, at Ibn sina specialized hospital from December 2014 to June 2015.
Figure 2: Distribution of cases according to restriction on gluten free diet, at Ibn sina specialized hospital from December 2014 to June 2015.52 (64.1%) of women had their first menses after age of 16 and 16 (19.8%), 11 (13.6%) had their menarche between 11 to 13 years and 14 to 16 years respectively and just 2 (2.4%) of women had menarche at age less than 11 (Figure 3), half of women had normal menstrual pattern 40 (49.4%), while 30 (37%) experienced oligomenorrhoea and 5 (6.2%), 2 (2.5%) of women had secondary amenorrhaoea and menorrhagia respectively. No one of women had hypomenorrhoea (Figure 4). 21 (58.3%) of women experienced difficulty in conceiving versus 15 (41.7%) did not (Table 2).
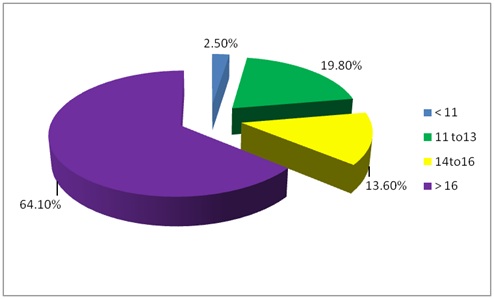 Figure 3: Distribution of cases according to their menarche, at Ibn sina specialized hospital from December 2014 to June 2015.
Figure 3: Distribution of cases according to their menarche, at Ibn sina specialized hospital from December 2014 to June 2015.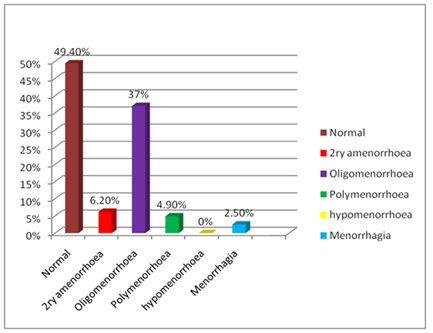
| Frequency | Percent | |
| Yes | 21 | 58.3% |
| No | 15 | 41.7% |
| Total | 36 | 100% |
| Miscarriage | Frequency | percent |
| Yes | 23 | 63.9% |
| No | 13 | 36.1% |
| Total | 36 | 100% |
| Preterm delivery | ||
| Yes | 6 | 16.7% |
| No | 30 | 83.3% |
| Total | 36 | 100% |
| Pregnancy induced hypertension | ||
| Yes | 21 | 58.3% |
| No | 15 | 41.7% |
| Total | 36 | 4.9% |
| Intrauterine growth restriction | ||
| Yes | 1 | 2.8% |
| No | 35 | 97.2% |
| Total | 36 | 100% |
| Stillbirths | ||
| Yes | 1 | 2.8% |
| No | 35 | 97.2% |
| Total | 36 | 100% |
| Birth defects | ||
| Yes | 1 | 2.8% |
| No | 35 | 97.2% |
| Total | 36 | 100% |
| Mode of delivery | ||
| Vaginal delivery | 21 | 70% |
| Casearean delivery | 9 | 30% |
| Total | 30 | 100% |
30 (83.3%) of women had not preterm delivery versus 6 (16.7%) had history of preterm delivery, 21 (58.3%) had history of PIH while 15 (41.7%) had not, (table 3).
35 (97.2%) did not have history of IUGR, whereas 1 (2.8%) had history of IUGR, (Table 3).
35 (97.2%) did not have history of stillbirth or history of birth defects, whereas 1 (2.8%) had history of stillbirth or history of birth defects, 21 (70%) delivered vaginally while 9 (30%) delivered by caesarean section (Table 3).
Cross tabulation shows the effect of gluten diet restriction on menstrual pattern, 23 of women who were on gluten free diet had improvement in their menstrual pattern while 8 of cases had no obvious change (P value 0.002), which is highly significant (Table 4).
| Items | Yes | No | P value |
| The effect of gluten diet restriction on menstrual pattern | 23 | 8 | 0.002 |
| The duration of disease and difficulty in conceiving | 18 | 2 | 0.000 |
| Body mass index and restriction on gluten free diet | 42 | 5 | 0.000 |
Cross tabulation between body mass index and restriction on gluten free diet, 42 of women who restricted on gluten free diet had normal weight (P value 0.000), which is highly significant, (Table 4).
DISCUSSION
Age distribution showed that 32 (39.5%) and 30 (37%) were between 25-34 years and 35-45 years and this is not far from the literature that emphasized that CD can occur at any age but it increase in childhood and in adulthood between 40 to 60 years (5).
More than half of women were living at urban 55 (67.9%), reflecting the role of environmental factors such as excessive exposure to wheat in urban more than rural areas, also people who are living in urban areas, searching continuous medical advices and it is supported by literature [13,14].
About half of women had normal weight 47 (58%), that has been correlated to restriction of gluten diet (P value 0.000) and it is supported by literature, showed that women almost achieved their normal weight or overweight after gluten free diet.
Fifty eight (71.6%) of women tend to restrict their diet and it is due to availability of a dietitian in CD clinic, in who has been participated in improving the compliance of these women, supporting and encouraging them [15].
The average age of menarche is 12.3 years in African women, in this study, more than two third of women 63 (77.7%) had menarche after the age of 14, the delaying possibly is due to malnutrition associated with CD, as these women were on strict gluten diet, they tend to reduce their body mass index and so reduce adipose fat that secrete some protein (as leptin), influencing the hypothalamus and involving in various aspects of female reproductive function, the result consistent with study, conducted by Fergusson et al., and another study published in 2004 by Kotz et al.,. There was study conducted in Brazilian women, proved that there was a significant delay in puberty in celiac patients in comparison to control group, in contrast to that study, conducted at university of Messina in Italy in 2008, it conclude, untreated CD may not associated with menarcheal retardation [16,17].
About third of those women had oligomenorrhoea 30 (37%), while the lesser percentages were for secondary amenorrhoea, polymenorrhoea and menorrhagia 5 (6.2%), 4 (4.9%) and 2 (2.5%) respectively and about half of those women experienced some improvement in their menstrual pattern while they were on gluten free diet (P value 0.002) and it is supported by case control Italian study, it has been explored that there is association between CD and menstrual disorders in form of amenorrhoea, oligomenorrgoea, hypomenorrhoea and menorrhagia [18].
Thirty six (44.4%) of women were married, near to two third of these women experienced some difficulty in conceiving 21 (58.3%), it has been correlated to duration of CD because 18 of these women have disease for 5 to 10 years (P value 0.000), probably the etiology of this difficulty is multi factorial. There are many problems seen in CD that may affect a woman’s ability to achieve a pregnancy like delay of menarche and menstrual disorders (ovulation problems), putting in mind sub fertility may be immune mediated, it is near to some studies, conducted in Europe and Mid east, it emphasized, CD has been associated with sub fertility, as well as it is consistent with Canadian study in 2008, revealed that, CD may be a significant contributor to fertility problems in women, as well as studies that carried out by Sher et al ,. Collin and colleagues and Certain study that was performed in Sardinia by Meloni et al, Swedish study concluded that women with CD overall had normal fertility and this explained by the modality of life of Swedish women [19-21].
In regard to obstetrics outcome, 23 (63.9%) had past history of miscarriage and it is supported by literature, as it has been shown in Ogborn study, conducted in 1975 and the study has been performed by Gasbarrini, both gave corresponding results. Another several studies were done in Italy, Argentina and United Kingdom have been supported, the association between higher incidences of miscarriages and CD and the exact reason is not clear but it can be related to nutritional and immunological problems that associated with CD [20,22,23].
Near to two third of women 21 (58.3%) had past history of PIH, knowing the majority of women with CD had anemia, this low hemoglobin play role in PIH as well as role of antibodies that can affect placental function. The result compatible with study which was performed in Italy that showed 10% of CD women may have PIH.
Although three studies from Italy, Denmark and Swedish revealed the association between preterm delivery and CD, this study inferred only 6 (16.7%) of women had past history of preterm delivery [24].
1 (2.8%) women had past history of IUGR that is corresponding to large Italian study, it is concluded no higher incidence of IUGR in celiac patients, in reverse to some studies that conducted in Europe, Italy and population based cohort study Orebro university hospital and Swedish society of medicine that has been explored the association between IUGR and CD [25-27]
About 1 (2.8%) of women had stillbirth and it is not identical to the result of Leicester general hospital in United Kingdom that has been supported that association [16].
In the study 1 (2.8%) of women had birth defects, it has been supported by literature like Swedish study and another study which has been conducted in united kingdom inferred, there was association between CD and birth defects, however the risks were small [28,29].
Approximate two third of women has been delivered vaginally 21 (70%), it is opposite to the recent German study that has been concluded, the rate of caesarean section increased if the parents had CD, and also same result was concluded from Italian study [5,30].
CONCLUSION
The study shows CD play a significant role in reproductive health in form of delay menarche, menstrual pattern change, it has been inferred influence of gluten free diet on menstrual pattern. It concluded, women may experienced some difficulty in conceiving and it is associated with duration of disease. There are some complications that may occur for women with CD such as miscarriage and PIH.
FUTURE DIRECTIONS
RECOMMENDATIONS
• Continuous integration between obstetricians and gynecologists and Gastroenterology consultants during the follow up assessment of women with CD
• Availability of a dietitian for celiac patients to support, encourage them and to give them comprehensive information about their diet and others alternatives
• Routine CD screening for women who has unexplained gastrointestinal symptoms, family history of CD, menstrual disorders or who had past history of adverse outcome during pregnancy.
• Routine CD screening for women who has unexplained subfertility
• Future studies will be needed to clarify the association between CD and reproductive health problems specially fertility issues, including laboratory investigations (hormonal profile) in those studies
REFERENCES
- Lewis NR, Holmes GKT (2010) Risk of Morbidity in Contemporary Celiac Diseas. Expert Rev Gastroenterol Hepatol 4: 767-780.
- Yamada T, Alphers DH (2003) Textbook of Gastroenterology (4thedn), Lippincott Williams & Wilkins, Philadelphia, USA.
- Fauci A, Braunwald E, Kasper D, Hauser S, Longo D, et al. (2008) Harrison's Principles of Internal Medicine (17thedn). Mcgraw-hill Publishers, USA. Pg no: 872-1885.
- Lebwohl B, Green P (2003) Screening for Celiac Disease. N Engl J Med 349: 1673-1674.
- Bloom S, Webster GD (2006) Oxford handbook of GIT & Hepatology (7thedn). Oxford university Press, UK.
- Pellicano R, Astegiano M, Bruno M, Fagoonee S, Rizzetto M (2007) Women and celiac disease: Association with unexplained infertility. Minerva Med 98: 217-219.
- Collin P, Vilska S, Heinonen PK, Hällström O, Pikkarian P (1996) Infertility and celiac disease. Gut 39: 382 -384.
- Sher K, May J (1996) Female fertility, obstetric and gynecological history in celiac disease, a case control study. Acta Paediatr Suppl 412: 76-77.
- Martinelli D, Fortunato F, Tafuri S, Germinario CA, Prato R (2010) Reproductive life disorders in Italian celiac women. A case-control study. BMC Gastroenterology 10: 89.
- Stazi A, Trinti A (2005) Reproductive aspects of celiac disease. Ann Ital med Int 20: 143-157.
- Green PH, Jabri B (2003) Celiac disease. Lancet 362: 383-391.
- Norgard B, Fonuger K, Sorensen HT, Olsen S (1999) Birth outcomes of women with celiac disease: a nationwide historical cohort study. Am J gastroenterol 94: 2435-2440.
- Rewers M (2005) Epidemiology of celiac disease: what are the prevalence, incidence, and progression of celiac disease? Gastroenterology 128: 47-51.
- Sollid LM (2008) Hunting for Celiac Disease Genes. Gastroenterol 134: 869-871.
- Cheng J, Brar PS, Lee AR, Green PH (2010) Body mass index in celiac disease: beneficial effect of a gluten-free diet. J Clin Gastroenterol 44: 267-71.
- Shelly S, Shawky Z (2010) Celiac Disease and Its Effect on Human Reproduction: A Review. Journal of Reproductive Medicine 55: 3-8.
- Sferlazzas C, Arrigo T, Salzano G, Pellegrino S, La Fauci G, et al., (2008) Menarcheal age in celiac disease may not be delayed and may be irrespective of age at diagnosis and dietary management. J Endocrinol Invest 31: 432-435.
- Mohindra S, Yachha SK, Srivastava A, Krishnani N, Aggarwal R, et al., (2001) Coeliac disease in Indian children: assessment of clinical, nutritional and pathologic characteristics. J Health Popul Nutr 19: 204-208.
- Sherk S, Mayberry JF (1994) Female fertility, obstetric and gynaecological history in coeliac disease. A case control study. Digestion 55: 243-246.
- Molteni N, Bardella MT, Bianchi PA (1990) Obstetric and gynecological problems in women with untreated celiac sprue. J Clin Gastroenterol 12: 37-39.
- Speroff L, Fritz MA (2005) Clinical Gynecologic Endocrinology and Infertility (7thedn). Philadelphia lippencott Williams & wilkins, USA.
- Sher KS, Jayanthi V, Probert CSJ, Stewart CR, Mayberry JF (1994) Infertility, Obstetric and Gynaecological Problems in Coeliac Sprue. Dig Dis 12: 186-190.
- Orgborn AD (1975) Pregnancy in patient with celiac disease 82: 293-296.
- Greco L, Veneziano A, Di Donato L, Zampella C, Pecoraro M, et al. (2004) Undiagnosed coeliac disease does not appear to be associated with unfavourable outcome of pregnancy. Gut 53: 149-151.
- Stazi AV, Mantovani A (2000) A risk factor for female fertility and pregnancy: celiac disease. Gynecol Endocrinol 14: 454-463.
- Khashan AS, Henriksen TB, Mortensen PB, McNamee R, McCarthy FP, et al. ( 2010) The impact of maternal celiac disease on birthweight and preterm birth: a Danish population-based cohort study. Hum Reprod 25: 528-534.
- Rostami K, Steegers EA, Wong WY, Braat DD, Steegers-Theunissen RP (2001) Coeliac disease and reproductive disorders: a neglected association. Eur J Obstet Gynecol Reprod Biol 96: 146-149.
- Zugna D, Richiardi L, Stephansson O, Pasternak B, Ekbom A, et al., (2014) Risk of congenital malformations among offspring of mothers and fathers with celiac disease: a nationwide cohort study. Clin Gastroenterol Hepatol 12: 1108-1116.
- Fasano A, Berti I, Gerarduzzi T, Not T, Colletti RB, et al., (2003) Prevalence of celiac disease in at-risk and not-at-risk groups in the United States: a large multicenter study. Arch Intern Med 163: 286-292.
- Adams F (1856) On the Coeliac Affection. The Extant Works of Aretaeus, the Cappadocian. Sydenham Society, London. Pg no: 350-351.
Citation: Hassan SM, Yassin K, Zakaria NA (2017) Reproductive Health Indicators Among Women with Celiac Disease in Sudan at Ibn Sina Specialized Hospital from December 2014 to June 2015. J Reprod Med Gynecol Obstet 2: 007.
Copyright: © 2017 Salma M Hassan, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.