Expansion of Ergonomic Function in Medical Robotics
*Corresponding Author(s):
Vadim GolovinMoscow Polytechnic University, Moscow, Russian Federation
Tel:+7 4952230523,
Email:medicalrobot@mail.ru
Abstract
The features of ergonomics in medical robotics are considered in the article. They are caused by the fact that the third component of the ergonomic system is not a technical environment but patient’s person. This system belongs to the class of man-machine systems. A number of new connections, circuits, subsystems and modes appear. The third component of ergatic system can be useful for control, if this component is an alive human patient. The modes of individual robot control by a patient and mutual performance of procedure by a physician and robot in restorative medicine are of a particular interest. Accounting for the third component allows providing the safe joint work of a physician and robot.
Keywords
INTRODUCTION
Ergonomics is scientific and applied discipline about activities of human interacting with labor instruments, beginning with a shovel. In any sphere of human activities ergonomics is organization of human conditions of labor, service and safety. Ergonomics is service and it is a part of Mesrob workshop.
Ergonomics excludes fully automatic operation of machines without human participation and sets the optimal human-machine interaction. It relates to ergonomics in industry, agriculture, transport, military affairs and medicine [1]. For example, it is mobile robot inspecting and repairing pipelines of the water drain. The ergatic control system of this robot can operate in command, tracking, interactive modes and observing moving [2]. The ergonomic aspects of medical mini-robotic system designing are dealt in paper [3]. Also the problems of medical ergonomics are discussed in paper [4]. The problems of military affairs of ergonomics are considered in monograph [1].
But human conditions of labor, service and safety as a rule are provided in relation to person exploiting the machine. Except two indicated components the third component of control object is included in ergatic system. Generally it is technical environment, for example detail, plowing, food and others. Certainly in any sphere of human activities the relation to the third human component is positive in order to help, except for military affairs, where the aim is to destroy selectively or en masse.
But the third component can be a man and not under anesthesia during surgery but living with individual psychophysiology. So a particularly important role of the third human component is manifested in medical robotics.
THREE COMPONENTS OF ERGATIC ROBOT SYSTEM IN RESTORATIVE MEDICINE
Let us consider robotic system of restorative medicine which performs the manipulations on soft tissues, for example massage [5,6]. The scheme of this system is given in figure 1. There are three components: physician-operator, robot, patient in this ergatic system, and also informative subsystem like knowledge base [7,8].
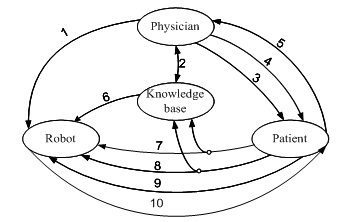 Figure 1: Scheme of interaction between components of physician-operator system, robot and patient.
Figure 1: Scheme of interaction between components of physician-operator system, robot and patient.• Use by the physician of the data, received in the previous sessions and knowledge base replenishment (system Medsoft)
• Psychological influence of the physician on the patient
• Manual execution of procedure by the physician (solo or with a robot)
• Signals of subjective patient’s state transmitted to the physician including verbal feedback
• Assigned values of forces, movements, velocities for position/force and nominal date for biotechnical control
• Signals of real state of soft tissues for position/force control
• Signals of real state of soft tissues for biotechnical control
• Signals of individual robot control from patient
• Robot action on patient
The indicated on the scheme influences, signals and modes form several control counters: automatic position/force control (6+7+10), automatic biotechnical control (6+8+10), command control (1+2+10), manual performing of procedure (4+5), mutual performance of procedure by physician and robot (1+2+3+4+5+6+7+8+9+10), individual robot control from patient (9). Some of indicated counters are open loop (3, 6) and others are closed loop (1, 2, 4, 5). The stability of closed loops is considered below.
On this scheme a lot relationships with patient is seen. These relationships form the modes which are not considered in ergonomics usually.
SUBSYSTEM OF POSITION/FORCE CONTROL IN ROBOTIC SYSTEM FOR RESTORATIVE MEDICINE
Main purpose of robotic system for restorative medicine consists in approaching to assigned physiological patient’s state in general by means of mechanical robot actions. The position/force control and biotechnical control systems are ones from sub systems of robotic system. The biotechnical control counter covers the position/force control one (Figure 2). In the contour of position/force control the patient’s biological soft tissue is a control object. In the contour of biotechnical control the converter of mechanical influence variables to variables of a psycho-physiological state is a control object. The sub goal of position/force control system is given as follows.
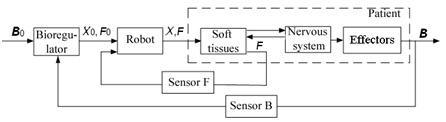 Figure 2: Block diagram of position/force and biotechnical control systems.
Figure 2: Block diagram of position/force and biotechnical control systems.

The theory of position/force control of robot interacting with dynamic environment is expounded within the framework of analytical mechanics in monograph [9]. Great Serbian scientist Miomir Vukobratovic and Russian mathematician Yury Ekalo have brought a substantial contribution to theory of dynamic control of robot - environment interaction and position/force control theory. The robot interacting with the dynamic environment can be presented by the following differential equation: 
The environment dynamics can be described by the following differential equation: Where  are the vectors of the generalized coordinates of position, velocity and acceleration accordingly, is the matrix characterizing inertial properties of the manipulator,
are the vectors of the generalized coordinates of position, velocity and acceleration accordingly, is the matrix characterizing inertial properties of the manipulator, ![]() is the vector characterizing gravitational, centrifugal, Coriolis’ forces,
is the vector characterizing gravitational, centrifugal, Coriolis’ forces, ![]() is the matrix characterizing inertial properties of the environment,
is the matrix characterizing inertial properties of the environment, ![]() is the vector characterizing viscoelastic properties of the environment and its weight,
is the vector characterizing viscoelastic properties of the environment and its weight, ![]() is the vector of the input control,
is the vector of the input control, ![]() is the vector of the forces operating on the end link (tool) of the manipulator from the environment,
is the vector of the forces operating on the end link (tool) of the manipulator from the environment,  is the nonsingular matrix. To guarantee the necessary quality transients the control law should be as follows:
is the nonsingular matrix. To guarantee the necessary quality transients the control law should be as follows:
If environment dynamic parameters are known and m=n then one of the control laws of system having feedback loops with respect to ![]() can be the following: Theoretically asymptotic stability is provided in proposed control laws by the approximation of the model of medical robot to equation of second other for deviations. Practically the oscillatory processes arise at high speed approach to robot tool, especially when soft tissue covers a stiff bone.
can be the following: Theoretically asymptotic stability is provided in proposed control laws by the approximation of the model of medical robot to equation of second other for deviations. Practically the oscillatory processes arise at high speed approach to robot tool, especially when soft tissue covers a stiff bone.
The force transients when the robot tool penetrates in patient’s soft tissue covering the stiff bone with various approach velocities are presented in figure 3. It is necessary to notice occurrence of significant forces Fz and zero force value at separation of a tool from soft tissue. The force error dependencies on approach speed Vz0 are given on figure 4. At various elasticity coefficients of environment Ke. To reduce overloads it is necessary to measure distance to a surface, for example, with a location sensor. Given above graphs are taken for robot with stiff drives when robot inertia, stiffness and viscosity are much higher than biological soft tissue ones. If robot hand is lightweight and drives are soft then the interaction of robot and environment can be without vibrations.
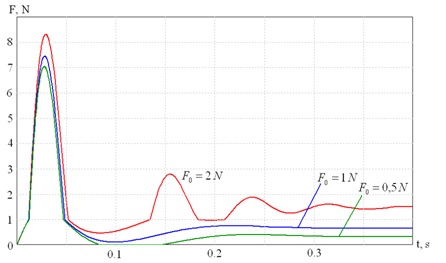 Figure 3: Force transients curves at approach speed 100 mm/s.
Figure 3: Force transients curves at approach speed 100 mm/s.
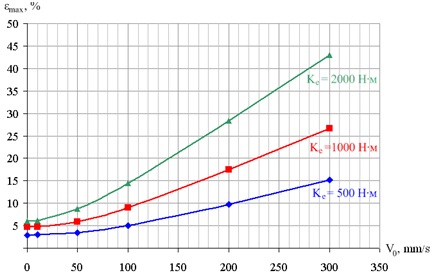 Figure 4: Force error dependencies on approach speed Vz0.
Figure 4: Force error dependencies on approach speed Vz0.
SUBSYSTEM OF BIOTECHNICAL CONTROL IN ROBOTIC SYSTEM FOR RESTORATIVE MEDICINE
Usually in medical robotics the performing assigned movements is considered although the providing of biological efficiency is the general aim.In this work the biotechnical control system task can be formulated as terminal control task of final state: it is necessary to synthesize such input mechanic influences on the patient which during θ = t1 - t0 provides transfer from an initial person’s state B in normal state B0.
Where B0 is vector of assigned normal variables of psychophysiological patient’s state, B is vector of real variables of psychophysiological patient’s states, θ = t1 - t0 is time transition from an initial person’s state in normal one.If physiological variables of the patient’s state are measured then there is a possibility to control them rationally, for example, supporting them in a normal range. The present restorative medical apparatus carry out the assigned mechanical influences on the patient (a massage, movements of extremities in joints, a post-isometric relaxation, a mobilization), but they do not estimate objectively therapeutic effect. Nevertheless, during a series of sessions or during one session of restorative medicine it is possible to observe changes of some physiological patients’ parameters to estimate efficiency of therapy and to change the plan of procedures, i.e., to control restorative medicine procedure. The muscular tone and electric skin resistance are the most informative physiological parameters of the patient’ state. These parameters, despite on hindrances from patient’s mentality respond on restorative medicine influences, providing a relaxation or mobilization of the patient [7]. Let us consider automatic control of the patient’s state for some massage phases when electric skin resistance is the main controlled variable of system (Figure 5). Possibility of such control is given by experimental curves in experiments with influence of a certain massage modes on electric skin resistance (Figure 6).In figure 6 the exponential increase of electric skin resistance is visible at relax massage influence during 270 s and decrease of electric skin resistance at mobilization massage influence during 150 s.Many experiments show the exponential increase of electric skin resistance at relax massage. Relax massage includes drainage modes: squeezing, kneading and stroking, which are carried out slowly and continuously at a rate of 50 mm/s. The duration of increase of electric skin resistance to the established value for various patients is various and is 4 - 15 minutes. The exciting massage modes, as a rule, cause decrease of electric skin resistance. The quick massage modes, including impact ones, use as exciting techniques. The speed of the devices is about 200 mm/s, the duration of decrease of electric skin resistance to the established value is about one minute.
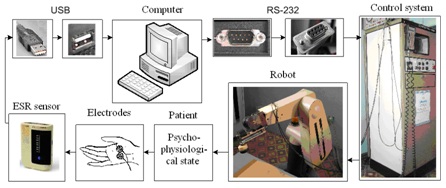 Figure 5: Robotic system for restorative medicine with biotechnical control on signal of electric skin resistance on the basis of Puma-560 robot.
Figure 5: Robotic system for restorative medicine with biotechnical control on signal of electric skin resistance on the basis of Puma-560 robot.
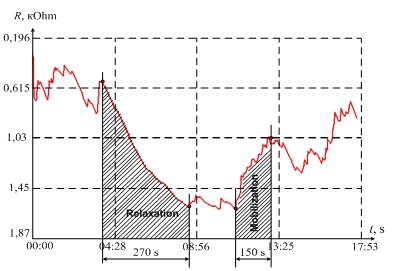 Figure 6: Curve of electric skin resistance in a massage session.
Figure 6: Curve of electric skin resistance in a massage session.
SUBSYSTEMS OF COMMAND, MANUAL PERFORMANCE OF PROCEDURE BY A PHYSICIAN, INDIVIDUAL AND MUTUAL PERFORMANCE OF PROCEDURE BY THE PHYSICIAN AND ROBOT
Subsystem of command robot control is necessary for robot training by physician-operator. For training of assigned trajectory X0 with necessary force of interacting of robot tool with patient’s soft tissues F0 two methods were proposed: the training of force points and training of continuous trajectory by means of teacher showing. The trained force points except position and orientation of geometric coordinates X0include coordinates of force vector F0. So trained force point A in general case can be represented by eighteen-dimensional vector:
Where n, s and a are the three-dimensional orientation subvectors, p is the three dimensional subvector of tool position and F and M are three dimensional subvectors of force and torques. The force points have to be measured fairly accurately so the basic robot has to be precision and stiff. The force training allows performing the second phase of the position/force control as a positional tracking [10,11]. This enables to use as a base usual robots without force correction tracking. If a robot is able to perform the force correction then the quality of control generally increases. On figure 7 the curve L0(X0, F0) represents the trajectory of the robot tool when
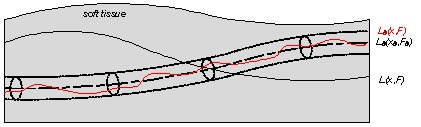 Figure 7: The position/force control accuracy in position or force training.
Figure 7: The position/force control accuracy in position or force training.
The curve L(X, F) represents the trajectory of the robot tool after usual position training which depends primarily on surface relief. The curve L0(X, F) represents the trajectory of the robot tool after force training when the required accuracy is achieved.At Moscow State Industrial University the robot performing massage and extremities movement’s techniques has been developed [8]. A basis of this robot is the industrial PUMA-560 robot that has anthropomorphic manipulator. On the end link a force module containing a strain gauge is mounted. Necessary efforts are made and supervised by position/force control system expanding possibilities of the standard robot.The second method of training of continuous trajectory by means of teacher showing supposes soft backdrivable robot. In this case robot drives have to be compliant in order not to interfere with the training. The control system unloads robot hand from gravitation. In this case open kinematic robot chain, as more compliant, may be preferred. High position robot accuracy is not necessary. After training the written trajectory can be corrected to consider assigned forces. Ergonomically this method of training is more adaptive to the physician-operator and to patient using to perform the training more quickly.Subsystem of individual robot control is necessary for family use without physician-operator. In this mode patient controls robot himself. He can use programs and trained points and curves from previous sessions or he can correct them.Subsystem of mutual performance of procedure by physician and robot is necessary when some fine techniques have to be performed by physician and robot has to assist him. In the scheme of interaction between components of system physician- operator, robot and patient (Figure 1) the mutual performance of procedure by physician and robot can include all 10 connections. This regime permits to work without enclosure, to organize ergonomic interaction of human and robot in common work area and to increase efficiency.New relations between the robot and the person arise not only in a medical robotics. In non-structured environments and extreme situations, the robot should not be “stupid” but the intellectual assistant to the person. There are problems of equality of rights at interaction of the robot and the assembly worker on the conveyor, when in unscheduled situations, the assembly worker not only controls the robot but also he adapts to its work, providing both the friendly interface and his own safety.
PROBLEMS OF INTELLIGENT ERGATIC ROBOTIC SYSTEMS CONTROL
Although every component of ergatic robotic system has certain independence but we need to prioritize. The efficiency to fulfill the objective is increased significantly when these components are connected through a knowledge base. Moreover, who should make the final decision: the doctor or the patient? For example, the procedure can be unpleasant and painful for the patient. May be in this case of conflicts between physician-operator and patient the priority has to be given to physician-operator.The certain rules of behavior have to be laid down in the knowledge base, for example, with using of production rules defined on the basis of the medical experience. The human presence in system causes a number of uncertainties, so production rules can be formed in terms of fuzzy logic or random processes [8].The discreteness of the process can cause the oscillation and system instability. Also instability can be caused by bad choice of membership functions in fuzzy control.Problem-oriented language for control by robot should be close to the natural human language. The creating of a system of dialogue control with the robot in a natural language is perspective one.The development of control and training panel is significant ergotic problem. It has to be comfortable for physician-operator but not an engineer-operator and has to be comfortable especially in case of individual robot control. In any case the priority has to be given to human but not a robot.
SAFETY PROBLEMS
• Check of drives in the beginning of procedures and also the force sensor in programmed control points
• Performance of the first movements with the minimum forces
• Drives placing not in a robot hand but on a platform that will provide small inertia and easiness of a hand
• Soft non-electro conductive covering of robot hand and placing of tactile sensors on wrist and hand of the robot
It is necessary to show the current values of mechanical and biomedical variables on the monitor and to allocate area of the deviations, warning with sound and light signals about the approach to the danger.
Some connections between components of system form the closed rings. Therefore, it is necessary to provide stability of these contours.
The considered requirements of safety should be taken into account by creating of the hardware interface between the doctor, the patient and the robot and also by language developing.
POSSIBLE MEANS OF PREVENTION OF DANGER ARE THE FOLLOWING:
• Switching-off of drives on signal of the maximum force sensor which is connected to position/force control system or abduction of a robot arm according to biomedical signals
• Check of drives in the beginning of procedures and also the force sensor in programmed control points
• Performance of the first movements with the minimum forces
• Drives placing not in a robot hand but on a platform that will provide small inertia and easiness of a hand
• Soft non-electro conductive covering of robot hand and placing of tactile sensors on wrist and hand of the robot
It is necessary to show the current values of mechanical and biomedical variables on the monitor and to allocate area of the deviations, warning with sound and light signals about the approach to the danger.
Some connections between components of system form the closed rings. Therefore, it is necessary to provide stability of these contours.
The considered requirements of safety should be taken into account by creating of the hardware interface between the doctor, the patient and the robot and also by language developing.
CONCLUSION
• Ergonomics of medical robotics and especially in restorative medicine robotics has to consider not only dynamics and psychophysiology of physician-operator but also a patient
• At extended understanding ergonomics the accounting of the patient causes necessity to consider a lot of new subsystems
• The appearance of compliant and backdrivable robots, working without enclosure, allows to organize ergonomic interaction of human and robot in common working area and to increase efficiency
ACKNOWLEDGEMENT
The scientific work described in this paper was supported by Russian presidential grant ? ??-5826.2016.8.
REFERENCES
- Munipov V, Zinchenko V (2001) Ergonomics: Person-oriented designing of technics, software and environment. Logos 356.
- Yushchenko A (2013) Man and robot - compatibility and interoperability. Proceedings of the 7th International Symposium Extreme Robotics, 7th IARP RISE-ER'2013 St. Petersburg, RTC, Russia, pg no: 40-46.
- http://novtex.ru/mech/annot2003_08.htm#8
- Naichenko M, Rizchenkov S (2011) What is medical ergonomics? Forth Russian Multiconference on control problems. Divnomorsk, Russia.
- Golovin, V, Samorukov A (1998) Massage method and device for its implementation, Russian patent? 2145833.
- Birukov A, Savin D, Yarovoi V (2007) Selection of table height for performing Russian massage. Journal Massage, body esthetics 7: 7-12.
- Golovin V, Arhipov M, Zhuravlev V (2011) Ergatic and biotechnical control in medical robotics. Journal Mechatronics, Automation, Control 18: 54-56.
- Golovin V, Arkhipov M, Zhuravlev V (2012) Robotics in restorative medicine. LAP LAMBERT Academic Publishing, Germany.
- Vukobratovic M (2009) Dynamics and robust control of robot - environment interaction. World Scientific Publishing Company, Singapore.
- Golovin V, Arkhipov M, Zhuravlev V (2014) Force Training for Position/Force Control of Massage Robots. In: Rodi? A, Pisla D, Bleuler H (eds.). New Trends in Medical and Service Robots, Mechanisms and Machine Science. Springer International Publishing, New York, USA.
- Golovin V, Arhipov M, Zhuravlev, V (2014) Position/force control of medical robot interacting with dynamic biological soft tissue. Advances on Theory and Practice of Robots and Manipulators, Springer International Publishing, NY, USA.
Citation: Arkhipov M, Golovin V, Kocherevskaya L, Vzhesnevsky E, Uglev A, et al. (2017) ?xpansion of Ergonomic Function in Medical Robotics. J Altern Complement Integr Med 3: 031.
Copyright: © 2017 Maksim Arkhipov, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.