Efficient Rehabilitation of Vergence Accommodation in Children: A Case Study
*Corresponding Author(s):
Zoï KapoulaIris Laboratoire De Physiopathologie De La Vision Et Motricite Binoculaire, Université Paris Descartes, Paris, France
Tel:+33(0) 142864039,
Email:zoi.kapoula@gmail.com
Abstract
Background: Disorders of binocular vision are frequently due to the vergence eye movement abnormalities and their synergy with accommodation. Nowadays, it is a public health problem, as it concerns many children, adolescents and young adults.
Material: We report here a new efficient rehabilitation protocol (patent W02011073288, see Kapoula et al. 2016) applied for a 9 years old child and fourteen years old adolescent. This method called double step vergence protocol has been used previously exclusively for saccades. The double step vergence protocol was applied for vergence training, during four sessions of 15min, and vergence and accommodation were recorded before, during, and after the rehabilitation procedure.
Results: After the rehabilitation, the latency of vergence decreased, the amplitude increased as well as its mean velocity increased. Importantly the accommodation taking place during the convergence and the disaccommodation during the divergence became significantly faster following training with the double step vergence protocol. The benefits were spread to saccades and to both components of combined saccade vergence eye movements.
Conclusion. The study provides convincing evidence for fast vergence - accommodation neuroplasticity in both the child and the adolescent and supports further clinical research and use of this method.
Keywords
Accommodation; Combined saccade vergence eye movements; Double step in depth; Saccades; Vergence rehabilitation
INTRODUCTION
The problems of vergence are frequent, including for children [1]. The consequences are multiple: blurred vision, intermittent diplopy, headaches, attention disturbance, and interference with learning abilities [2].
Orthoptic reeducation is classically used to cope with this problem. Yet, the methods of orthoptists are still empirical, with no objective measurement of eye movements and thus lack of temporal aspects of eye movement dysfunction and improvement following reeducation. Recently, Kapoula et al.[Remove] [3] introduced a research based method coupled with video eye movement recording and analysis. It allows to perform a fine diagnosis of abnormalities including their temporal aspects; and also to rehabilitate the efficiency of eye movement with a learning algorithm, i.e. double step of vergence target.
The double step target for inducing eye movement learning has been extensively used but only for saccades. The study of Kapoula et al.,[3] was carried out in young students and introduced the clinical use in depth of this double step method for targets. The study showed that four weekly sessions of thirty five minutes each are sufficient to restore normal eye movement properties: the latency of the vergence decreased the variability of the amplitude of vergence decreased, as well as its duration and its speed increased. Clinically, the symptoms disappeared, and at least for some subjects, stereovision improved (measured with the TNO stereo acuity test). Orthoptic clinical testing also showed improvement: the Punctum Proximum of Convergence (PPC) decreased while convergence measured with bar prism increased. (Daniel et al., 2016) [4] showed that vergence improvements obtained with this method are spread to saccades during reading: saccades are better coordinated (reduction of the disconjugacy). Interestingly, fixation duration also decreased, and this indicates a cognitive facilitation built upon better binocular motor control: as the eyes are better yoked, single binocular vision of the words is obtained faster thus facilitating reading. Morize et al., [5] have shown that large saccades at any depth (20, 40 or 150 cm from the observer) are also improved after vergence rehabilitation with the vergence double step paradigm: again the latency decreased, the accuracy as well as the binocular coordination control of saccades improved. Moreover, following vergence rehabilitation with the double step, postural control improved in terms of reduction of energy needed to keep the body stable in quiet stance (decrease of mean power frequency of body swing with eyes opened or closed [6]).
The purpose of the present study was to apply for the first time this method in a child and a teenager and to test whether fifteen-minute training for four sessions would lead to an improvement of eyes movement efficiency. Extensive recordings with two types of eye trackers were done before, during and after the training sessions to understand the physiologic process of oculomotor neuroplasticity. Results show improvements of eyes movements particularly in the temporal aspects, including accommodative acceleration, and stimulate further research and clinical use of the double step paradigm.
MATERIAL AND METHODS
The investigation adhered to the tenets of the declaration of Helsinki and was approved by the human experimentation committee, Comité de Protection des Personnes Ile de France II, 2O15-A01100-49. Written consent was obtained from each subject and his/her parents.
PARTICIPANTS
A nine years old child (AD) and a fourteen years old adolescent (LK) years old participated in the study.
ORTHOPTIC TESTING
An extensive orthoptic testing was done. The visual acuity for both was found to be 10/10 for both eyes. Binocular vision was evaluated with the Titmus stereo-acuity test. The stereo-acuity was found to be 80 sec of arc for AD, and 40 sec of arc for LK. For vergence, normal reference values were taken from the study of Von Noorden et al., [7]. Relative to normal values, AD showed rather remote Near Point of Convergence (NPC=8 cm); he also showed mild weakness of both convergence (at far, 20 diopters, at near 25 diopters) and divergence (at far6 diopters, at near 10 diopters). For LK, vergence values were also weak relative to normal (convergenceat far 12 diopters, at near 20 diopters; divergence at far 4, at near 12 diopters). Thus, the orthoptist suggested for vergence rehabilitation in both the cases.
DEVICE FOR OCULOMOTOR TESTS
Oculomotor tests were performed in mesopic light conditions; subjects sat in front of the REMOBI device (patent US8851669, WO2011073288), which was placed at 20cm of the eyes, at eye level. Stimuli of this visual display were red LEDs displayed at different distances always in the horizontal plane (0°, Figure 1A). LED characteristics were: nominal frequency 626nm, intensity 180mCd, and diameter 3 mm. Adjacent to each LED was embedded a buzzer with the following characteristics: nominal frequency approximately 2048Hz, sound pressure level >= 70dB, diameter 12 mm.
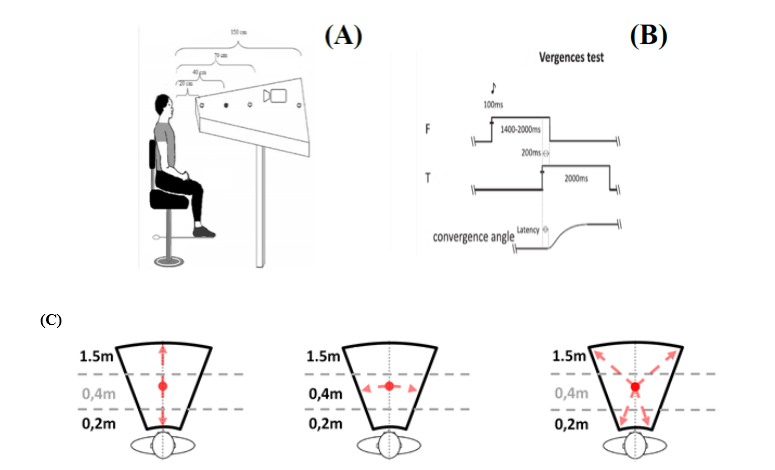 Figure 1A, 1B & 1C: Spatial (A) and temporal (B) arrangement of vergence test. Subjects are looking successively at different LEDs; from the initial (40cm) fixation LED, to, the target LED for divergence (150cm) or the target LED for convergence (20cm). Each trial starts with the fixation target that appears for a variable period of 1200 to 1800ms; following this period the target LED lights are on for 2000ms together with a paired buzzer preceding 50 ms and lasting only 100ms; the fixation LED switches off 200ms after the onset of the target LED (overlap period).(C). Arrows indicate the possible target locations for each test.
Figure 1A, 1B & 1C: Spatial (A) and temporal (B) arrangement of vergence test. Subjects are looking successively at different LEDs; from the initial (40cm) fixation LED, to, the target LED for divergence (150cm) or the target LED for convergence (20cm). Each trial starts with the fixation target that appears for a variable period of 1200 to 1800ms; following this period the target LED lights are on for 2000ms together with a paired buzzer preceding 50 ms and lasting only 100ms; the fixation LED switches off 200ms after the onset of the target LED (overlap period).(C). Arrows indicate the possible target locations for each test.
Eye movement recording
EyeSeeCam: For both, the child and the adolescent, eye movements were recorded binocularly before and after rehabilitation with a head-mounted video-oculography device, the EyeSeeCam (University of Munich Hospital, Clinical Neuroscience, Munich, Germany) For the adolescent, eye movements were also recorded with the same device during the training sessions.
PowerRef III: For the child AD during the four sessions of rehabilitation, vergence and accommodation were recorded with the remote, infrared optometer PowerRef III at 50 Hz (Plusoptix, Germany). This device was placed at about 1 meter from the child’s eyes in order to obtain measures in optimal conditions. The PowerRef III guarantees an objective measure of both the accommodation (subject refraction) and the vergence for a specific target (Figure 2). These measures were based on the principle of retinoscopy: A small light source is situated near the aperture of a camera lens. With this method the light, from an array of infrared light emitting diodes set eccentric to a CCD camera aperture, is reflected from the eye and captured as a video image. In this video image, a typical brightness profile is seen, captured within the pupil that provides quantitative measures of the direction and degree of the eye’s defocus over a defined working range. The slope of the intensity gradient indicates the degree of the eye’s defocus. Information on the direction of this defocus (hyperopia or myopia) is provided by the sign characterizing the slope of the intensity gradient.
Ocular motor tests
Calibration of the EyeSeeCam device: The standard EyeSeeCam five point calibration was applied using a matrix of laser dots that was presented at viewing distance of 1.5m with peripheral dots displayed at 8.5° rightward, downward, leftward and upward : subject fixated each dot at their own pace, and the total calibration task lasted 14 seconds.
A further calibration task was performed before the vergence test: This task consisted of eight leftward and eight rightward randomly interleaved saccades to LEDs located at 10° and 20° from midsagittal plane of REMOBI, at a distance of 1.5m from the subjects’ eyes.
Vergence test: Each trial started by lighting the LED at 40 cm along the median plane. After a variable fixation period of 1200 to 1800ms, the target LED was lit for 2000ms. The fixation LED was switched off 200ms after the onset of the target LED (overlap paradigm). The lighting of each LED (fixation or target) was accompanied by the corresponding buzzer sound for 100 ms; the sound preceded the LED by 50 ms and lasted 100 ms (see Figure 2B). Such visual-acoustic stimulation aimed to reinforce deployment of attention resources to the LED. The vergence test contained 40 trials, half of them to the far target and the other to the near target. The far one called for a change in vergence angle from 9° to 2°, that is a divergence movement of 7°. The near target LED called for a change of vergence from 9° to 17°, that is a convergence of 8°. Convergence and divergence trials were interleaved pseudo-randomly (see Figure 1C left). Between trials, a blanked period of 300 to 700ms was applied. All eye movement data to be reported here came from this task. This test was done twice; before and after vergence rehabilitation with double step protocol.
Saccade test: Each trial started with the fixation central LED lighting at 40cm from the subject for a randomized period ranging from 1400ms to 2000ms; it was followed by the lighting of the saccade target LED for 2000ms at 20° of eccentricity, randomly chosen on the left or on the right. There were 40 trials (20 left, 20 right, Figure 1C middle).
Combined saccade vergence test: At the beginning of each trial the fixation central LED lighted up at 40cm from the subject’s eyes for a period varying from 1400 to 2000ms. It was followed by the lighting of the target LED for 2000ms randomly at a depth distance of 20cm or 150cm and at 20° left or right. The test contained 80 trials (20 convergent left trials with the target appearing at 20° to the left at 20 cm from the subject’s eyes, 20 divergent trials to the left with the target appearing at 20° left at 150 cm distance, 20 convergent trials to the right, with the target being at 20° right and at 20 cm depth, and 20 divergent trials to the right with the target at 20° right and at 150cm depth, Figure 1C, right).
For all the three tests (saccade, vergence and the combined eye movements), the central fixation LED was switched off 200 ms after the lightning of the target LED (overlap paradigm, Figure 1B).
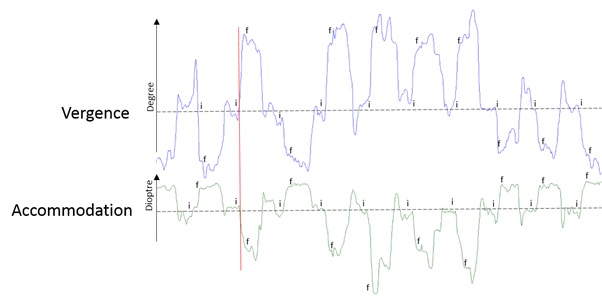 Figure 2:Traces of vergence (blue) and accommodation (green) during a recording with PowerRef III device i: initiation of the vergence or accommodation. f: final position or adjustment of the accommodation.
Figure 2:Traces of vergence (blue) and accommodation (green) during a recording with PowerRef III device i: initiation of the vergence or accommodation. f: final position or adjustment of the accommodation.
Vergence double step rehabilitation protocol
A 15-minute rehabilitation session was applied weekly, or two times a week to both subjects. The rehabilitation sessions contained 5 blocks sequenced as follows: 1 block of divergence, 4 blocks of convergence. Each block contained 40 trials and lasted 2 to 3 minutes. A 1-minute pause was applied between blocks during which the subject was questioned on whether the LEDs were seen single, double, or blurred at each location; subjects were allowed to stand up and relax while resting.
Briefly, the target for convergence or divergence appeared first to a location (overlap pa; after 200ms, presumably before the accomplishment of the vergence eye movement, the target stepped to a second location. Given that the vergence latency is between 160 and 250ms, and vergence execution lasts between 350 and 550ms, it is almost certain that the second step of the target occurred before the initial vergence eye movement has been made. This double-step protocol for clinical purposes is part of the patent.
Vergence, saccade, combined eyes movements before and after rehabilitation
To evaluate the effect of the retention of the rehabilitation, the vergence test (single step) described above was done before, a week, 3 months, and a year after the end of the rehabilitation for child AD. For LK the vergence test (single step) was done before and 3 months after the 4 sessions of rehabilitation, as well as at the end of each of the four rehabilitation sessions. For child AD, at the end of each rehabilitation session, vergence and accommodation were also measured with the remote Poweref device described above.
DATA ANALYSIS
Data recorded with EyeSeeCam was analysed with AEMA, software developed in the IRIS laboratory. The beginning and end of the vergence movements were defined as the time point when the eye velocity exceeded or dropped below 5°/s: these criteria are standard and were applied automatically by the AEMA software. Trials with blinks or other artefacts were discarded. Saccade onset and offsets were automatically detected by the AEMA software: the onset and offset of the saccade was marked as the time when the velocity signal exceeded or dropped respectively below 10% of the maximum velocity. For combined movements decomposed to their saccade and vergence components, the same respective criteria as above were used.
Data recorded with PowerRef III were analysed with the software VERAC, also developed by IRIS lab. The investigator scrutinized the vergence and accommodation traces as well as the vergence velocity on a computer screen; the 5°/s criterion was applied for the onset and the offset. Thus, was measured the duration and the amplitude of the convergence, of divergence, of the accommodation and of the desaccommodation (Figure 2).
STATISTICAL ANALYSIS
Statistical analyses of all sessions were made on the software STATISTICA. Student’s t-test were done on the sessions before and after the four double step rehabilitations, or for comparison between sessions of rehabilitation.
RESULTS
Effect of double step protocol: before and after results
Figure 3 shows for each participant eye movement traces for vergence recorded with the EyeSeeCamdevice before (A, C) and after (B, D) rehabilitation with the double step paradigm. Upward inflection indicates convergence and downward divergence. Traces of many successive trials are offset at zero time point, i.e., when the target LED was switched on. The horizontal lines indicate the target for convergence or divergence, respectively. For the child AD, the traces before rehabilitation (Figure 3A) show hypometria, particularly for convergence. Thevelocity was slow, as the trajectory of the movement looks rather linear sometimes. Similar observations can be made for the adolescent (Figure 3C). After rehabilitation, for both the child and the adolescent, the trajectories of both convergence and divergence look faster.
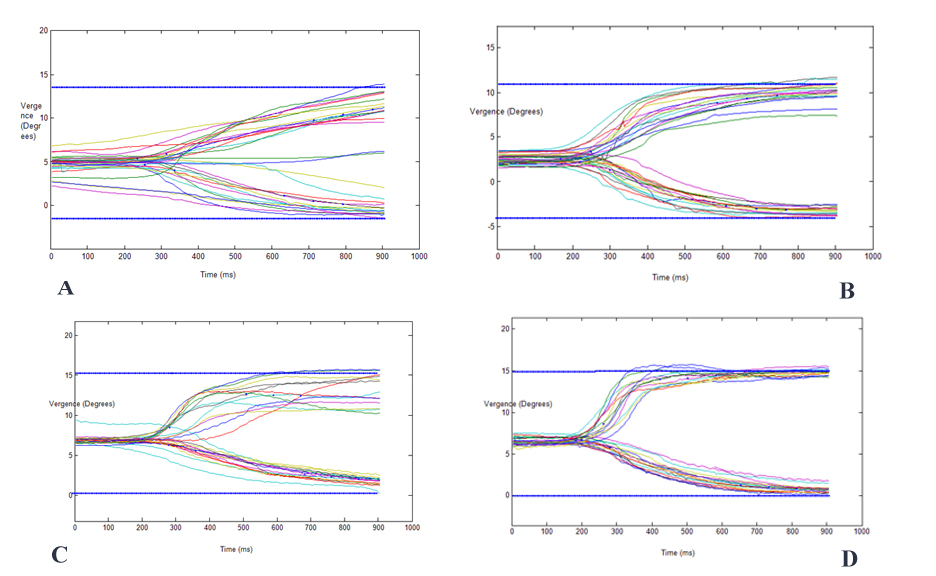 Figure 3:Traces of vergence movements before and after four sessions of rehabilitation from subject AD (A,B) and LK(C,D).
Figure 3:Traces of vergence movements before and after four sessions of rehabilitation from subject AD (A,B) and LK(C,D).
Quantitative results and statistical values are shown in Table 1. For child AD, convergence latency, but not divergence, decreased significantly (p<0.001). The mean velocity increased significantly for both convergence and divergence. Finally, the mean amplitude decreased significantly for convergence only. The coefficient of variability (Standard Deviation/Mean*100, CV) indicated rather normal values (around 20%,[3]) except one case (convergence duration after 3 months for subject AD, CV=33%). For the adolescent LK, the latency decreased significantly for divergence, the mean velocity of both convergence and divergence increased significantly, as well as the amplitude of both convergence and divergence increased significantly. In several instances the coefficient of variability decreased, for instance for the amplitude, the CV dropped from 18 to 13 for convergence for child AD (p=0.037), and from 31 to 6 for divergence for adolescent LK (p<0.001). Thus, in line with the study of Kapoula et al., the data shows significant improvement of latency and/or of speed, or reduction of amplitude’s variability [3].
|
ID |
Latency |
Duration |
Velocity |
Amplitude |
|||||
|
AD |
Convergence |
Mean / C.V. |
Students test |
Mean / C.V. |
Students test |
Mean / C.V. |
Students test |
Mean / C.V. |
Students test |
|
Before |
235 / 21 |
430 / 12 |
5 / 0 |
8.11 / 18 |
|||||
|
After |
177 / 16 |
p=0.0006 |
452 / 21 |
p=0.36 |
15/ 20 |
p<0.0001 |
7.16 / 13 |
p=0.037 |
|
|
3 months |
278 / 22 |
p=0.0191 |
118 / 33 |
p<0.0001 |
38 / 18 |
p<0.0001 |
9.74 / 19 |
p=0.0037 |
|
|
1 year |
255 / 23 |
p=0.25 |
165 / 27 |
p<0.0001 |
23 / 22 |
p<0.0001 |
6.09 / 14 |
p<0.0001 |
|
|
LK |
Before |
211 / 21 |
221 / 13 |
18 / 28 |
5.81 / 31 |
||||
|
After |
183 / 21 |
p=0.09 |
246 / 26 |
p=0.31 |
29 / 24 |
p<0.001 |
7.71 / 6 |
p<0.001 |
|
|
Divergence |
|||||||||
|
AD |
Before |
255 / 20 |
438 / 27 |
4 / 0 |
5.53 / 18 |
||||
|
After |
227 / 19 |
p=0.12 |
395 / 15 |
p=0.17 |
13 / 15 |
p<0.0001 |
5.5 / 6 |
p=0.23 |
|
|
3 months |
288 / 14 |
p=0.029 |
271 / 10 |
p<0.0001 |
14 / 17 |
p<0.0001 |
5.05 / 21 |
p=0.1471 |
|
|
1 year |
228 / 22 |
p=0.1119 |
290 / 9 |
p<0.0001 |
17 / 12 |
p<0.0001 |
4.57 / 19 |
p=0.0031 |
|
|
LK |
Before |
290 / 24 |
437 / 17 |
09 / 22 |
4.86 / 21 |
||||
|
After |
199 / 16 |
p<0.001 |
443 / 17 |
p=0.84 |
11 / 18 |
p=0.02 |
5.74 / 14 |
p=0.01 |
|
Table 1: Eye movement parameters (latency, duration, velocity, and amplitude) for convergence and divergence for AD and LK before and a week after the rehabilitation, for AD data are also shown 3 months and a year after the rehabilitation.
Evolution of accommodation and/or vergence at the end of each training session
The single step vergence test was done at the end of each neurorehabilitation session. For child AD, the measurement of vergence and accommodation was done with a remote device (PowerRef III Plusoptix). For adolescent LK, the measurements were done with the EyeSeeCam device.
Evolution for child AD
Figure 4A shows the evolution of duration and amplitude for convergence and divergence. Convergence amplitude and duration weren’t significantly modified from session 1 to session 4, even though the duration of convergence tends to decrease, going from 320ms during the first session to 251ms in session 4. However, the double step protocol had an important impact on divergence, especially on its duration, which significantly dropped from 400ms in the first session, to 120ms during the third session (t=3.2, p=0.033), finally reaching 255ms at the end of the final rehabilitation session. Divergence’s amplitude was not significantly modified all along the training, but was close to the required amplitude of 6.5 degrees.
Figure 4B shows the amplitude and the duration for accommodation whichwas deeply and rapidly impacted by the double step protocol as its power significantly increased from -1.6δ to -2.9δ (t=-2.67, p=0.020) from session 1 to session 2, and stayed stable around the required amplitude (-2.5δ) during the following sessions (session 3: -2.8δ, t=-2.79, p=0.020; Session 4: -2.91δ, t=-2.42, p=0.031). The duration also decreased from 420ms during the first session to 265ms during the second session. It also stayed stable around 275ms, a good physiological duration, during the following sessions (for the third session: 300ms; for the fourth session: 260ms). Desaccommodation was not significantly modified through the four sessions, for its power was already near the required value during the first session (theoretical: 1.9δ, measured value: 1.8δ).For session 2 the measured value was 1.28δ; and for session 4 it went up to 2.8δ. Session 3 was not analyzed because of a lack of sufficient data without blinks during this recording.
This recording with the PowerRef device givesanother way to look at the modifications brought by the double step protocol during the training. Even if the sampling frequency of the PowerRef III is lower than that of the EyeSeeCam device (25 vs 220 Hz), the former gives additional information on accommodation. These results show that rehabilitation has a rapid impact not only on vergence, but also on the accommodation, particularly its duration.
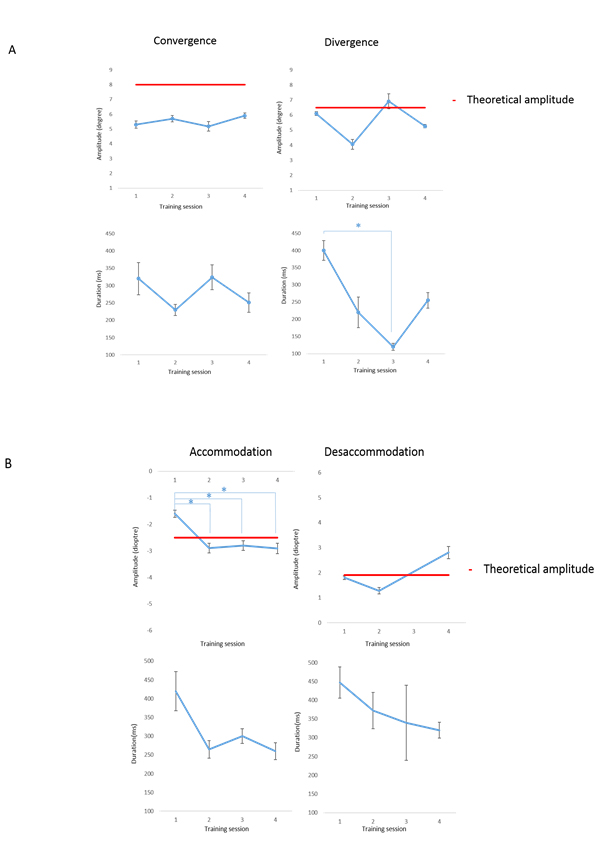 Figure 4:Evolution of amplitude and duration for convergence and divergence (A), accommodation and desaccommodation (B) for child AD. Target values are shown with a red line. *: p<0.05
Figure 4:Evolution of amplitude and duration for convergence and divergence (A), accommodation and desaccommodation (B) for child AD. Target values are shown with a red line. *: p<0.05
Evolution of vergence for LK
Figure 5 shows the evolution of vergence movements measured at the end of each session of the rehabilitation. Her vergence movements evolved to become progressively faster, more reproducible and accurate.
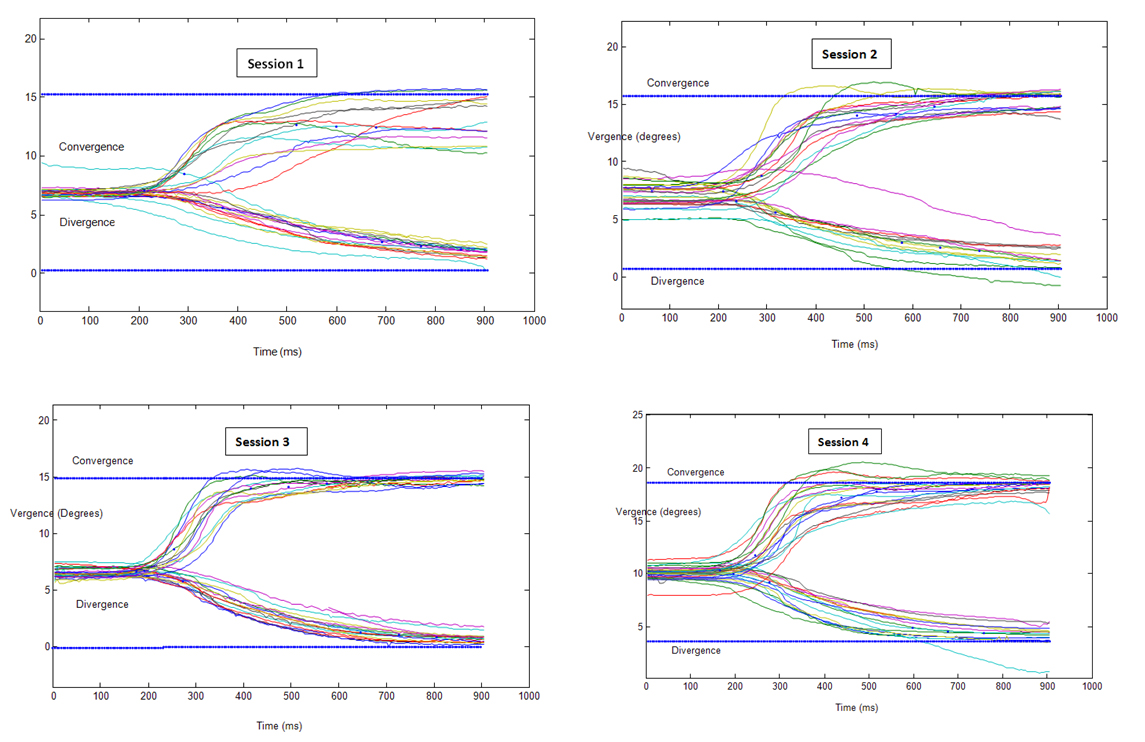 Figure 5: Traces of vergence movements for the adolescent LK during the four sessions of rehabilitation.
Figure 5: Traces of vergence movements for the adolescent LK during the four sessions of rehabilitation.
Her mean values for each eye movement parameter together with the coefficient of variability for each session are shown in Table 2. Convergence and divergence movements changed rapidly from one session to another: in the second session, convergence amplitude was already significantly higher than before, with an increase in amplitude of 2 degrees (t= -3.46, p=0.002); divergence latency dropped from 290ms to 237ms (t= 2.32, p=0.029). In the third session, results were even more visible with significantly higher amplitude, latency and velocity for both convergence and divergence relative to the first session: Convergence amplitude remained high (7.47 degrees, t=-3.74, p<0.001) while divergence’s amplitude rose from 4.86 degrees in the first session to 5.62 degrees (t=-2.42, p=0.022). The velocity also increased significantly from 18 degree/s to 29 degrees/s (t=-4.21, p<0.001) for convergence and from 9 degrees/s to 13 degrees/s for divergence (t=-3.20, p=0.004), and the latency dropped both for convergence (166ms, t=3.36, p=0.002) and divergence (196ms, t=4.94 p<0.001). After the fourth session of rehabilitation with the double step protocol, every aspect of convergence and divergence except duration were significantly modified relative to the first session: amplitudes were at 7.71 degrees (t=-3.82, p<0.001) for convergence, and 5.74 degrees (t=-2.62, p=0.014) for divergence; the velocity stayed at 29 degree/s (t=-4.13, p<0.001) for convergence and 11 degrees/s (t=-2.53, p=0.020) for divergence; latency stayed below 200ms at 183ms (t=1.72, p=0.099) for convergence and 199ms (t=4.77, p<0.001) for divergence. Thus the double step protocol on teenager’s eye movements caused major benefits after only one session and the improvement evolved or stabilized on the following sessions.
|
Subject LK |
Latency |
Duration |
Velocity |
Amplitude |
||||
|
Convergence |
Mean / C.V. |
Students test |
Mean / C.V. |
Students test |
Mean / C.V. |
Students test |
Mean/ C.V. |
Students test |
|
Session 1 |
211 /21 |
221 / 13 |
18 / 28 |
5.81 / 31 |
||||
|
Session 2 |
210 / 20 |
p=0.91 |
244 / 28 |
p=0.37 |
23 / 30 |
p=0.058 |
7.84 / 13 |
p=0.002 |
|
Session 3 |
166 / 18 |
p=0.002 |
232 / 18 |
p=0.49 |
29 / 24 |
p<0.001 |
7.47 / 9 |
p<0.001 |
|
Session 4 |
183 / 21 |
p=0.099 |
246 / 26 |
p=0.31 |
29 / 24 |
p<0.001 |
7.71 / 6 |
p<0.001 |
|
Divergence |
||||||||
|
Session 1 |
290 / 24 |
437 / 17 |
9 / 22 |
4.86 /21 |
||||
|
Session 2 |
237 / 21 |
p=0.029 |
382 / 14 |
p=0.089 |
10 / 30 |
p=0.55 |
5.2 /24 |
p=0.45 |
|
Session 3 |
196 / 14 |
p<0.001 |
401 / 18 |
p=0.29 |
13 /23 |
p=0.004 |
5.62 / 12 |
p=0.022 |
|
Session 4 |
199 / 16 |
p<0.001 |
443 / 17 |
p=0.85 |
11 /18 |
p=0.020 |
5.74 / 14 |
p=0.014 |
Table 2: Evolution of eye movement parameters (latency, duration, velocity, and amplitude) for convergence and divergence for subjects LK recorded at the end of each session of rehabilitation. Student tests were done between the first and the second, third and fourth session.
Additional Observations: Spread of benefits to other eye movements
Saccades: Figure 6 shows typical trajectories of saccades before and after a week of four sessions of rehabilitation. For the child AD, the variability in latency during the first session was very high: latency values varied between 200ms and 550ms. Saccades often involved several secondary corrective movements to reach the target that is indicated by the red line. Once the target was reached, there was often a return to the initial point of fixation (0°) in an anticipating way before the offset of the target. After the vergence rehabilitation, saccade latency variability decreased drastically, and all saccades were now triggered with latency between 200ms and 400ms; the primary saccade brought the eyes closer to the target, and stayed on the target without anticipating the return back to the initial position.
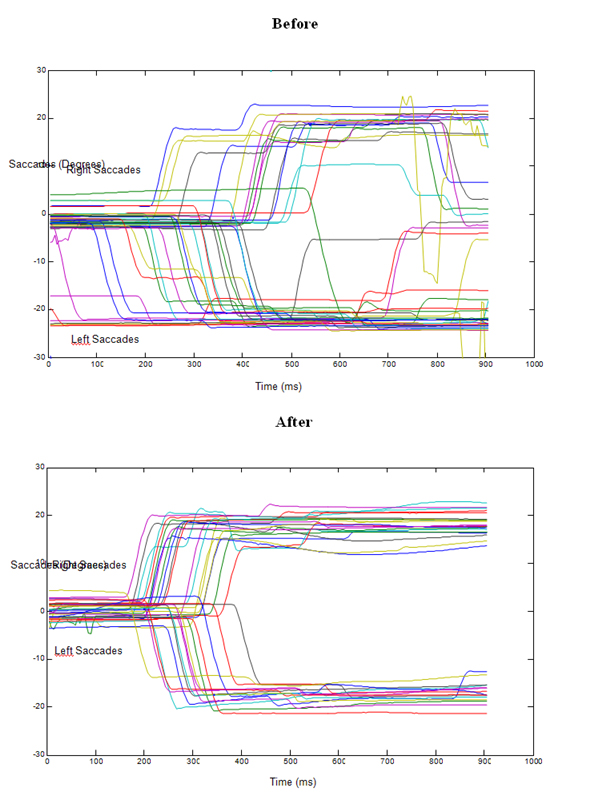 Figure 6: Traces of saccade movements for subject AD before (top) and after (bottom) the four sessions of rehabilitation.
Figure 6: Traces of saccade movements for subject AD before (top) and after (bottom) the four sessions of rehabilitation.
To summarize, the main result of the rehabilitation was the significant drop of the latency (Table 3): Right saccade’s initiation was reduced from 372ms to 234ms after the rehabilitation (t=5.33, p<0.001) and left one was reduced from 295ms to 253ms (t= 2.04, p=0.049). Duration and velocity also tend to improve, but without a significant difference.
|
Subject AD |
Latency |
Duration |
Velocity |
Amplitude |
||||
|
Right Saccade |
Mean / C.V. |
Students test |
Mean / C.V. |
Students test |
Mean / C.V. |
Students test |
Mean / C.V. |
Students test |
|
Before |
372 / 26 |
72 /11 |
259 /13 |
18.06 /16 |
||||
|
After |
234 / 24 |
p<0.001 |
69 /4 |
p=0.18 |
252 /7 |
p=0.43 |
17.47 /7 |
p=0.42 |
|
1 year |
228 / 20 |
p<0.001 |
67 / 9 |
p=0.0097 |
251 / 14 |
p=0.3861 |
17.2 / 14 |
p=0.2407 |
|
Left Saccade |
||||||||
|
Before |
295 /23 |
77 /14 |
236 /16 |
18.52 /21 |
||||
|
After |
253 /23 |
p=0.04 |
72 /6 |
p=0.13 |
261 / 8 |
p=0.064 |
18.78 /10 |
p=0.91 |
|
1 year |
238 / 16 |
p<0.0001 |
75 / 12 |
p=0.4585 |
219 / 11 |
p=0.051 |
16.36 / 6 |
p=0.0022 |
Table 3: Parameters of saccades before and after vergence rehabilitation for subject AD.
Combined Eye Movements
Table 4 shows mean values and the corresponding Coefficient of Variation (CV) for each parameter and for each component of the convergent and of the divergent combined eye movements, together with statistical value (t-test). For right convergent movements, the latencies decreased significantly for both components, going respectively from 354ms to 275ms (t=3.12, p=0.004) for the convergence componentand from 298ms to 256ms (t=2.24, p=0.034) for the saccade component. Durations were significantly reduced for left convergent movements, respectively decreasing from 247ms to 142ms (t=4.03, p<0.001) for the convergence component and from 76ms to 71ms (t=2.25, p=0.031) for the saccade component. Velocity was increased significantly. Fo left convergent movements, the velocity increased from 23°/sec to 40°/s (t=-6.48, p<0.001).For left divergent movements, the velocity of the vergence increased from 22°/s to 29°/s (t=-3.01, p=0.006); for right divergent movements, the velocity of the vergence increased from 17°/s to 20°/s (t=-2.41, p=0.023). The velocity of the right vergence component of convergent movement increased from 227°/s to 276°/s (t=-5.56, p<0.001); the velocity of the left vergence component increased from 231°/s to 252°/s (t=-2.57, p=0.015); the velocity of the left saccade component of divergent movements increased from 223°/s to 252°/s (t=-3.29, p=0.002). Finally, the amplitude improved for the divergence combined with left or right saccades for converging right saccade, and for diverging left saccade, increasing respectively from 3.56° to 4.71° (t=-4.13, p<0.001) for the divergence component combined with right saccades, from 4.39° to 5.3 (t=-2.50, p=0.018) for the divergence combined with left saccades, from 17.06° to 21.4° (t=-4.74, p<0.001) for the saccade component to right combined with convergence, and from 18.36° to 19.81° (t=-3.04, p=0.005) for the saccade component to right combined with divergence. Thus, significant modifications were observed for many parameters of combined eye movements; benefits from the double step rehabilitation method spread to both, saccades and to both components of the combined saccade-vergence movements.
|
Subject AD |
Latency |
Duration |
Velocity |
Amplitude |
||||
|
Divergence to the Right |
||||||||
|
Divergence Component |
Mean / C.V. |
Students test |
Mean / C.V. |
Students test |
Mean / C.V. |
Students test |
Mean / C.V. |
Students test |
|
Before |
263 / 22 |
196 / 27 |
17 /24 |
3.56 / 28 |
||||
|
After |
279 / 17 |
p=0.43 |
181 / 20 |
p=0.44 |
20 / 20 |
p=0.023 |
4.71 / 12 |
p<0.0001 |
|
1 year |
463 / 33 |
p<0.0001 |
21 / 14 |
p<0.0001 |
44 / 34 |
p<0.0001 |
2.27 / 19 |
p<0.0001 |
|
Saccade Component |
||||||||
|
Before |
233 / 17 |
72 / 10 |
237 / 7 |
17.06 / 8 |
||||
|
After |
238 / 19 |
p=0.77 |
73 / 5 |
p=0.82 |
240 / 6 |
p=0.50 |
17.5 / 7 |
p=0.34 |
|
1 year |
250 / 23 |
p=0.2831 |
69 / 8.7 |
p=0.1602 |
239 /5.9 |
p=0.6825 |
16.38 / 7 |
p=0.0943 |
|
Divergence to the Left |
||||||||
|
Divergence Component |
|
|||||||
|
Before |
294 / 21 |
Not enough data |
22 / 23 |
4.39 / 19 |
||||
|
After |
290 / 13 |
p=0.79 |
Not enough data |
29 / 21 |
p=0.006 |
5.3 / 23 |
p=0.018 |
|
|
1 year |
617 / 35 |
p<0.0001 |
5 / 0 |
132 / 33 |
p<0.0001 |
0.64 / 19 |
p<0.0001 |
|
|
Saccade Component |
||||||||
|
Before |
258 / 17 |
83 / 18 |
223 / 7 |
18.36 / 13 |
||||
|
After |
276 / 21 |
p=0.83 |
77 / 10 |
p=0.73 |
252 / 8 |
p=0.002 |
19.81 / 8 |
p=0.005 |
|
1 year |
242 / 21 |
p=0.2994 |
80 / 10 |
p=0.4335 |
241 / 7 |
p=0.0017 |
19.37 / 10 |
p=0.1438 |
Table 4: Parameters of saccade and vergence components of combined eye movements before and after vergence rehabilitation for subject AD.
DISCUSSION
Efficiency of the method
Prior studies [3,4] have shown the efficacy of the vergence double step rehabilitation method for restoring vergence performances in young students. The present study demonstrated for the first time that the method is efficient for both; the child and the adolescent. Indeed, four sessions of only 15 minutes each were sufficient to induce permanent beneficial changes in terms of latency, amplitude, duration and velocity of convergence and divergence. Although anecdotal, the benefits seem to transfer in real life, as for the 9 years old child, there was a clear improvement for reading activities and academic school performances. The adolescent also reported improvements of her sport performances in high school. Presumably, the method of double step in depth stimulated neural oculomotor plasticity efficiently for both cases. It thus can be useful for clinicians in dealing efficiently with problems of vergence in children and adolescents as such problems have negative consequences for learning abilities.
The present study also brings important findings in terms of physiological interaction between vergence and accommodation. For the first time, and by using the complementary technology by PlusOptix (PoweRef III), we were able to measure and quantify the changes in the duration of accommodation during the vergence rehabilitation sessions. The measurements of PoweRef III enabled us to demonstrate the improvement of accommodative responses. It is remarkable that during the vergence, the accommodation or desaccomodation were performed more rapidly. Even though the LED sare not powerful accommodative stimuli, because of the reciprocal interaction between vergence and accommodation, stimulating the vergence system also stimulated the accommodation. Thus, the Remobi vergence double step rehabilitation paradigm improves both vergence and accommodation. Future developmental studies would be of interest to investigate the evolution of vergence accommodation in synergy. Acceleration of accommodation due to vergence rehabilitation is a novel important result.
Another result from the present study is that the benefit from vergence rehabilitation along the median plane spreads to natural combined eye movement in direction and in depth and to lateral saccades. For the first time, it was shown here that for the child with vergence disorders, combined eye movements are improved after vergence rehabilitation as at many instances the latency decreased, or the velocity, or the amplitude increased. As a result, these combined eye movements in space, that are the most frequent movements we make in everyday life, were now executed more efficiently.
CONCLUSION
In conclusion, this study demonstrates remarkable capacity of neural plasticity as stimulated by the Remobi technology that helps to restore efficient vergence in both, the child and the adolescent. The benefits appear rapidly and can spread to the saccades and to the combined saccade-vergence eye movements. Although this study needs further consolidation with a larger population, it has many future implications, including for children with attention deficits and learning disabilities. It is important to note that such methods are urgently needed as a large number of children nowadays are suffering from problems of headache, visual stress and concentration that could be at least partially due to poor vergence control in 3D space.
ACKNOWLEDGEMENT
We thank Christian Schmidt, Plusoptix, for lending us the powered equipment to conduct the study.
REFERENCES
- Rouse MW, Borsting E, Hyman L, Hussein M, Cotter SA, et al. (1999):Frequency of convergence insufficiency among fifth and sixth graders. The Convergence Insufficiency and Reading Study (CIRS) group. Optom Vis Sci 76: 943-949.
- Cooper J, Duckman R (1978) Convergence insufficiency: incidence, diagnosis, and treatment. J Am Optom Assoc 49: 673-680.
- Kapoula Z, Morize A, Daniel F, Jonqua F, Orssaud C, et al. (2016):Objective evaluation of vergence disorders and a research-based novel method for vergence rehabilitation.Transl Vis Sci Technol 5: 8.
- Daniel F, Morize A, Brémond-Gignac D, Kapoula Z (2016) Benefits from vergence rehabilitation: evidence for improvement of reading saccades and fixations. Front Integr Neurosci 20: 10-33.
- Morize A, Brémond-Gignac D, Daniel F, Kapoula Z (2017) Effects of pure vergence training on initiation and binocular coordination of saccades. Invest Ophthtalmol Vis Sci 58: 329-342.
- Morize A, Kapoula Z. Reeducation of vergence dynamics improves posturalcontrol. Neurosci Lett. 2017 Aug 24;656:22-30.
- von Noorden GK, Campos EC (2002) Binocular Vision and Ocular Motility: Theory and Management of Strabismus. Mosby, St. Louis, USA.
Citation: Kapoula Z, Chaturvedi A, Pain E, Morize A, Palpanas T, et al. (2019) Efficient Rehabilitation of Vergence Accommodation in Children: A Case Study. J Clin Stud Med Case Rep 6: 074.
Copyright: © 2019 Zoï Kapoula, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.