Journal of Nephrology & Renal Therapy Category: Clinical
Type: Case Report
Lobar Pneumonia and Glomerulonephritis: An Unusual Association
*Corresponding Author(s):
Sare Gülfem ÖzlüDepartment Of Pediatric Nephrology, Dr Sami Ulus Childrens And Maternity Hospital, Yildirim Beyazit University, Yeni Ziraat Mahallesi, 657. Sk. No:5, Ziraat, 06110 Alt?nda?/Ankara, Turkey
Tel:+90 5057735450,
Email:saredr@gmail.com
Received Date: Apr 19, 2016
Accepted Date: Aug 11, 2016
Published Date: Aug 26, 2016
Abstract
Acute Postinfectious Glomerulonephritis (APIGN) is the most common renal pathology in developing countries and a wide spectrum of infectious agents may be the cause of the disease. The prototype of the disease is acute poststreptococcal glomerulonephritis, but other infectious aetiologies such as Staphylococcus, Pneumococcus, Mycobacteria, Yersinia and various viral, parasitic and fungal infections may also be relevant. APIGN occurs typically 7-14 days after infection but in some cases it can occur concurrently with pneumonia. Here we report a 4 years old girl presented with pneumonia and glomerulonephritis simultaneously. Although we could not detect the underlying aetiology she responded well to appropriate antibiotics and diuretics. We aimed to remind the simultaneous and rare presentation of pneumonia and glomerulonephritis.
Keywords
Child-hood; Glomerulonephritis; Pneumonia
INTRODUCTION
Acute Postinfectious Glomerulonephritis (APIGN) includes a large group of glomerulonephritis that result from a variety of infectious agents [1]. APIGN generally occurs after an infection caused by Group A β-Hemolytic Streptococcus (GABHS) and also to a lesser extent it occurs after staphylococcal, pneumococcal infections and various viral infections like coxsackievirus B, influenza virus and mumps [1] also follows fungal and parasitic infections. Association with pneumonia is rarely reported [2]. Although more commonly seen in adults there are also four small series and few reported cases with pneumonia in the pediatric literature [2-8]. While APIGN typically occurs between 7-14 days after an infection, glomerulonephritis associated with pneumonia usually develops concurrent with pneumonia [3]. Here we report a four years old girl with lobar pneumonia who presented simultaneously with APIGN.
CASE REPORT
A 4-year-old girl presented with cough, fever, dark urine and abdominal pain lasting for over two days. She was daughter of non-consanguineous parents and past medical history was unremarkable. Her father had upper respiratory tract infection one week prior to her complaints. On physical examination her temperature was 38.7 C, pulse rate 135 beats/minute, respiratory rate 40 breaths/minute and blood pressure was 120/70 mmhg (>95th percentile for age, height and sex). She had an erythematous posterior pharynx without exudate. On auscultation respiratory voices were decreased on right basal region. Abdomen was diffusely tender. Other system examinations were normal. Laboratory examinations revealed elevated white blood cells of 16.100/mm3 (87.1% neutrophils, 10.6% lymphocytes, 2.3% band forms) with hemoglobin 8.84 g/dl, and platelets 255.000/mm3. Blood urea nitrogen and serum creatinine levels were elevated at 40 mg/dl (7.9-21 mg/dl) and 1.5 mg/dl (0.39-0.79 mg/dl) respectively. Estimated glomerular filtration rate was found to be 48 ml/min/1.73m2 by Schwartz formula. On microscopic analysis of the urine there were more than 100 erythrocytes and 4-5 leukocytes per high power field. Urine dipstick test revealed proteinuria of 2+. The spot urine protein/creatinine ratio was: 1.4 (mg/mmol) .Serum complement 3 level was 0.159 g/L (0.83-1.77 g/L) and C4 was 0.209 (0.12-0.4 g/L) g/L. Anti-streptolysin O levels were elevated with 612U/ml (<200 U/ml). Blood, urine and pharyngeal swab cultures were obtained before antibiotic administration and all of them were negative. Serological tests for Mycoplasma, Chlamydia were also negative and titers did not elevated on repeated investigations. Viral PCR obtained from nasopharyngeal swabs was also negative. On chest radiograph, there was consolidation on right upper lobe indicating lobar pneumonia (Figure 1). Renal ultrasound showed enlarged kidneys with increased echogenicity bilaterally.
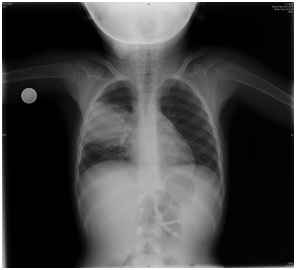
Figure 1: Chest radiograph showing lobar pneumonia on right upper lobe.
She was diagnosed as lobar pneumonia and glomerulonephritis and ceftriaxone and furosemide were started. Successful diuresis begun on the third day of her admission and blood pressure was in normal limits for her age. Also serum creatinine and blood urea nitrogen levels were decreased to 0.6 mg/dl and 20 mg/dl respectively. She was discharged from the hospital on the seventh day with serum creatinine level 0.4 mg/dl and blood urea nitrogen 14 mg/dl. Antihypertensive and diuretic medications were discontinued. On follow up; two months after her hospitalization serum C3 returned to normal limits. Other laboratory parameters were normal. Chest radiograph (Figure 2) was not in normal limits but has markedly improved with some residual consolidation/atelectasis and she did not have any medication.
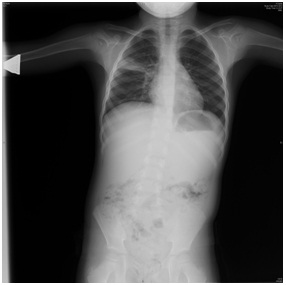
Figure 2: Chest radiograph showing revealing lobar pneumonia.
DISCUSSION
Pneumonia associated glomerulonephritis is a rare condition that occurs more commonly in adults than in children. To our knowledge there are four published series for pediatric patients including 3, 11, 4 and 6 patients [2-5]. In all of these series glomerulonephritis developed soon after pneumonia; macroscopic hematuria developed after 24-72 hours of hospital admission [2,3,5], but in the study of Schachter [4], glomerulonephritis developed within six weeks after the infection. In our patient macroscopic hematuria was observed simultaneously with respiratory symptoms and GFR was decreased when she was diagnosed as pneumonia.
Although all of the patients were male in the study of Srivastava [3], this may be an incidental finding because there are female patients in the other studies and the number of the patients in all series are small to interpretar about this issue. Patients are generally under the age of ten and so was our patient and this may be related to the infectious agent causing pneumonia [2-5].
As in other forms of postinfectious glomerulonephritis in pneumonia-associated glomerulonephritis, the inflammatory process that takes place in the glomeruli is triggered by antigen-antibody reactivity that results in local activity of complement system and of the coagulation cascade [1].
Hypocomplementemia occurs as a result of activation of alternative complement pathway and it was also a common finding in the series we had reviewed [2,3,5]. Hypocomplementemia was also observed in our patient and returned to normal after 12 weeks at follow up.
Various infectious agents may cause pneumonia associated with glomerulonephritis, mycoplasma pneumonia is the most common microorganism seen in adult series [9]. Streptococcus pneumonia and Chlamydia pneumonia infections may also be associated with glomerulonephritis [2,6-8]. We could not detect the causing microorganism in our patient; blood, pharyngeal swab and urine cultures were all negative. Because the etiology could not be identified and glomerulonephritis occurred synchronously with pneumonia IgA nephropathy was also considered as a differential diagnosis. Our patient had low serum complement 3 levels, marked hypertension and showed a quick resolution of renal impairment. She did not have chronic persistent or recurrent hematuria during follow up. Taken together these findings favored the diagnosis of postinfectious glomerulonephritis rather than IgA nephropathy.
Antistreptolysin O (ASLO) titers were elevated in our patient as reported in other series in the literature. Srivastava reported elevated ASLO titers in 10 of 11 patients in his study [3]. All of the 3 patients and 5 of the 6 patients in the studies of Lechon [2] and Vila Cots [5] had also elevated ASLO titers respectively. But none of these authors attributed glomerulonephritis to Streptococcus pyogenes infection because ASLO titers may be affected from many other factors and no universally normal value was applicable. In our patient; pharyngeal swab culture was negative, there was typical clinical, laboratory and radiological findings of pneumonia; therefore our patient was diagnosed as pneumonia associated glomerulonephritis. Because the clinical picture of the patient was mild and anti-neutrophil cytoplasmic antibody was negative we did not consider an immune mediated process which affected lung and kidney simultaneously as seen in Good-Pasture syndrome. Yet this was the first attack of hematuria synchronous with a respiratory tract infection and serum complement 3 level was low IgA was not thought at the forefront.
Diagnosis depends on urine analysis (red blood cells and red blood cell casts, white blood cells, rarely proteinuria), evidence of previous infection (Streptococcal test, pharyngeal swab for viral PCR, etc), renal function tests and serum complement levels. If the patient is presented with a well-defined clinical picture renal biopsy is seldom required [1]. We did not perform renal biopsy because of rapid improvement of renal and respiratory findings with antibiotic and diuretic treatment. Only one child in the study of Srivastava went under renal biopsy which showed proliferative glomerulonephritis without crescents [3].
Renal prognosis is generally benign and the prognosis is favorable in pneumonia associated APIGN. Antibiotic treatment is required when infection is present at the time of diagnosis [1]. Treatment is usually supportive and directed towards potential complications as hypertension and severe fluid and electrolyte disturbances. Dialysis is rarely required in children for treatment of uremia, hyperkalemia or severe circulatory congestion [1]. Only one child in the study of Srivastava [3] required dialysis for four days but at follow up blood pressure, urine analysis, serum complements were normalized in 9 patients in whom follow up was available. Renal involvement was also mild in the series of Lechon and Vila Cots respectively [2,5]. In our patient oliguria lasted for only one day and she responded well to diuretics and antibiotics. At follow up renal function tests and urine analysis were completely normal.
As reported in previous series and case reports there is an association between pneumonia and glomerulonephritis although it is very rare. In typical clinical picture basic laboratory investigations may be sufficient; renal biopsy is recommended when normocomplementemia or persistent hypocomplementemia exists or when renal function declines rapidly [1]. In most patients the respiratory and renal prognosis is favorable but clinicians must be aware of the course to make prompt diagnosis and appropriate management and to avoid unnecessary medical intervention.
Although all of the patients were male in the study of Srivastava [3], this may be an incidental finding because there are female patients in the other studies and the number of the patients in all series are small to interpretar about this issue. Patients are generally under the age of ten and so was our patient and this may be related to the infectious agent causing pneumonia [2-5].
As in other forms of postinfectious glomerulonephritis in pneumonia-associated glomerulonephritis, the inflammatory process that takes place in the glomeruli is triggered by antigen-antibody reactivity that results in local activity of complement system and of the coagulation cascade [1].
Hypocomplementemia occurs as a result of activation of alternative complement pathway and it was also a common finding in the series we had reviewed [2,3,5]. Hypocomplementemia was also observed in our patient and returned to normal after 12 weeks at follow up.
Various infectious agents may cause pneumonia associated with glomerulonephritis, mycoplasma pneumonia is the most common microorganism seen in adult series [9]. Streptococcus pneumonia and Chlamydia pneumonia infections may also be associated with glomerulonephritis [2,6-8]. We could not detect the causing microorganism in our patient; blood, pharyngeal swab and urine cultures were all negative. Because the etiology could not be identified and glomerulonephritis occurred synchronously with pneumonia IgA nephropathy was also considered as a differential diagnosis. Our patient had low serum complement 3 levels, marked hypertension and showed a quick resolution of renal impairment. She did not have chronic persistent or recurrent hematuria during follow up. Taken together these findings favored the diagnosis of postinfectious glomerulonephritis rather than IgA nephropathy.
Antistreptolysin O (ASLO) titers were elevated in our patient as reported in other series in the literature. Srivastava reported elevated ASLO titers in 10 of 11 patients in his study [3]. All of the 3 patients and 5 of the 6 patients in the studies of Lechon [2] and Vila Cots [5] had also elevated ASLO titers respectively. But none of these authors attributed glomerulonephritis to Streptococcus pyogenes infection because ASLO titers may be affected from many other factors and no universally normal value was applicable. In our patient; pharyngeal swab culture was negative, there was typical clinical, laboratory and radiological findings of pneumonia; therefore our patient was diagnosed as pneumonia associated glomerulonephritis. Because the clinical picture of the patient was mild and anti-neutrophil cytoplasmic antibody was negative we did not consider an immune mediated process which affected lung and kidney simultaneously as seen in Good-Pasture syndrome. Yet this was the first attack of hematuria synchronous with a respiratory tract infection and serum complement 3 level was low IgA was not thought at the forefront.
Diagnosis depends on urine analysis (red blood cells and red blood cell casts, white blood cells, rarely proteinuria), evidence of previous infection (Streptococcal test, pharyngeal swab for viral PCR, etc), renal function tests and serum complement levels. If the patient is presented with a well-defined clinical picture renal biopsy is seldom required [1]. We did not perform renal biopsy because of rapid improvement of renal and respiratory findings with antibiotic and diuretic treatment. Only one child in the study of Srivastava went under renal biopsy which showed proliferative glomerulonephritis without crescents [3].
Renal prognosis is generally benign and the prognosis is favorable in pneumonia associated APIGN. Antibiotic treatment is required when infection is present at the time of diagnosis [1]. Treatment is usually supportive and directed towards potential complications as hypertension and severe fluid and electrolyte disturbances. Dialysis is rarely required in children for treatment of uremia, hyperkalemia or severe circulatory congestion [1]. Only one child in the study of Srivastava [3] required dialysis for four days but at follow up blood pressure, urine analysis, serum complements were normalized in 9 patients in whom follow up was available. Renal involvement was also mild in the series of Lechon and Vila Cots respectively [2,5]. In our patient oliguria lasted for only one day and she responded well to diuretics and antibiotics. At follow up renal function tests and urine analysis were completely normal.
As reported in previous series and case reports there is an association between pneumonia and glomerulonephritis although it is very rare. In typical clinical picture basic laboratory investigations may be sufficient; renal biopsy is recommended when normocomplementemia or persistent hypocomplementemia exists or when renal function declines rapidly [1]. In most patients the respiratory and renal prognosis is favorable but clinicians must be aware of the course to make prompt diagnosis and appropriate management and to avoid unnecessary medical intervention.
REFERENCES
- Rotriguez–IturbeB, Sergio M (2009) Acute postinfectious glomerulonephritis. In: Avner ED, Harmon EW, Niaudet P, Yoshikawa N (eds.). Pediatric Nephrology, (6th edn), Berlin Heidelberg, Springer, Place, Country. Pg: 743-755.
- Lechon FC, de la Torre Espi M, Abal RP, Peiro JEP (2010) Acute glomerulonephritis associated with pneumonia: a review of three cases. PediatrNephrol 25: 161-164.
- Srivastava T, Warady, Alon US (2002) Pneumonia-associated acute glomerulonephritis. Clin Nephrol 57: 175-182.
- Schachter J, Pomeranz A, Berger I, Wolach B (1987) Acute glomerulonephritis secondary to lobar pneumonia. Int J Pediatr Nephrol 8: 211-214.
- Vila Cots J, Piqueras Marimbaldo I, Arias Constanti V, Camacho Díaz JA, Gimenez Llort A, et al. (2011) [Pneumonia associated acute glomerulonephritis: a review of 6 cases]. An Pediatr (Barc) 74: 332-335.
- Phillips J, Palmer A, Baliga R (2005) Glomerulonephritis associated with acute pneumococcal pneumonia: a case report. Pediatr Nephrol 20: 1494-1495.
- Morin D, Ichay I, Dumas ML et al. (1999) Membranoproliferative glomerulonephritis in a 10-year-old boy with pneumococcal pneumonia. Pediatr Nephrol 13: 58.
- Tanaka H, Onodera N, Ito R, Hirano K, Monma N, et al. (1999) Acute glomerulonephritis associated with pneumonia: a possible Chlamydia pneumoniae etiology? Pediatr Int 41: 698-700.
- van Westrhenen R, Weening JJ, Krediet RT (1998) Pneumonia and glomerulonephritis caused by Mycoplasma pneumoniae. Nephrol Dial Transplant 13: 3208-3211.
Citation: Özlü SG, Yilmaz AÇ, Bülbül M, Aydo? Ö, ?enel S (2016) Lobar Pneumonia and Glomerulonephritis: An Unusual Association. J Nephrol Renal Ther 2: 009
Copyright: © 2016 Sare Gülfem Özlü, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Journal Highlights
© 2026, Copyrights Herald Scholarly Open Access. All Rights Reserved!