Survey of Trauma Physicians Awareness of Rehabilitation Services in King Saud Medical City
*Corresponding Author(s):
Wafaa HakamiPhysical Therapist, King Saud Medical City, Riyadh, Saudi Arabia
Tel:+966533636262,
Email:w-hakami@ksmc.med.sa
Abstract
Introduction
Traumatic injuries are one of the most prominent causes of morbidity, disability, and mortality in Saudi Arabia. It is the leading cause of hospital admission, and it also has an impact on hospitals and their services as well.One of the healthcare teams involved in the care of the trauma patient is the rehabilitation team. In King Saud Medical City, this team consists of the following departments: Physicalmedicine and rehabilitation, physical therapy, occupational therapy, speech and swallowing, orthotics and prosthetics, and social services. They work along each other as a multidisciplinary team to treat patients with a holistic approach on a referral system from physicians from different specialties within the hospital.
Aim and significance
The aim of this study is to assess King Saud Medical City physicians' awareness levels regarding the rehabilitation services with a comparison of trauma physicians' awareness levels compared to other specialty physicians. Currently, there are no studies establishing this aim.
Methods
The study design is a cross-sectional study using a structured questionnaire in King Saud Medical City. The subjects are physicians currently working in King Saud Medical City from different specialties with a focus on trauma physicians.
Results
35 physicians participated in this study, 83% (n=29) were males and 17% (n=6) females. Ages ranged in 25-62 years-range with a mean age (±SD) of 40.43±10.6 years. 28.6% (n =10) of the participating physicians were trauma physicians and 71.4% (n=25) physicians were from orthopedics, emergency, general surgery, and other groups working in King Saud Medical City. 37.1% (n=13) of the physicians were consultants, 17.1% (n=5) were associate consultants, 20% (n=7) were assistant consultants and 25.7% (n=9) were residents.
All participants were aware of physical medicine and rehabilitation (100%, N=35), 91.4% (N=32) were also aware of Physical Therapy, and 88.6% (N=31) were aware of occupational therapy. As for orthotics and prosthetics, 82.9% (N=29) have heard of them as well as speech and swallowing pathologists. 77.1% (N=27) physicians knew that social workers are involved with the rehabilitation team. Opinions also were taken if a rehabilitation center was needed and 94.3% answered with "yes". They had the same opinion when asked if the rehabilitation center will contribute to a better outcome.
Using the non-parametric Kruskal-Wallis test (One Way ANOVA), there is no difference between the awareness of trauma physicians and other specialties physicians.
Discussion and conclusion
This is the first study of this aim regarding any specialty group of physicians' awareness of rehabilitation in King Saud Medical City.
The outcome of this study acknowledged high awareness levels of the rehabilitation team and its services among trauma physicians in King Saud Medical City, with small variation between awareness of the different services. The highest awareness levels were of physical medicine and rehabilitation, physical therapy, and occupational therapy. The awareness levels of orthotics andprosthetics, speech and swallowing, and social workers were moderate which encourages educational activities to raise awareness.
These encouraging results with favorably high levels of awareness in most aspects have proved that the awareness of rehabilitation in all the participating physicians is praiseworthy, but still has room for development and advancement of the rehabilitation services either in their current state or in the future as a dedicated center within King Saud Medical City.
Keywords
Awareness; King Saud Medical City; Rehabilitation; Saudi Arabia; Trauma
INTRODUCTION
Traumatic injuries are one of the most prominent causes of morbidity, disability, and mortality in this era of development in Saudi Arabia. They pose a serious threat to health and are a psycho-socio-economic burden on the injured patients and their families and societies with an undeniable influence on their lifestyle. It is the leading cause of hospital admission globally and it has an impact on hospitals and their services as well [1,2]. Due to the burden of trauma and the rising necessity for its management and care development, a cooperation agreement between King Saud Medical City and Alfred Hospital of Australia resulted in launching a trauma registry in King Saud Medical City and a services program titled 'King Saud Medical City-The Alfred International Trauma Program - Trauma Service Development" commencing in 2015 with expected completion at 2019[3,4].
King Saud Medical City (KSMC) is a tertiary ministry of health hospital serving the population of Riyadh since 1956 with a trauma unit since 2015 [3,4]. One of the healthcare teams involved in the care of the trauma patient, and patients in general, is the rehabilitation team.
Rehabilitation, as defined by World Health Organization (WHO), is “a set of measures that assist individuals who experience, or are likely to experience, disability to achieve and maintain optimal functioning in interaction with their environments” [5]. It is aimed to either prevent or slow down the loss of function. It is also aimed to improve, restore, or compensate for lost function. Ultimately it can maintain a level of function which all depends on the patient’s status as defined by WHO Rehabilitation guidelines [6]. The rehabilitation team in King Saud Medical City consists of the following departments: physical medicine and rehabilitation, physical therapy, occupational therapy, speech and swallowing, orthotics and prosthetics, and social services. They work along each other as a multidisciplinary team to treat patients with a holistic approach on a referral system from physicians from different specialties within the hospital.
While the rehabilitation team approach is comprehensive, its involvement with trauma patients is controlled by physicians' referral to rehabilitation which is limited compared to other specialties. This to some extent also confines the patient’s outcome in the long run which asks a question of the cause of this difference and the possibility of contrasting levels of awareness between the specialties. In a study done by Al Jadid et al., (2017)[7] in Prince Sultan Military Medical City (PSMMC), the awareness of physicians of physical medicine and rehabilitation was satisfactory with a moderate level of awareness. In that study (Al Jadid et al., 2017), “92.5% physicians reported being aware and/or heard about PM&R, while 20% responded that PM&R was identical to physical therapy” [7]. The study was done by Al Jadid (2017)[7] focused only on physicians' awareness of PMR in PSMMC, it was a first on its kind and has influenced the authors of this study to research the awareness of physicians on the rehabilitation team in King Saud Medical City, with an emphasis on trauma physicians.
Awareness is as defined by Cambridge dictionary is "knowledge that something exists, or understanding of a situation or subject at the present time based on information or experience" which is what the study precisely aimed to measure: do trauma physicians, based on their current knowledge and experiences, know of the rehabilitation services in King Saud Medical City or not.
AIMS OF THE STUDY
- Assess physicians’ awareness levels regarding the rehabilitation services in King Saud Medical City (KSMC), Riyadh, Saudi Arabia
- Compare the awareness of trauma physicians to that of other specialty physicians also working in KSMC
SIGNIFICANCE
There are no studies establishing awareness levels of trauma physicians or physicians in general at King Saud Medical City of rehabilitation services provided in King Saud Medical City. From this study, we can identify their awareness levels, and act accordingly to increase awareness if required.
METHODOLOGY
Setting: King Saud Medical City (KSMC), Riyadh, Saudi Arabia.
Subjects: trauma and other specialty physicians in KSMC.
Design: a cross-sectional study.
Variables:
Personal details of physicians, including;
- Age
- Gender
- Specialty
- Ranking according to the Saudi Commission for health specialties
- Length\period of employment at KSMC
- Source of their awareness
- Referral to rehabilitation and follow up
- Patient improvement
- Awareness and knowledge about differences between rehabilitation services
- Need for a rehabilitation center to be established in KSMC
Inclusion criteria:
- Physicians working full-time in KSMC at the time of their participation
- Physicians who have their SCFHS
- Physicians in the trauma department
Exclusion criteria:
- Physicians who are not full-time employees at KSMC
- Medical interns and students
- Other allied health specialties than physicians
DATA COLLECTION AND EXTRACTION
A structured questionnaire was used for data collection. It was sent by email and completed online by all physicians who were contacted and agreed to participate with one of our researchers. The questionnaire had a personal data section, and separate sections for each rehabilitation specialty (physical medicine and rehabilitation, physical therapy, occupational therapy, orthotics and prosthetics, speech and swallowing, and social worker). Each section had 4 yes/no questions regarding communication, and 5-6 questions measured the awareness level as well as a true multiple-choice question at the end of each section with one correct answer with the purpose of affirming awareness. For each section, the first question was a defining question with if answered with "no", the remaining questions of the section were assumed to be "no" and no awareness was expected. The participants were expected to answer the questions with attention to the relations of each question to its section. The participants were requested to answer questions privately with no intervention or assistance from colleagues or the use of the internet.
ANALYSIS
The data collected and analyzed was age (discrete numerical data), gender, specialty, and SCFHS ranking, and period of employment (categorical data), and a scale of awareness varying from no awareness to high awareness (ordinal nominal data).Data were analyzed using Microsoft Excel 2016 (Microsoft Corporation, Seattle, WA, USA) and the statistical package for social sciences (SPSS Inc., Chicago, IL, USA). The method of statistical analysis is the central tendency (mean) and frequency. Besides the descriptive analysis, the differences between trauma and the other specialties physicians were measured using a non-parametric Kruskal-Wallis test (One Way ANOVA).
RESULTS
There was a total of 35 participants who completed the questionnaire. At the time of the survey, the hospital had 17 trauma physicians, and 10 of them answered the questionnaire completely. The hospital's research center determined that it was acceptable to proceed to data processing when the sample size reached 35 participants. Of the participants, 83% (n=29) were males and 17% (n=6) females. Their ages had a range of 25-62 years with a mean age (±SD) of 40.43±10.6 years.28.6% (n=10) of the participating physicians were trauma physicians and 71.4% (n=25) physicians were from orthopedics, emergency, general surgery, and other groups working in King Saud Medical City. 37.1% (n=13) of the physicians were consultants, 17.1% (n=5) were associate consultants, 20% (n=7) were assistant consultants and 25.7% (n=9) were residents.
This demographic data is presented in table 1 and through figures 1 to 5.As for the responses of the questionnaires, they are represented in tables from A to F in two tables for each section except section G which is represented in one table.
|
Age |
Frequency (N) and Percentage (%) |
|
Less than 30 years |
7 (20%) |
|
From 30 to less than 40 years |
9 (26%) |
|
From 40 to less than 50 years |
11 (31%) |
|
From 50 years and more |
8 (23%) |
|
Gender |
Frequency (N) and Percentage (%) |
|
Male |
29 (83%) |
|
Female |
6 (17%) |
|
SCFHS Ranking |
Frequency (N) and Percentage (%) |
|
Resident |
7 (20%) |
|
Assistant consultant |
6 (17.1%) |
|
Associate consultant |
13 (37.1%) |
|
Consultant |
9 (25.7%) |
|
Specialty |
Frequency (N) and Percentage (%) |
|
Trauma |
10 (28.6%) |
|
ER |
4 (11.4%) |
|
General surgery |
3 (8.6%) |
|
Internal medicine |
3 (8.6%) |
|
Neurology |
1 (2.9%) |
|
Neurosurgery |
2 (5.7%) |
|
Orthopedic |
7 (20%) |
|
Plastic surgery |
2 (5.7%) |
|
Radiology |
1 (2.9%) |
|
Other (GP) |
1 (2.9%) |
|
Other (Rheumatology) |
1 (2.9%) |
|
Duration of employment at KSMC |
Frequency (N) and Percentage (%) |
|
Less than 1 year |
1 (2.9%) |
|
1 year |
7 (20%) |
|
2 years |
9 (25.7%) |
|
3 years |
5 (14.3%) |
|
4 years |
1 (2.9%) |
|
5 years or more |
12 (34.3%) |
Table 1: Demographic characteristics.
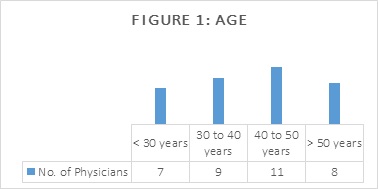 Figure 1: Column chart of age distribution by frequency. Mean = 40.43, SD = 10.6.
Figure 1: Column chart of age distribution by frequency. Mean = 40.43, SD = 10.6.
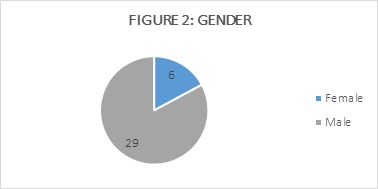 Figure 2: Pie chart of gender distribution by frequency.
Figure 2: Pie chart of gender distribution by frequency.
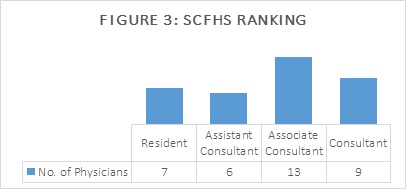 Figure 3: Column chart of Saudi Health Commission for Health Specialties distribution by frequency.
Figure 3: Column chart of Saudi Health Commission for Health Specialties distribution by frequency.
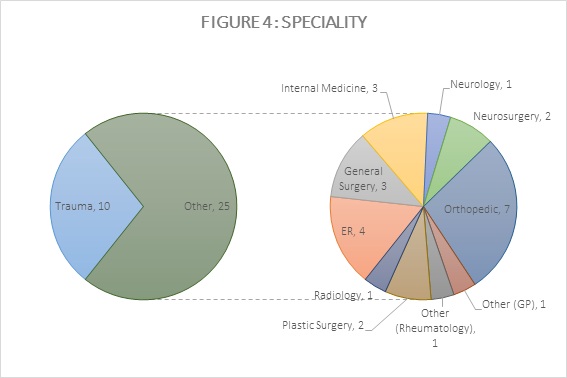 Figure 4: Pie chart of physician’s specialties by frequency.
Figure 4: Pie chart of physician’s specialties by frequency.
 Figure 5: Column chart of employment duration by frequency.
Figure 5: Column chart of employment duration by frequency.
|
Questions |
Frequency (N) and Percentage (%) |
|
Have you heard of the physical medicine and rehabilitation (PMR) specialty? |
|
|
No |
0 (0%) |
|
Yes |
35 (100%) |
|
Have you ever referred a patient to physical medicine and rehabilitation? |
|
|
No |
5 (14.3%) |
|
Yes |
29 (82.9%) |
|
Not applicable |
1 (2.9%) |
|
If yes, did you follow up with the patients afterward? |
|
|
No |
10 (28.6%) |
|
Yes |
21 (60%) |
|
Not applicable |
4 (11.4%) |
|
Did your patient improve after the referral to PMR? |
|
|
No |
2 (5.7%) |
|
Yes |
25 (71.4%) |
|
Not applicable |
6 (17.1%) |
|
No follow up |
2 (5.7%) |
|
How did you know of PMR and rehabilitation services in KSMC? |
|
|
KSMC portal |
3 (8.6%) |
|
Work colleagues |
18 (51.4%) |
|
Direct contact with a rehabilitation specialist |
14 (40%) |
Table (A-1): Physical Medicine and Rehabilitation.
|
Statements |
Awareness (N & %) |
|||
|
Never aware |
Slightly aware |
Moderately aware |
Strongly aware |
|
|
To what extent are you aware that your collaboration with PMR will benefit the patient? |
0 (0%) |
5 (14.3%) |
14 (40%) |
16 (45.7%) |
|
Are you aware that Physical medicine and rehabilitation is not the same as physical therapy? |
3 (8.6%) |
5 (14.3%) |
7 (20%) |
20 (57.1%) |
|
Are you aware of the need for specialized rehabilitation physicians? |
1 (2.9%) |
2 (5.7%) |
9 (25.7%) |
23 (65.7%) |
|
How much are you aware that Prescription of exercises and modalities are within the scope of PMR practice? |
5 (14.3%) |
4 (11.4%) |
13 (37.1%) |
13 (37.1%) |
|
How much are you aware that musculoskeletal disorders and neurological disorders diagnosis and treatment are within PMR scope? |
1 (2.9%) |
9 (25.7%) |
13 (37.1%) |
12 (34.3%) |
|
Are you aware that physical medicine and rehabilitation are able to refer patients to other rehabilitation departments such as physical therapy, occupational therapy, orthotics and prosthetics, speech and swallowing, and social workers? |
5 (14.3%) |
5 (14.3%) |
12 (34.3%) |
13 (37.1%) |
Table (A-2): Physical Medicine and Rehabilitation.
|
Questions |
Frequency (N) and Percentage (%) |
|
Have you heard of the physical therapy? |
|
|
No |
3 (8.6%) |
|
Yes |
32 (91.4%) |
|
Have you ever referred a patient to physical therapy? |
|
|
No |
6 (17.1%) |
|
Yes |
28 (80%) |
|
Not applicable |
1 (2.9%) |
|
If yes, did you follow up with the patients afterward? |
|
|
No |
8 (22.9%) |
|
Yes |
25 (71.4%) |
|
Not applicable |
2 (5.7%) |
|
Did your patient improve after the referral to PT? |
|
|
No |
6 (17.1%) |
|
Yes |
22 (62.9%) |
|
Not applicable |
1 (2.9%) |
|
No follow up |
6 (17.1%) |
|
Physical therapy scope of practice includes all except: |
|
|
Pain management. |
2 (5.7%) |
|
Medications prescription. (Correct Answer) |
30 (85.7%) |
|
Use of therapeutic techniques and modalities. |
3 (8.6%) |
Table (B-1): Physical Therapy.
|
Statements |
Awareness (N & %) |
|||
|
Never aware |
Slightly aware |
Moderately aware |
Strongly aware |
|
|
How much are you aware that physical therapy is more than prescribed exercise? |
7 (20%) |
8 (22.9%) |
9 (25.7%) |
11 (31.4%) |
|
Are you aware that physical therapy is necessary to patients’ functional independence? |
4 (11.4%) |
5 (14.3%) |
9 (25.7%) |
17 (48.6%) |
|
Are you aware that physical therapy has a role in pain management? |
11 (31.4%) |
6 (17.1%) |
12 (34.3%) |
6 (17.1%) |
|
How much are you aware that physical therapy has a role in all conditions affecting mobility and movement? |
3 (8.6%) |
4 (11.4%) |
11 (31.4%) |
17 (48.6%) |
|
To what extent are you aware that physical therapists use a therapeutic form of ultrasound modality? |
16 (45.7%) |
6 (17.1%) |
6 (17.1%) |
7 (20%) |
Table (B-2): Physical Therapy.
|
Questions |
Frequency (N) and Percentage (%) |
|
Have you heard of occupational therapy? |
|
|
No |
4 (11.4%) |
|
Yes |
31 (88.6%) |
|
Have you ever referred a patient to occupational therapy? |
|
|
No |
19 (54.3%) |
|
Yes |
14 (40%) |
|
Not applicable |
2 (5.7%) |
|
If yes, did you follow up with the patients afterward? |
|
|
No |
12 (34.3%) |
|
Yes |
13 (37.1%) |
|
Not applicable |
10 (28.6%) |
|
Did your patient improve after the referral to OT? |
|
|
No |
11 (31.4%) |
|
Yes |
8 (22.9%) |
|
Not applicable |
11 (31.4%) |
|
No follow up |
5 (14.3%) |
|
Occupational therapy main outcome focuses on ... with varying interventions to achieve it: |
|
|
Patient safety. |
3 (8.6%) |
|
Patient dependence. |
12 (34.3%) |
|
Activities of daily living (ADL) (Correct Answer) |
20 (57.1%) |
Table (C-1): Occupational Therapy.
|
Statements |
Awareness (N & %) |
|||
|
Never aware |
Slightly aware |
Moderately aware |
Strongly aware |
|
|
Are you aware that occupational therapy is different from physical therapy? |
6 (17.1%) |
11 (31.4%) |
4 (11.4%) |
14 (40%) |
|
Are you aware that occupational therapy is necessary to patients’ functional independence? |
6 (17.1%) |
8 (22.9%) |
11 (31.4%) |
10 (28.6%) |
|
Are you aware that occupational therapy has a role in patients’ return to normal daily activities? |
6 (17.1%) |
4 (11.4%) |
13 (37.1%) |
12 (34.3%) |
|
Are you aware that occupational therapy is essential to patient’s return to work? |
6 (17.1%) |
5 (14.3%) |
13 (37.1%) |
11 (31.4%) |
|
Are you aware that occupational therapists are able to use and modify orthotics/external splints? |
14 (40%) |
3 (8.6%) |
7 (20%) |
11 (31.4%) |
Table (C-2): Occupational Therapy.
|
Questions |
Frequency (N) and Percentage (%) |
|
Have you heard of orthotics and prosthetics department? |
|
|
No |
6 (17.1%) |
|
Yes |
29 (82.9%) |
|
Have you ever referred a patient to orthotics and prosthetics department? |
|
|
No |
12 (34.3%) |
|
Yes |
22 (62.9%) |
|
Not applicable |
1 (2.9%) |
|
If yes, did you follow up with the patients afterward? |
|
|
No |
11 (31.4%) |
|
Yes |
19 (54.3%) |
|
Not applicable |
5 (14.3%) |
|
Did your patient improve after the referral to orthotics and prosthetics department? |
|
|
No |
6 (17.1%) |
|
Yes |
19 (54.3%) |
|
Not applicable |
5 (14.3%) |
|
No follow up |
5 (14.3%) |
|
Orthotics and prosthetics department make/prescribe: |
|
|
Upper extremity splints |
1 (2.9%) |
|
Spinal braces |
1 (2.9%) |
|
Lower extremity prosthetics |
2 (5.7%) |
|
All of the above is correct (Correct Answer) |
31 (88.6%) |
Table (D-1): Orthotics and Prosthetics.
|
Statements |
Awareness (N & %) |
|||
|
Never aware |
Slightly aware |
Moderately aware |
Strongly aware |
|
|
Are you aware that orthotics and prosthetics department prescribes prefabricated equipment? |
7 (20%) |
4 (11.4%) |
13 (37.1%) |
11 (31.4%) |
|
To what extent are you aware that orthotics and prosthetics department is able to make custom orthotics? |
7 (20%) |
4 (11.4%) |
12 (34.3%) |
12 (34.3%) |
|
How much are you aware that orthotics and prosthetics department is able to make adjustments to orthotics/prosthetics? |
7 (20%) |
4 (11.4%) |
12 (34.3%) |
12 (34.3%) |
|
Are you aware that an orthotic is external braces designed to fulfill a specific need in a patients’ treatment? |
6 (17.1%) |
3 (8.6%) |
12 (34.3%) |
14 (40%) |
|
Are you aware that a prosthetic is artificial limbs designed to substitute a patient with limb loss? |
8 (22.9%) |
2 (5.7%) |
7 (20%) |
18 (51.4%) |
Table (D-2): Orthotics and Prosthetics.
|
Questions |
Frequency (N) and Percentage (%) |
|
Have you heard of speech and swallowing department? |
|
|
No |
6 (17.1%) |
|
Yes |
29 (82.9%) |
|
Have you ever referred a patient to speech and swallowing department? |
|
|
No |
14 (40%) |
|
Yes |
21 (60%) |
|
Not applicable |
0 (0%) |
|
If yes, did you follow up with the patients afterward? |
|
|
No |
7 (20%) |
|
Yes |
22 (62.9%) |
|
Not applicable |
6 (17.1%) |
|
Did your patient improve after the referral to speech and swallowing department? |
|
|
No |
8 (22.9%) |
|
Yes |
18 (51.4%) |
|
Not applicable |
7 (20%) |
|
No follow up |
2 (5.7%) |
|
Speech and swallowing pathologists work with the following disorders except: |
|
|
Dysphagia |
5 (14.3%) |
|
Dysarthria |
3 (8.6%) |
|
Agraphia (Correct Answer) |
21 (60%) |
|
Aphasia |
6 (17.1%) |
Table (E-1): Speech and Swallowing.
|
Statements |
Awareness (N & %) |
|||
|
Never aware |
Slightly aware |
Moderately aware |
Strongly aware |
|
|
Are you aware that speech and swallowing department has a role in rehabilitation? |
7 (20%) |
5 (14.3%) |
12 (34.3%) |
11 (31.4%) |
|
How much are you aware that speech pathologists are able to diagnose and treat speech and language disorders? |
6 (17.1%) |
10 (28.6%) |
8 (22.9%) |
11 (31.4%) |
|
Are you aware that swallowing pathologists are able to diagnose and treat swallowing and feeding disorders? |
7 (20%) |
5 (14.3%) |
8 (22.9%) |
15 (42.9%) |
|
To what extent are you aware that speech and swallowing pathologists use diagnostic radiology modalities? |
10 (28.6%) |
10 (28.6%) |
4 (11.4%) |
11 (31.4%) |
|
Are you aware that speech and swallowing pathologists are able to modify a patient’s diet to suit their swallowing status? |
7 (20%) |
8 (22.9%) |
9 (25.7%) |
11 (31.4%) |
Table (E-2): Speech and Swallowing.
|
Questions |
Frequency (N) and Percentage (%) |
|
Are social workers a part of the rehabilitation team? |
|
|
No |
8 (22.9%) |
|
Yes |
27 (77.1%) |
Table (F-1): Social Worker.
|
Statements |
Awareness (N & %) |
|||
|
Never aware |
Slightly aware |
Moderately aware |
Strongly aware |
|
|
Are you aware that social workers assist in patient’s acceptance and family management of health condition? |
8 (22.9%) |
6 (17.1%) |
9 (25.7%) |
12 (34.4%) |
Table (F-2): Social Worker.
|
Questions |
Frequency (N) and Percentage (%) |
|
Do you think that KSMC needs a rehabilitation center? |
|
|
No |
2 (5.7%) |
|
Yes |
33 (94.3%) |
|
Do you believe that having a rehabilitation center contributes to better patient rehabilitation outcome? |
|
|
No |
2 (5.7%) |
|
Yes |
33 (94.3%) |
Table G:Rehabilitation center.
Trauma versus other specialties awareness levels comparison:With the null hypothesis being that there is no difference between the awareness due to the between trauma and other specialty groups, and the alternative hypothesis suggests that there is a difference between the awareness due to the between trauma and other specialty groups.
The following table H shows the results of the non-parametric Kruskal-Wallis test (One Way ANOVA):
|
No. |
Awareness |
P-value |
Result |
|
A |
Physical Medicine and Rehabilitation |
0.321 |
Don’t reject the null hypothesis |
|
B |
Physical Therapy |
0.97 |
|
|
C |
Occupational Therapy |
0.679 |
|
|
D |
Orthotics and Prosthetics |
0.653 |
|
|
E |
Speech and Swallowing |
0.113 |
|
|
F |
Social Worker |
0.733 |
Table H: Hypothesis.
Note:Every p-value in the previous table is greater than 0.05 which indicates that there is no difference between the awareness of trauma physicians and other specialties physicians.
DISCUSSION
To this time, this is the first study measuring the awareness of King Saud Medical City physicians of the rehabilitation team through a structured questionnaire to collect their responses. It is also the first to compare trauma physicians' awareness to the physicians from other teams and evaluate communication between all of the teams. There were also no prior studies of this aim regarding any specialty group of physicians in King Saud Medical City.
In Khan's systematic review of multidisciplinary rehabilitation for trauma patients in 2011 [8], he deducted that "although significant improvements in the coordination and organization of trauma care and services have reduced patient mortality, this has not extended to include rehabilitation services." In that study (Khan, 2011), it was suggested that rehabilitation requirements and resources should be tailored to governmental and private health sectors to prioritize rehabilitation of trauma survivors [8].
Taking the first question of each section as an indicator, all participants were aware of Physical Medicine and Rehabilitation (100%, N=35) (table A-1), 91.4% (N=32) were also aware of Physical Therapy (table B-1), and 88.6% (N=31) were aware of Occupational Therapy (table C-1). As for Orthotics and Prosthetics (table D-1), 82.9% (N=29) have heard of them as well as Speech and Swallowing pathologists (table E-1). 77.1% (N=27) physicians knew that social workers are involved with the rehabilitation team (table F). These results are represented in figure 6.
Figure 6: Pie chart of the answer to "Do you think that KSMC needs a rehabilitation center?"
For the last section, opinions were taken if a rehabilitation center was needed and 94.3% answered with "yes". They had the same opinion when asked if the rehabilitation center will contribute to a better outcome (table G).
This study showed that a majority of physicians were "moderately to highly aware" of most of the statements in the questionnaire which measured awareness of physicians with the rehabilitation team, although the difference in awareness between trauma physicians and other specialties was not significant. All physicians participating in this study have heard of physical medicine and rehabilitationphysicians and reported that they knew of them by their work colleagues (N=18 51.4%). This finding is similar to that of Al Jadid (2017)[7], where the awareness of physicians of physical medicine and rehabilitation was satisfactory with a moderate level of awareness. This finding was also evident in relation to the physical therapy, occupational therapy, speech and swallowing disorders, and the prosthetics and orthotics department. A high level of awareness was found of all of them. These high awareness levels can be attributed to the medical city environment and communication in-between the medical staff. It can be also attributed to the interaction language between all of the multidisciplinary team which is English both verbal and written communication such as the patient files which include documentation of all treating professionals.
Physical medicine and rehabilitation
Physical Medicine and Rehabilitation (PMR) are a medical specialty involved with rehabilitation. A PMR specialist is an expert in dealing with the rehabilitative process from providing a diagnosis to delivering treatment with rehabilitation as a core to this approach. Physical medicine and rehabilitation physicians in King Saud Medical City have an out-patients clinic and are a part of inpatient round team along with other physicians' teams which attributed to them being the highest awareness level in this study. King Saud Medical City physicians knew of them mostly through their work colleagues (N=18, 51.4%) and by direct contact with them (N=14, 40%). They work on a consultation system and are usually given the task of referring the patients themselves to the rehabilitation team after a thorough physical examination which clarifies more on them being the members of the rehabilitation most known. 45.7% (N=16) physicians agreed strongly that their collaboration with PMR will benefit their patients, and 65.7% (N=23) were also highly aware that a specialized physician in rehabilitation was needed. When a patient requires more than one services, and if their conditions met a certain criterion, they are included in intensive rehabilitation and are followed up during a weekly meeting. This meeting includes all of the rehabilitation team and simplifies communication between the team members. 13 physicians (37.1%) were strongly aware that this was done by PMR. These findings are demonstrated in table A-1 and A-2.
Physical therapy
Another member of the rehabilitation team is a Physical Therapist (PT), an allied health professional purposed to restore wellness to individuals following injury, pain or disability [9]. The scope of the practice of physical therapy is broad and diverse, with many recognized specialties including musculoskeletal/orthopedics, sports, geriatrics, pediatrics, cardiopulmonary, neurology, women's health, and it has a role after trauma as well. As proven in Gohy and Ali study in 2016, "The integration of physiotherapists within any trauma medical team is a necessity. Raising the awareness of medical teams on the importance of physiotherapy and the criteria for prescribing physiotherapy is essential to ensure a good quality of care, allowing patients’ optimal functional recovery" [10]. PT department in King Saud Medical City is one of the oldest departments in the medical city, therefore as expected the results of PT were one of the highest communication levels in this study but had diverse awareness levels. According to Beaulieu, 2015, PT is one of the standard three acute rehabilitation treatment programs [11]. A majority of participants have referred their patients to PT (N=28, 80%) and followed up (N=25, 71.4%) then reported animprovement in their patients' conditions (N=22, 62.9%). A varied result was found when asked if PT was more than prescribed exercises with only 31.4% being strongly aware where PT included many interventions other than exercises such as manual therapy and electrotherapy which was another statement with unexpected results, as only 20% (N=7) were strongly aware that ultrasound could be used as a therapeutic modality by physical therapists. A statement with mixed results was if physicians knew if PT had a role in pain management which 17.1% (N=6) were strongly aware of. This can be contributed to the pain management in inpatients is usually managed pharmaceutically, although a majority of the patients referred to the outpatients' department of physical therapy report a chief complain of pain. As expected, the statements with strongest awareness levels were PT role for patients with conditions impairing mobility and movement as well as their goals being aimed for patient's functional independence, with 48.6% (N=17) physicians strongly aware of these statements. 20 physicians out of 35 (57.1%) were highly aware of the difference between PT and PMR, which is as well similar to the findings of Al Jadid study in PSMMC in 2017[7]. This prompts a question of which certain aspect of their practices does this misconception exists in. For the MCQ, 85.7% (n=30) knew that physical therapy did not have a role in medications prescription, which was the correct answer. These findings are demonstrated in table B-1 and B-2.
Occupational therapy
As physical therapists are mainly focused on mobility and function, closely related allied health professionals are Occupational Therapists (OT). Occupational therapists' scope of practice is similar to that of physical therapists, but with a focus and emphasis on occupation and return to normal activities of daily living [12]. Patient independence in ADL by recovery from trauma has a complex process and it is easily or ideally achieved by physical therapy alone [10]. So, both PTs and OTs work together to maximize the patients’ outcome. As PT, OT is also one of the standard three acute rehabilitation treatment programs [11]. 40% (N=14) of participants have referred their patients to OT and 37.1% (N=13) followed up with them, then 22.9% (N=8) reported an improvement in their patients' conditions. These findings do match with the physicians awareness of OT, as 28.6% (N=10) were strongly aware of the necessity of occupational therapy to the functional independence of patients, 34.3% (n=12) were also strongly aware of their role in return to daily activities and 31.4% (n=11) had a high awareness of OTs involvement in patients return to work. But these findings conflict with that only 40% (n=14) were highly aware of the difference between occupational and physical therapy. For the MCQ, 57.1% (n=20) answered the correct answer, which was OT's focus on ADL. These findings are demonstrated in table C-1 and C-2.
Orthotics and prosthetics
Orthotics and prosthetics specialties are technically two specialties working together, where an orthotics specialist fabricates external braces known as orthoses designed to fulfill a specific need in a patient’s treatment. On the other hand, a prosthetic specialist builds an artificial limb (prosthesis) to substitute a patient with limb loss. Both orthotics and prosthetics specialties take a great amount of precession and attention to details to suit each specific individual patient [13]. Of the participating physicians, 62.9% (n=22) have referred their patients to P&O, 54.3% (n=19) followed up, and the same group reported improvement in their patients'conditions. 34.3% (n=12) were strongly aware that P&O were able to make and adjust orthotics and prosthetics. The most acknowledgeable finding was the awareness of prosthetics function with a high level of awareness in 51.4% (n=18). For the MCQ, 88.6% (n=31) answered correctly and were aware that P&O can provide patients with upper extremities splints, spinal braces, lower extremities braces, and other. These findings are demonstrated in table D-1 and D-2.
Speech and swallowing
Speech and swallowing pathologists are specialists who work to prevent, assess, diagnose, and treat speech and swallowing disorders [14]. Speech disorders occur when a person is unable to produce speech or sounds correctly or fluently, or has problems with their voice or resonance [15]. Swallowing disorders are associated with the inability to swallow or feed which affects a patient’s nutrition and forms a hazard to the patient’s health [15]. Speech and swallowing pathologists or speech therapists are one of the standard three acute rehabilitation treatment programs [11]. Due to the high sensitivity of their intervention and its effect on patients' survival, 60% (n=21) have referred their patients to speech and swallowing pathologists. The same group followed up with their patients and 51.4% (n=18) reported improvement in their conditions. 11 physicians were highly aware of the S&S role in rehabilitation which is 31.4% of the participants, and they were also equally aware of their role in language disorders. A larger group up to 15 (42.9%) were strongly aware of S&S involvement in the management of feeding disorders. For the MCQ, 60% (n=21) knew that agraphia, which is a cerebral disorder characterized by the inability to write. As this disorder involves writing, it is not a part of speech and swallowing pathologists' scope of practice. These findings are demonstrated in table E-1 and E-2.
Social workers
Social workers are a key element of a patient’s rehabilitation. They assist patients and their families with a psycho-socio-economic approach discussing the impact of their current medical status and the available treatments [16].
77.1% (n=27) were aware of social workers contribution to patients' rehabilitation, but only 34.3% (n=12) were strongly aware of their exact role in patients' acceptance and management of their condition.
Need for rehabilitation center
Another important matter than awareness was also introduced in this study, which is King Saud Medical City need for a rehabilitation center. These questions received the 2nd highest agreement and awareness levels (1st was PMR) up to 94.3% (n=33) agreed to the need for a rehabilitation center and its contribution to a better rehabilitation outcome.
Trauma physicians versus others
As the aim of this study was to assess awareness of King Saud Medical City physicians of rehabilitation services as well as comparing trauma physicians to other specialty physicians, table H shows that the difference between these groups was insignificant. Therefore, no further comparison was done and the awareness of all groups was presented as one. This finding was interestingly not as predicted initially prior to the imitation of the study, and can be credited to the interdisciplinary nature of King Saud Medical City staff, their communication, ongoing collaboration, and steady teamwork.
King Saud Medical City (KSMC) is one of the numerous established hospitals with rehabilitative services such as king Fahad medical city (KFMC), King Khalid university hospital (KKUH), and King Abdulaziz university hospital (KAUH). The services provided by each one of the hospitals as in the findings of Al-Sobayel study [17] (2014) done in Riyadh and specifically King Saud Medical City, these services are admirable, but yet insufficient in comparison to the growing population and advancement in medical services. In order to manage this insufficiency, communication and coordination between the interdisciplinary teams is the key for improvement.
LIMITATIONS
Some limitations have been observed in this study, including the language used in the survey being English and no other information was taken of it being the mother language or their level of proficiency. Even though that is a limitation, it is acknowledged that English is the language used for communication and documentation in King Saud Medical City. The nature of the cross-sectional design of the study taking the awareness of a certain group at a certain group of time can be considered a limitation, which can be solved by implementing the study again periodically. Another limitation was the study's focus on one medical city and its representation of the population of all physicians in Riyadh, the kingdom's capital. An error in the questionnaire responses was found where participants answered related questioned in an incoherent matter but it was adjusted and mentioned above accordingly in the design section regarding the questionnaire and is considered a design flaw rather than a limitation.
CONCLUSION
This study showed encouraging results with favorably high levels of awareness in most aspects and proved that the awareness of rehabilitation in all the participating physicians is praiseworthy, but still has room for development and advancement of the rehabilitation services either in their current state or in the future as a dedicated center within King Saud Medical City.
It is suggested for the study to be repeated periodically to ensure a sustained level of awareness is always achieved for the ultimate benefit of the patients and ideal communication between the healthcare professionals in King Saud Medical City. A study separating the specialties and studying each individually could be beneficial for specifically targeted approaches. For a more generalized result, our hypothesis could be restudied with a larger sample size either in King Saud Medical City or including more than one medical city/center.
ACKNOWLEDGEMENT
This research was conducted under the cooperation of "King Saud Medical City, Saudi Arabia" and "The Alfred, Australia" in "Trauma Research Workshop" in last 3rd of 2018 and 1st third of 2019.
REFERENCES
- Alghnam S, Alkelya M, Al-Bedah K, Al-Enazi S (2014) Burden of traumatic injuries in Saudi Arabia: Lessons from a major trauma registry in Riyadh, Saudi Arabia. Ann Saudi Med 34: 291-296.
- Al-Naami MY, Arafah MA, Al-Ibrahim FS (2010) Trauma care systems in Saudi Arabia: An agenda for action. Ann Saudi Med 30: 50-58.
- King Saud Medical City - The Alfred International Trauma Program - Trauma Service Development, Melbourne, Australia.
- MOH Signs cooperation agreement between King Saud Medical City and Australian Alfred Hospital. Kingdom of Saudi Arabia.
- WHO Rehabilitation(2016) Geneva, Switzerland.
- https://www.who.int/disabilities/care/rehabilitation_guidelines_concept.pdf
- Al Jadid M, Alibrahim MS, Almutairi NM, Al Harbi HA, Abdelhalim R, et al. (2017) Physician awareness of physical medicine and rehabilitation: a cross-sectional study from Saudi Arabia. J Phys Med RehabilDisabil 4: 1-5.
- Khan F, Amatya B, Hoffman K (2011) Systematic review of multidisciplinary rehabilitation in patients with multiple trauma. Br J Surg 99: 88-96.
- Bellamy J, APTA - Who are physical therapists? Alexandria,Egypt.
- Gohy B, Ali E, Van den Bergh R, Schillberg E, Nasim M, et al. (2016) Early physical and functional rehabilitation of trauma patients in the Médecins Sans Frontières trauma centre in Kunduz, Afghanistan: Luxury or necessity? Int Health 8: 381-389.
- Beaulieu CL, Dijkers MP, Barrett RS, Horn SD, Giuffrida CG, et al. (2015) Occupational, physical, and speech therapy treatment activities during inpatient rehabilitation for traumatic brain injury. Arch Phys Med Rehabil 96: 222-234.
- WFOT - About Occupational Therapy, London,United Kingdom.
- AOPA - What is an orthotist/prosthetist? Australia.
- ASHA - Speech-Language Pathologists, USA.
- ASHA - Swallowing Disorders in Adults, USA.
- NASW - Clinical Social Work. Washington, D.C., USA.
- Al-Sobayel H, Aleisa E, Buragadda S, Rao MG (2014) Rehabilitation services in saudiarabia: an overview of its current structure and future challenges. J Gen Practice 2: 184.
Citation: Hakami W, Alzahrani H, AlatwiM (2019) Survey of Trauma Physicians Awareness of Rehabilitation Services in King Saud Medical City. J Phys Med Rehabil Disabil 5: 037.
Copyright: © 2019 Wafaa Hakami, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.