A Case Report of an Intestinal Malrotation in an Adult Patient and it's Treatment by a Laparoscopic Ladd Procedure
*Corresponding Author(s):
Zvi PerryCenter For Bariatric Surgery, Division Of General Surgery, Department Of Surgery, McGill University, Montreal, Quebec, Canada
Tel:+1 4384953352,
Email:zperry1@gmail.com
Abstract
Intestinal malrotation is a rare congenital anomaly, mainly seen in children. In adults, this diagnosis is quite difficult. We describe herein A 55-year-old man presented with recurrent abdominal pain. He had been seen by GI consult and had an EGD and colonoscopy which were normal. CT imaging showed a partial small bowel malrotation without malrotation of the colon. The treatment of choice in children is considered the LADD procedure, and we decided to have him undergo a laparoscopic procedure. We performed a laparoscopic Ladd procedure, completely mobilizing the right and transverse colon to expose the malrotated small bowel, encased in fibrous bands (Ladd’ bands), which were divided. After surgery the entire colon was positioned to left of midline and the small bowel to right of midline. Appendectomy was not performed; the patient was informed about the anatomic position of his appendix. He recovered well and was discharged on the first postoperative day. At his visit 4 weeks later, he was asymptomatic for the first time in years.
Keywords
Case report; Intestinal malrotation; LADD procedure
BACKGROUND
Intestinal malrotation is a congenital anomaly, and is a rare entity, seen mainly in the pediatric population. In the last few years the laparoscopic approach has been tried to treat this rare entity even in small children [1], including the LADD procedure [1]. Malrotation of the intestine is generally regarded as a pediatric pathology. It is rare in adults. Patients may present with symptoms of acute bowel obstruction or chronic abdominal pain [2]. Barium study, Contrast Computed Tomography (CT), Magnetic Resonance Imaging (MRI), diagnostic laparoscopy and sometimes even explorative laparotomy are used for diagnosis. In adults the very few case reports that were seen were many times tied to a cancerous lesion, or malrotation that was correlated with other abnormalities, like volvulus [2]. In all the cases described in adults, preoperative diagnosis was considered difficult and prone to misdiagnosis [2]. The role of laparoscopy in treatment of intestinal malrotation in the adult is still unclear, even though more case reports of laparoscopic treatment have been seen lately [1].
CASE PRESENTATION
A 55 years old gentleman had been seen in our ER 5 times due to abdominal pain. Prior medical history included BPH and depression. Prior surgical history included a lap cholecystectomy (2014). Has been suffering for 6 months of crampy abdominal pain, sometimes with a burning sensation. The pain is intermittent and is not related to food and was also examined in another hospital where he had an US and a CT scan which were interpreted as normal. The pain sometimes goes up to his chest and causes his shortness of breath. He lost 14 kg during these months, non-intentional. No known family history for cancer or abdominal disease. Had normal bowel movements, no sick relatives, did not travel recently, no use of drugs or alcohol. Had been seen by GI consult and had an EGD and colonoscopy which were normal except for a small transverse colon polyp which was excised.
Physical examination has revealed a thin man, mild tenderness in the epigastrium with no rebound or guarding. RR 18, hr 89, bp 103/58, temp 36.9 and saturation was 96% (RA). Labs have shown no anemia, no leukocytosis or thrombocytosis, normal chemistry and a normal urine analysis. Due to the pleuritic component of the epigastric pain Troponin, ECG and a chest CT were ordered. For the prolonged abdominal pain and weight loss an abdominal CT enterography was added.
Chest CT was normal, abdominal CT has shown 2 small liver lesions (less than 5mm), an enlarged prostate and a partial small bowel malrotation without obstruction (Figures 1 panels A and B).
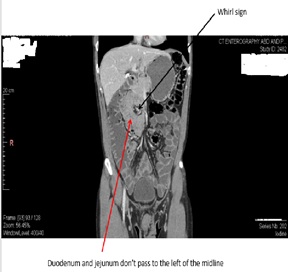 Figure 1: Panel A- Abdominal CT.
Figure 1: Panel A- Abdominal CT.
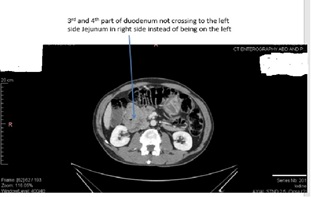 Figure 1: Panel B.
Figure 1: Panel B.
Due to the fact the pain resolved and the patient was a-symptomatic it was decided to have an elective procedure, which was done 5 days after his discharge. The treatment of choice in children is the LADD procedure, and we decided to have him undergo a this as a laparoscopic procedure. We have asked the assistance of an experienced pediatric surgeon to aid us.
The trocar placement was a 10 mm umbilical trocar for the scope and 3 5 mm trocars in a fan like shape with a hand breath to the left and right of the scope trocars, and another 5 mm trocar a hand breath away from the right trocar. Another 5 mm trocar was inserted near the falciform to aid in liver retraction. The team included 2 adult surgeons (GF and ZHP) and an experienced pediatric surgeon (JML). We used a 12 mm pneumoperitoneum during the procedure, and the team was positioned so that one handles the camera and retracts the liver, the other holds a grasper and ultrasonic shears and the last member is aiding with a grasper to aid in moving the bowel. We started with surveying the abdomen and have found the colon in its anatomic position, but a malrotation of the small bowel, with the ligament of Treitz to the right of the spine, and most of the small bowel loops posterior to the mesentery of the right and transverse colon. We mobilized the right and transverse colon, so we can see the mal-rotated small bowel, which was incased in fibrous bands (LADD bands), which were then divided. It was decided against an appendectomy, thus preventing a conversion of a clean operation becoming a contaminated one, surly in an adult who could be educated upon the fact his appendix is not in the RLQ, as well as the wide use of CT which will show his mispositioned appendix if needed. Operative time was about 120 minutes, with a normal surgical and anesthetic course. Post operation, he recovered smoothly, without any complications, and was discharged on day 2. We saw the patient 4 weeks after the surgery, and he was doing well, with resolution of all of his symptoms.
CONCLUSION
A case of adult intestinal malrotation is rare; accuratepreoperative diagnosis and timely surgery are essential because it can causestrangulation of the bowel. Other case reports have shown similar dilemma's in diagnosis and treatment of intestinal malrotation in the adult patient [1,2].
The incidence of this entity in the adult patient islow and preoperative diagnosis is difficult, and if happens is sometimes only an incidental finding [2], as is seen for example in bariatric patients undergoing Gastric Bypass (RYGB) [3]. Because of the vast differential diagnosis in caring for patients with chronic abdominal pain, Computed Tomography (CT) scan can and should play an importantrole in the evaluation of patients with this abnormality [2], and if need be also CT enterography which gives higher resolution and better accuracy [2,3]. An important differential diagnosis in such a patient, without a clear pathology and with weight loss is “Superior Mesenteric Artery Syndrome” in which a mechanical compression of third part of duodenum between SMA, anteriorly, and abdominal aorta, posteriorly causes these symptoms, but this was ruled out with imaging.An accurate preoperative diagnosisof intestinal malrotation was and still is a challenge and it seems that the laparoscopic approach for a LADD procedure is a feasible and safe way of treating this [2,3], even though others advocate for the use of an open procedure [4]. The Ladd procedure, consisting of division of Ladd's bands, widening of the mesentery, and incidental appendectomy, remains the standard surgical repair. Digestive surgeons who care for adults should be familiar with this procedure, and it should be performed, as often as possible, with the assistance of a pediatric surgeon, as was done in our case. One must remember that the decision if one should use operate in an open or laparoscopic approach mainly is dependent upon the physiological state of the patient, as well as the surgeon experience with these techniques.
CONFLICT OF INTEREST
None.
REFERENCES
- Miyano G, Fukuzawa H, Morita K, Kaneshiro M, Miyake H, et al. (2015) Laparoscopic repair of malrotation: what are the indications in neonates and children? J Laparoendosc Adv Surg Tech A 25: 155-158.
- Smith K, Martinez-Quinones P, Hawkins M (2017) Midgut Volvulus in Adults with Congenital Intestinal Malrotation. Am Surg 83: 314-315.
- Hill S, Koontz CS, Langness SM, Wulkan ML (2011) Laparoscopic versus open repair of congenital duodenal obstruction in infants. J Laparoendosc Adv Surg Tech A 21: 961-963.
- Fung AT, Konkin DE, Kanji ZS (2017) Malrotation with midgut volvulus in an adult: a case report and review of the literature. J Surg Case Rep 2017: rjx081.
Citation: Perry Z, Laberge JM, Fried G (2019) A Case Report of an Intestinal Malrotation in an Adult Patient and it's Treatment by a Laparoscopic Ladd Procedure. Archiv Surg S Educ 1: 006.
Copyright: © 2019 Zvi Perry, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.