A New Device for Stable Fixation of the Gallbladder during Single Port Laparoscopic Cholecystectomy
*Corresponding Author(s):
Khanov Vladislav OBashkir State Medical University, Lenina Str 3, Ufa, Bashkortostan Republic, Russian Federation
Email:khanovv@mail.ru
Abstract
A new device to perform a single port laparoscopic cholecystectomy presented. Given the scheme of main components of this device and its possibilities in clinical practice during an operation.
Keywords
Cholecystectomy; Gall bladder; Laparoscopy; Surgery
Introduction
Laparoscopic cholecystectomy is widely performed standard surgical treatment of cholelithiasis. The transition from laparotomy to laparoscopy has significantly decreased the aggressiveness of surgical intervention. However, to date, laparoscopic cholecystectomy requires several (3 or 4) small incisions in the abdomen [1,2]. The techniques, further minimizing the invasiveness of the procedure by reducing the number of trocars used and/or a change in access point, are being develope. Increasingly popular are Natural Orifice Transluminal Endoscopic Surgery (NOTES) techniques, including single port access surgery performed through a single incision in the umbilicus (SILS). While the specialized equipment for single port access surgery is being developed and widely available, the introduction of new methods and techniques of minimally invasive interventions is accompanied by a number of issues, primarily feasibility, efficiency, safety and the possible range of applications, etc. that need to be addressed [3,4]. The surgical technique discussed in this paper is currently under development, and further accumulation of empirical data is required to determine the spectrum of possible expanded clinical use.
Materials and methods
The authors describe their own technique for the treatment of cholelithiasis using SILS laparoscopic approach. In the city hospitals, collaborating with the Department of Surgical Sciences and New Technology Development of Bashkir State Medical University, Ufa, 49 single port access laparoscopic cholecystectomy operations were performed. Out of 49 cases 40 patients were female (81,6%) and 9 were male (18,4%), while the age range was 24 to 73 years.
Safety and careful selection of patients were regarded as a priority. For all patients operated chronic calculous cholecystitis constituted the appropriate indication for a given procedure. Ultrasound examination showed that overall size of concretions did not exceed 3cm. It should be noted that in this patient group, 9 patients had previous history of deferred laparotomy (gynecological diseases), and 4 patients had body mass index (BMI) of 31 kg/m2. As research progressed, the technique was perfected so that the wider variations in clinical decision making regarding the indications for single port access surgery operations were allowed for. The average duration time of the surgical procedure was 79 ± 6,9 min.
Results And Discussion
SILS-port allows for good maneuverability, highly stable and comfortable instrument insertion as well as optimal access to the target tissue. The central working channel allows for any instruments up to 12,5 mm. However, for the convenience of manipulation in the working space there must be no more than 3 instruments used simultaneously, including a laparoscope.
Among the disadvantages of all the available SILS techniques, compared to multi-port laparoscopic surgery, many authors have noted significant difficulty in allocation of the gallbladder neck.
Parallel arrangement of the working tools’ axes greatly complicates the side tractions of the gallbladder. Typically the traction the gallbladder fundus in the cranial direction is performed during laparoscopic cholecystectomy in order to access the neck of the gallbladder and fix it in required position. Creating necessary tension and being able to effectively manipulate the gallbladder in all three dimensions during the operation are crucial in minimizing the risk of iatrogenic injuries of common bile duct [1,3].
Currently there are two most popular techniques used for gallbladder fixation during the procedure: first, using additional specialized curved instrument, which requires special training; second, stitching through the gallbladder fundus with a special needle with a thread drawn through the anterior abdominal wall; – both techniques have some significant drawbacks. The insertion of an additional tool in the working port leads to so-called “tools-conflict”. Moreover, it reduces visibility as the fundus of the gallbladder slips and bends over the fixing tool, being "dumped" on the area of operational impact.
The second technique appears more promising however is extremely elaborate and lengthens the time of surgery considerably. In order to perfect this procedure, we have proposed a way to capture and retain the gall bladder using a specially designed device with a metal string. The proposed method is as follows.
As the pneumoperitoneum is created and the single port access is set, a laparoscope and a dissector are inserted. The abdominal wall is punctured with the original device (Figure 1), a hollow needle with a metal string and a spring mechanism placed inside, which is connected to the button controlling the hook-clip mechanism to capture the strings (Figure 2).
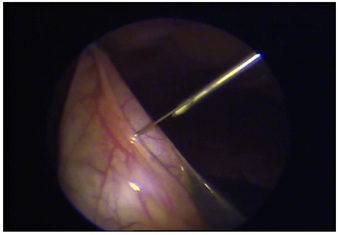 Figure 1: Metal string inside the needle flashes gallbladder wall.
Figure 1: Metal string inside the needle flashes gallbladder wall.
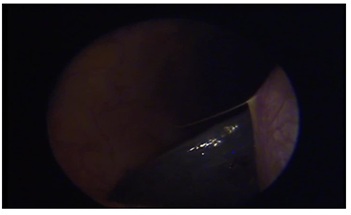 Figure 2: Visualized the end of the string to fix it by the hook-clip mechanism.
Figure 2: Visualized the end of the string to fix it by the hook-clip mechanism.
When the device is positioned next to the gallbladder fundus, a sharpened metal string is released, which pierces through the walls of the bladder (Figure 3). Then the locking device is moved back, grabbing the end of the string, exiting the abdominal cavity through the existing incision in the abdominal wall, pulling the gallbladder until it reaches the inner surface of the abdominal wall that allows us to securely fix the fundus of the gallbladder and get access to the elements of Calot triangle (Figure 4). Having separated the cystic artery and cystic duct, they are being clipped and intersected. Then, in subserous layer the amputation of the gallbladder is performed carefully separating it from the liver bedding. Hemostasis is carefully monitored and the cavity is lavaged of blood clots, pieces of residual tissue and gallbladder coagulation products. After that, the gallbladder is removed along with the port. The scheme of the device is shown on (Figure 5).
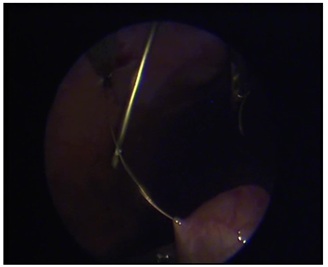 Figure 3: Capturing the end of the string to stretched out on abdominal wall.
Figure 3: Capturing the end of the string to stretched out on abdominal wall.
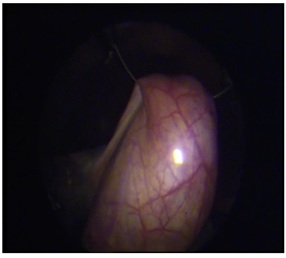 Figure 4: The gallbladder reliably fixed.
Figure 4: The gallbladder reliably fixed.
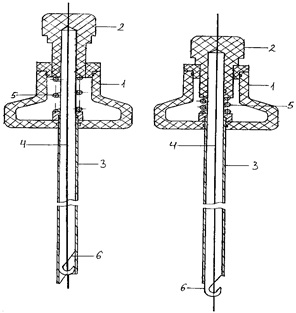 Figure 5: The scheme of the device (1-handle to hold the device, 2- button to move the hook in tube 3, 4- metal string passing through the needle and moving free in tube 3, 5- spring mechanism, 6- hook-shaped clip to fix the string).
Figure 5: The scheme of the device (1-handle to hold the device, 2- button to move the hook in tube 3, 4- metal string passing through the needle and moving free in tube 3, 5- spring mechanism, 6- hook-shaped clip to fix the string).
The technique was successfully applied in 32 cases of single port access laparoscopic cholecystectomy discussed in this paper. Given the positive aspects of the proposed technique such as marked reduction in operation time, reliable and secure fixation of the gallbladder and improved visualization of the elements of the gallbladder neck, there were no complications associated with the use of this method.
In the early post-operation period the patients were closely observed for possible complications, however none had occurred. On the third day the patients were fully examined and the abdominal ultrasonography was performed.
Patients resumed activity on the first day after surgery, pain was minimal and did not require prescription of any narcotic analgesics. All patients were discharged within 5-days after surgery. Sutures were removed on 7-10-day after surgery. 3 months after release all patients had no complaints and felt good, upon being subjected to full re-examination no complications were recorded.
Conclusion
Thus, the research of single port access laparoscopic cholecystectomy has indicated a number of unique issues, not typical for other minimally invasive surgery, which require further consideration and empirical data collection in order to perfect and optimize this technique.
References
- Arezzo A, Passera R, Forcignanò E, Rapetti L, Cirocchi R, et al. (2018) Single-inci- sion laparoscopic cholecystectomy is responsible for increased adverse events: results of a meta-analysis of randomized controlled trials. Surg Endosc 32: 3739-3715.
- Bernhardt J, Sasse S, Ludwig K, Meier PN (2017) Update in natural orifice translumenal endoscopic surgery (NOTES). Curr Opin Gastroenterol 33: 346-351.
- Qiu Z, Sun J, Pu Y, Jiang T, and Cao J, et al. (2011) Learning Curve of Transumbilical Single Incision Laparoscopic Cholecystectomy (SILS): a preliminary study of 80 selected patients with benign gallbladder diseases. World J Surg 35: 2092-2101.
- Barutcu AG, Klein D, Kilian M, Biebl M (2020) Long-term follow-up after single-incision laparoscopic surgery. Surg Endosc 34: 126-132.
Citation: Valentin PN, Oleg GV, Vladislav KO (2023) A new device for stable fixation of the gallbladder during single port laparoscopic cholecystectomy. J Med Stud Res 5: 023.
Copyright: © 2023 Pavlov Valentin N, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.