A Novel Approach to Intrude Incisor by Removable Orthodontic Appliance
*Corresponding Author(s):
Panchali BatraDepartment Of Orthodontics And Dentofacial Orthopaedics, Faculty Of Dentistry, New Delhi, India
Tel:+91 9999908022,
Email:panchali.batra@gmail.com
Abstract
A dynamic smile is desirable at all age groups and orthodontists are smile architects. To construct a beautiful smile the various macro esthetic and micro esthetic factors must be kept in mind. Frontal esthetics is very crucial and poor frontal esthetics can be very bothering for the patient. In this article we are presenting a case report on how a simple removable appliance addressed the chief concern of patient of discrepancy in the level of incisors.
Keywords
INTRODUCTION
Smile is a person’s ability to express a range of emotions and can often determine how well a person can function in society. A beautiful smile is desirable for all age groups.
There are various macro aesthetic [1] and micro aesthetic components that contribute to a dynamic smile [2]. Poor frontal esthetics is usually the chief concern of patients and can lead to pursed smile or low self esteem. Factors that contribute to frontal esthetics are crown height and width, philtrum height, commissure height, inter labial gap, amount of incisal display at rest, amount of incisal display on smile, smile arc, gingival shape and contour, crown height and width [3].
The vertical position of incisors plays a crucial role in frontal esthetics [3].
In this article a case report is being presented on how a simple removable appliance addressed the patient’s chief complaint and improved the frontal smile esthetics by intruding the incisor and leveling the discrepancy of free gingival margin and the incisal edges.
CASE REPORT
A 23 year old male patient presented with chief complaint of discrepancy in level of upper front teeth. A detailed case history and periapical radiograph were taken to rule out etiological factors like trauma. IOPAR did not reveal any periapical pathology (Figure 1).
Figure 1: Pretreatment IOPAR.
Patient was asymptomatic and had no complaint of any pain or sensitivity. Clinical examination revealed a discrepancy in level of incisal edge of the two central incisors with left central incisor extruded by 2 mm. There was also a difference in the level of free gingival margin between the two central incisors. The overall occlusion was satisfactory and the malocclusion was localized to a single tooth (Figures 2 and 3).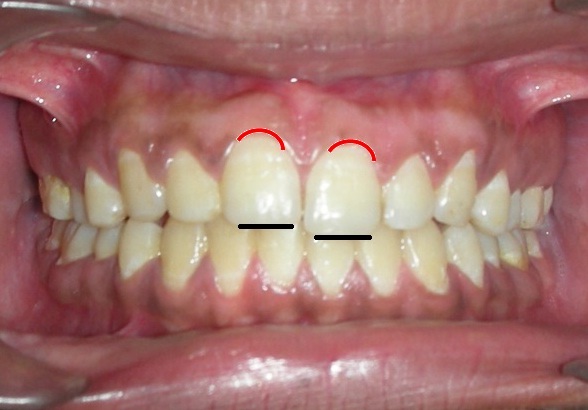
Figure 2: Pre treatment frontal view.
Figure 3: Pre treatment buccal view.
PROBLEM LIST AND TREATMENT OBJECTIVES
After careful evaluation of micro and mini aesthetic factors of his smile, we identified the following treatment objectives:
- To level the incisal edge of the two maxillary central incisors.
- To level the free gingival margins of the two maxillary central incisors.
TREATMENT ALTERNATIVES
The various treatment alternatives available for this case were as follows:
- Extrusion of right central incisor.
- Intrusion of the extruded left central incisor by fixed orthodontic appliance.
- Intrusion of the extruded left central incisor by removable appliance.
- Enameloplasty of the extruded incisor followed by gingivoplasty to correct the discrepancy in the free gingival margin.
Extrusion of right central incisor
Intrusion of the extruded left central incisor by fixed orthodontic appliance
- The use of optimal magnitude of force.
- The use of single point contact in the anterior region.
- The careful selection of point of application with respect to the center of resistance to be intruded.
- Selective intrusion based on anterior tooth geometry.
- Inhibition of eruption of posterior teeth and avoidance of undesirable eruptive mechanism.
- Control over the reactive unit by formation of a posterior anchorage unit.
Intrusion of the extruded left central incisor by removable appliance
Enameloplasty of the extruded incisor followed by gingivoplasty to correct the discrepancy in the free gingival margin
1. The main indication is when a fissure has to be removed and when one third or less of enamel depth is involved.
2. It is indicated in those teeth which have unfavorable height/width ratio.
Method of doing gingivoplasty: Gingivoplasty can be done either through electrosurgery or through soft tissue lasers. The drawbacks of electrosurgery are heat generation and recession [13]. Soft tissue lasers offer a superior degree of operator control while exhibiting decreased biologic side effects. Very fine incisions and surgical revisions are easily achieved with a degree of hemostasis that results in a clean surgical field [14]. Diode lasers operate at a wavelength that is easily absorbed by the gingival tissues, while posing little risk of damaging the tooth structure, and may be used in close proximity to enamel, cementum, existing restorations, or dental implants. Diode lasers may be used in either contact or noncontact mode [15].
We decided to opt for the third treatment alternative i.e., intrusion with removable appliance since it was most conservative treatment option and the malocclusion was confined to a single tooth.
APPLIANCE DESIGN
The appliance was a simple modification of the Hawleys appliance. Hawleys appliance which is a removable appliance consisting of labial bow and adams clasp as its wire components and an acrylic plate is a simple removable appliance for correcting minor malocclusions like proclination of incisors. It can be modified in several ways to act as an interceptive corrective or retentive appliance.
We incorporated a helix in the labial bow in the centre of the tooth to be intruded. The labial bow was positioned in the middle third of the crown. An attachment was bonded on the lingual aspect of the crown to be intruded, as apically as possible (Figures 4 and 5). 
Figure 4: Appliance frontal view.
Figure 5: Appliance Occlusal view.
The bonded bracket/button served as a means of attachment for the elastic which produced the force for intrusion. An intrusive force was applied on central incisor by a of 3/16" red elastic. The average force used for intrusion was 12-15 gram [5]. The patient was instructed to change the elastic daily. The acrylic around tooth to be intruded was trimmed so as not to interfere with intrusion. The desired intrusion was achieved in three weeks. Immediately after the desired intrusion was achieved the bracket was debonded and acrylic was added on the cingulum of the intruded incisor for retention (Figures 6 and 7).
Figure 6: Post treatment frontal view.
Figure 7: Post treatment buccal view.
DISCUSSION
Maxillary incisal edge position is the most important determinant in smile creation because once set, it serves as a reference point to decide the proper tooth proportion and gingival levels. The parameters used to help establish the maxillary incisal edge position are: degree of tooth display, phonetics [16,17] and patient input. When the mouth is relaxed and slightly open, 3.5 mm of the incisal third of the maxillary central incisor should be visible in a young individual. As age increases, the decline in the muscle tonus results in less tooth display. The patients’ desires must be met as best as possible, provided they do not interfere with the parameters previously discussed. The position of the free gingival margin of the anteriors is also a key factor to be kept in mind when designing a harmonious smile.
This patient presented with a vertical discrepancy of 2 mm in the level of incisal edges. Both laypersons and orthodontists can detect even minor incisal edge discrepancies. Laypersons and dentists can detect a discrepancy from 1.5 to 2 mm, whereas orthodontists are critical and can detect even 0.5 mm discrepancy [18]. The acceptability limit for gingival margin discrepancy between the two incisors is 2.1 mm [19,20]. Hence the need to treat this case was justifiable.
In this case we decided to opt for the third treatment alternative i.e., intrusion with removable appliance. The first treatment alternative of extruding the right central incisor was rejected as it would be unaesthetic. The second treatment alternative of fixed orthodontic treatment was not considered because the problem was limited to a single tooth. Apart from that high cost, increased chair side time and oral hygiene maintenance are concerns with fixed orthodontic appliance. The fourth treatment option of enameloplasty with gingivoplasty was rejected because if we do enameloplasty, the natural translucency of the enamel in the anteriors which is esthetic is lost. Moreover the discrepancy in the anterior free gingival margin would not be addressed and to correct that gingivoplasty would be needed. If the shorter tooth has a deeper sulcus, excisional gingivectomy is indicated to move the gingival margin of the shorter tooth apically. But in this case the sulcus depth was same in the two incisors, hence intrusion was indicated. Therefore we opted for the third alternative- Intrusion with removable orthodontic appliance.
A light and continuous force of 12-15 gram was given to the extruded central incisor by attaching elastic of size 3/16" between helix and bracket. No tipping movement was observed because of the presence of labial bow on buccal aspect and acrylic on palatal aspect. Moreover the incisors were upright facilitating intrusion since the forces would be transmitted through the centre of resistance of the tooth. The appliance did not dislodge because of the light force exerted by the elastic. A total intrusion of around 2 mm was achieved within three week by daily changing of elastic. The patient was instructed to wear the appliance 24 hours except during meals. After the desired intrusion was achieved acrylic was added on the cingulum of the intruded incisor to retain the intrusion (Figure 8).
Figure 8: Post treatment smile.
CONCLUSION
It is vivid from the above discussion that the smiles we create was esthetically appealing and functionally sound too. It is our duty to carefully diagnose, analyze and deliver the best to our patients, taking into account all of the discussed factors. A good finished case makes one clinician stand apart from the rest. The smile designing should be as conservative as possible unlike the past. Our aim has to be less reduction of tooth structure and greater esthetics and durability. This simple modification in removable appliance served as a means to intrude the incisor, achieve patient satisfaction improvement in frontal smile esthetics. This design can also be incorporated in the retention phase if minor intrusion is desired.
REFERENCES
- Morley J, Eubank J (2001) Macro esthetic elements of smile design. J Am Dent Assoc 132: 39-45.
- Sarver DM, Ackerman MB (2005) Dynamic smile visualization and quantification and its impact on orthodontic diagnosis and treatment planning. In: Romano R, Bichacho N, Touati B (eds.). The art of smile: integrating Prosthodontics, Orthodontics, Periodontics, Dental Technology and Plastic Surgery. Quintessence Publishers, Chicago, USA. Pg: 99-139.
- Zachrisson BU (1998) Esthetic factors involved in anterior tooth display and the smile: vertical dimension. J Clin Orthod 32: 432-445.
- Sarver DM (2001) The importance of incisor positioning in the esthetic smile: the smile arc. Am J Orthod Dentofacial Orthop 120: 98-111.
- Burstone CR (1977) Deep overbite correction by intrusion. Am J Orthod 72: 1-22.
- Davidovitch M, Rebellato J (1995) Two-couple orthodontic appliance systems utility arches: a two-couple intrusion arch. Semin Orthod 1: 25-30.
- Shroff B, Yoon WM, Lindauer SJ, Burstone CJ (1997) Simultaneous intrusion and retraction using a three-piece base arch. Angle Orthod 67: 455-461.
- Kalra V (1998) Simultaneous intrusion and retraction of the anterior teeth. J Clin Orthod 32: 535-540.
- Nanda R, Marzban R, Kuhlberg A (1998) The Connecticut Intrusion Arch. J Clin Orthod 32: 708-715.
- Carillo R, Buschang PH, Opperman LA, Franco PF, Rossouw EP (2007) Segmental intrusion with mini- screw implant anchorage: a radiographic evaluation. Am J Orthod Dentofacial Orthop 132: 1-6.
- Sturdevant (2014) Fundamentals of tooth preparation and pulp protection. In: Heymann HO, Swift EJ, Ritter AV (eds.). Art and Science of Operative Dentistry. (6th edn), Elsevier, USA. Pg: 167.
- Sarver DM (2011) Enameloplasty and Esthetic Finishing in Orthodontics-Identification and Treatment of Microesthetic Features in Orthodontics Part 1. Journal of Esthetic and Restorative Dentistry 23: 296-302.
- Kalkwarf KL, Krejci RF, Edison AR, Reinhardt RA (1983) Lateral heat production secondary to electrosurgical incisions. Oral Surg Oral Med Oral Pathol 55: 344-348.
- Lee EA (2006) Laser-assisted gingival tissue procedures in esthetic dentistry. Pract Proced Aesthet Dent 18: 2-6.
- Coluzzi DJ (2006) Lasers in dentistry: the future is here. Contemp Esthetics 10: 14-17.
- Pound E (1973) Personalized denture procedures. Dentist Manual. Denar Corporation, USA.
- Bloom DR, Padayachy JN (2006) Increasing occlusal vertical dimension--why, when and how. Br Dent J 200: 251-256.
- Kokich VO, Kokich VG, Kiyak HA (2006) Perceptions of dental professionals and laypersons to altered dental esthetics: asymmetric and symmetric situations. Am J Orthod Dentofacial Orthop 130: 141-151.
- Springer NC, Chang C, Fields HW, Beck FM, Firestone AR, et al.(2011) Smile esthetics from the layperson's perspective. Am J Orthod Dentofacial Orthop 139: 91-101.
- Ker AJ, Chan R, Fields HW, Beck M, Rosenstiel S (2008) Esthetics and smile characteristics from the layperson's perspective: a computer-based survey study. J Am Dent Assoc 139: 1318-1327.
Citation: Batra P, Miglani R, Saalim M (2015) A Novel Approach to Intrude Incisor by Removable Orthodontic Appliance. J Clin Stud Med Case Rep 2: 014.
Copyright: © 2015 Panchali Batra, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.