A novel Method for Sternal Fixation in Cardiac Surgery: Initial Experience
*Corresponding Author(s):
Jitao YangDepartment Of Thoracic And Cardiovascular Surgery, Shandong Provincial PKUcare Luzhong Hospital, Zibo, 255000, China
Email:yjtyang@163.com
Abstract
Objectives: To investigate whether the Ni-Ti-shaped memory alloy embracing plate is an effective treatment for post -sternotomy complications and to see if it can improve the mechanical stability of sternal closure and to evaluate its initial outcome.
Methods: One-hundred twenty patients from January 2012 through December 2015 underwent sternal fixation with the Ni-Ti-shaped memory alloy embracing plate in cardiac sugery. Sternal healing was evaluated by physical examination, wound healing complications and the Computed Tomography (CT) showings of coaptation the sternal halves. The pain scores were recorded preoperatively and postoperatively on day 3 to 7, discharge, 4 weeks, and 3 and 6 months.
Results: The patients with Ni-Ti-shaped memory alloy embracing plate fixation had less postoprative comlications, such as fat liquefication, mediastinitis, sternal dehiscenc. The postoperative pain scores were significantly lower in patients with sternal fixation of embracing plates than that with wire cerclage. The life quanlity was imporoved in embracing plate fixation patients.
Conclusion: The Ni-Ti-shaped memory alloy embracing plate significantly improved the sternal stability closure and life quanlity and reduced postoperative pain in cardiac surgery.
Keywords
Cardiac surgery; Embracing plate; Rigid fixa; Sternal plating
Introduction
With the rapid development of the society and the advances in medical technology, open heart surgery has become one of the most common procedures done in China. The standard approach for open heart surgical procedures is the median sternotomy that can be performed quickly and provides excellent exposure of the heart, which facilitates different cardiac operations, and is well tolerated by most patients [1]. Despite its good exposure, it is not free of complications. Serious wound complications, such as sternal dehiscence and Deep Sternal Wound Infection (DSWI), may occur after median sternotomy. The reported incidence of these complications has ranged from 0.3% to 5.0% in most studies [2]. This variation may be partly due to differences in study design and partly to differences in type of surgical procedures performed and the definitions of these complications. Especially, the devastating complication DSWI or mediastinitis can cause a high mortality rate of up to 15%, with a significantly prolonged hospital stay and the associated increase in cost. Sternal dehiscence and DSWI usually occur together, suggesting that instability of the sternal in the early postoperative period predisposes to infection [3]. So the most essential factor for preventing these complications is a stable and enduring sternal approximation. Various bone fixation materials and sternal closure techniques have been developed in order to optimiz sternal stability, but a reliable technique remains elusive [4,5]. Until now, the cerclage with stainless steel wires remains the standard technique for sternal closure. However, the steel wires can cut into the bone when mechanical stresses concentrated on at them, causing inadequate fixation and sternal dehiscence. Effective rigid osteosynthesis of the sternum is the most essential factor on preventing post-sternotomy complications from occurring by affording greater stability and promoting primary healing of the sternum. Several innovative methods for more rigid fixation of the sternum have been studied, but there is no ideal method yet. Some studies have demonstrated the sternal plating was superior to wire closure in rigid fixation of the sternum in mechanical properties [6-8].
We therefore adopted the Ni-Ti-shaped memory alloy embracing plates (Lanzhou Ximai Memory Alloy co. LTD, Gansu, China). The aim of this study is to determine whether the Ni-Ti-shaped memory alloy embracing plate is an effective treatment for post -sternotomy complications and to see if it can improve the mechanical stability of sternal closure and to evaluate its initial outcome.
Materials and Methods
Patients
This retrospective study included a total of 120 adult patients who underwent internal fixation of the sternum with the Ni-Ti-shaped memory alloy embracing plate from January 2012 through December 2015. The patients consisted of 84(70%) males 40 and 36 (30%) females, with an average age of 68 years (36-80 years). Among these patients, 74 patients underwent Coronary Artery Bypass Graft (CBAG), 30 cases underwent valve surgery, and 16 patients underwent other procedure. This plating was used for fixation of sternum by the selection of the patients and their family. Especially, we tended to suggest the patients accompanied by diabetes, hypertension and heart failure to receive sternal plating. Approval for the study was obtained from the PKUcare Luzhong Hospital Research Ethics Board.
Operative Procedures
Before operation, we measured the width of the sternum conventionally in order to chose the size of the plate. All operations were performed as the same way as it used to be done. Only the unilateral thoracic artery was used in all coronary surgeries in our department. The appropriate size of embracing plates were soaked into the ice-cold water to have good plasticity to allow extension of the embracing arm to a length greater than the width of the sternum while adequate hemostasis. The presternal pectoral muscle tissue was dissected off the anterior table of the sternal body respectively at the 3th, 4th and 5th intercostal space. One wire was placed in the manubrium and one in the region of the body of the sternum at the level of the 2th intercostal space. The wires were tightened carefully to align and approximate the sternal halves. Then the embracing plates were took out of the ice water and placed in the 3th to 5th intercostal space immediately. With the material property of expansion with heat and contract with cold, warm salt water at 40-50°C was poured on the plates. The plates recovered to the preset shape and were secured to the sternal body at appropriate level while two wires were placed in the manubrium and the upper sternum.
Successful rigid sternal closure was defined by physical examination absented with sternal instability, pain, wound healing complications and the Computed Tomography (CT) showings of coaptation the sternal halves. The postoperative sternal pain was evaluated by using a visual analog scale. The CT scans were used to assess sternal bone healing at 3 months. All CT cans were read by two independent radiologists in a department. The postoperative pain scores were recorded by patients independently using Numeric Rating Scale (NRS) and Wong-baker Faces Pain Scale (FPS). The pain scores were recorded preoperatively and postoperatively on day 3 to 7, discharge, 4 weeks, and 3 and 6 months. Additionally, patients rated sternal pain at rest and with coughing, and general movement. In order to compare the difference of between the plate fixation and the standard wire closure, we compared them (Group P )to the patients (N=180) fixed with circlage wire (Group W).
Statistical analysis
SPSS 17.0 software was used for statistical analysis. The group data comparison was made by Fisher’s exact test. A value of p < 0.05 was considered statistically significant.
Results
The overall median follow-up was 6 months (range, 4-12 months). All in hospital deaths were not correlation with the sternal wound complications. The age of the group P was elder that of the group W. And there are more people suffered from osteoporosis. In group P, there was no people with deep sternal infections/ mediastinitis and 5 patients had superficial sternal wound complications, such as fat liquefication. And 3 patients in group W had mediastinitis to receive wound surgery treatment. 15 persons suffered from fat liquefication and 3 patients had sternal dehiscence. All the people with complications were cured after anti-infecton, dressing change and the initial wound debridement. Bacterial culture showed that Staphylococcus aureus was the most common bacterial colonies and the positive rate only 15%. The CT evaluation of sternal healing demonstrated that the patients in the group P had greater healing than those in the group W at both 3 and 6 months. The evaluation of postoperative pain scores demonstrated that less pain in patients from than that from group W. During the period of in hospital, the pain scores in patients with fixation of embracing plates were as much as 30% lower than in ones with wires fixation. The great differences were seen with coughing. Over the 3-month follow up, there’s no significant difference in pain scores for both groups. Postoperative length of hospitalization was significantly shorter in the group P (median 7 VS 9 days). And the first hours drainage volume after operation was significantly reduced in group 20 P than that in group W (median 125 VS 220 ml) (Figures 1&2).
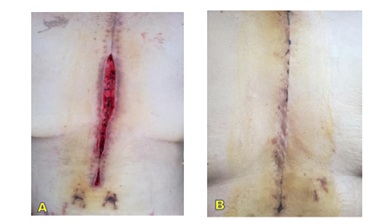 Figure 1: A) Incision dehiscence because of fat liqueficati; B) Well healed wound without any complications.
Figure 1: A) Incision dehiscence because of fat liqueficati; B) Well healed wound without any complications.
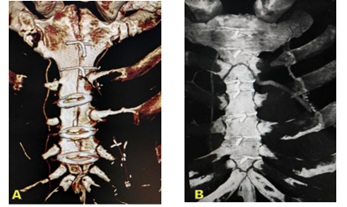 Figure 2: Representative three-dimensional scan reconstructions based on computed 19 tomography scans for embracing plates (A) and conventional wire cerclage (B) Patients.
Figure 2: Representative three-dimensional scan reconstructions based on computed 19 tomography scans for embracing plates (A) and conventional wire cerclage (B) Patients.
Disscusion
Since Julian reintroduced the median sternotomy in 1957 after its initial description by Milton in 1897 [9], over 40 different methods for sternal fixation have been described, claiming to have the ability to maximize stability of the sternotomy closure site. However, there was no one reliable technique remained elusive for poorly described advantages and disadvantages. The conventional cerclage with stainless steel wires remains the standard primary median stenotomy closure technique for most cardiac surgeons. The study found that the steel wires under the normal physiologic loads could cut into the bone and then lead to inadequate fixation and sternal dehiscence, especially for the patients with coughing, and/or osteoporosis. Infection interacted with sternal movement to set up a vicious circle which only could be treated by surgical debridement. The terrible wound complications including mediastinitis and osteomyelitis with a unacceptable morbidity rate of 9.8% to 14% in different studies. And the wound complications could cause a prolonged hospital stay and an increased cost of care. Some centers have begun using rigid titanium plates to fix the sterna, and some studied had demonstrated that rigid sternal plate fixation could significantly improve stability of sternotomy closure and bone healing, reduce early postoperative pain and decrease the incidence of postoperative mediastinitis [6-8,10]. And yet, this kind of plates had to need to be assisted by some other materials, such as: screwdrivers, drill bits, fasteners and so on. Additionally, it had to drill into the sternum, that had the inherent risks of injurying the heart and bypass graftings. Moreover, it took additional plenty of time to drill into the sternum, leading the overall operation time. So we adopted this kind of single claw alloy memory embracing plates. It didn’t need special materials to assist their implantation and to drill into the ribs or sternum, which can save lots of time and avoid the risk of 5 injury to heart and bypass conduits.
In this study, the application of embracing plate fixation to the sternum has shown to increase stability and improve the quality of life. The rigid closure of cutting edges of sternum could effectively reduce the bleeding from the marrow cavity of sternum. The present study proved the safety and practicality of the embracing plates with better distribution of the force across the sternum and a lower risk of bleeding than with sternotomy wires.
Ni-Ti shape-memory embracing plate/fixator was designed to fix long bone fractures, which consists of three components: body, arms, and sawteeth. Each pair of arms resembles a clamp. Animal studies have demonstrated the embracing plate has strong antibending and anti-torsional effects, and relatively low antiloading stress [11]. And some studies also have shown that this kind of embracing plate could provid good fixation of the fracture with minimal trauma to the local blood supply [12-14]. Based on the effectiveness of the embracing plate for the fixation of long bone nonuion, we applied the Ni-Ti shape-memory embracing plate with one pair of arm to fix sternum. Since the shape and stiffness of the nickel-titanium shape-memory allloy can be controlled by temperature, the embracing plate can be easily extended and shaped to fix sternum by temperatures changes. Before implantation, the embracing plate become easily bent and the embracing arm can extent to a length greater than the diameter of the sternm after immersing in ice cold water for minutes. In order to achieve a greater embracing force, we selected the embracing plate with 10-20% smaller in diameter than the diameter of the sternum measured. After implantation, the embracing plate was warmed with water at a temperature of 40-50°C and its original shape were resored. Ideally, the procedure of embracing plate implantation could be performed in a single attempt, and repeated cooling and warming of plate could result in the reduced stiffness.
However, there are some obstacle in clinical application of the Ni-Ti shape-memory embracing plate. Some people be worried about the issue of emergent reenty into the mediatstinum for massive haemorrhage. The embracing plates could be easily bent after cooling, or they could be cut in the middle with standard wire cutters as soon as found massive haemorrhage. Another obstacle to wide application was the cost of device. Indeed, the implants were more expensive than the wires. At our department, the average additional charge was about $ 1500. And our study demonstrated that the stenal fixation with embracing plate apparently decreased the comlication and improved the life quality after cardiac surgery. So compared to the additional hospital charge for post-stenotomy comlications and the increased morbidity and mortality, these expenses become negligible.
Our study had some limitations. The sample size was small. And due to some reasons, the application of the embracing plate was determined by the patient and their families. Some high-risk patients may still chose to sternal fixation with conventional wire cerclage for economic reasons. Otherwise, doctors and patients were not linded to treatment. And different surgry may affect the healing of the wound. So we’d better to recuit more patients and compare the effect in the patients with same surgery to minimize the differences.
In summary, this study demonstrated that rigid sternal stability could be achieved by the Ni-Ti-shaped memory alloy embracing plate fixation. And it could significantly decrease the complication after stonomy, improve the sternal healing and life quanlity and cause less postoperative pain than the conventional cerclage with steel wires.
Acknowledgement
The authors thank Dr. Yu Chen from Peking University People’s Hospital for his prominant language editing. We also thank Mr Xueqing Xu for assistance in collecting imaging.
Conflicts of Interest Statement
The authors state that there is no conflict of interest.
References
- McGregor WE, Payne M, Trumble DR, Farkas KM, Magovern JA (2003) Improvement of sternal closure stability with reinforced steel wires. Ann Thorac Surg 76: 1631-1634.
- Losanoff JE, Collier AD, Wagner-Mann CC, Richman BW, Huff H, et al. (2004) Biomechanical comparison of median sternotomy closures. Ann Thorac Surg 77: 203-209.
- Robicsek F, Fokin A, Cook J, Bhatia D (2000) Sternal instability after midline sternotomy. Thorac Cardiovasc Surg 48: 1-8.
- Robicsek F, Fokin A (2008) Search for a better mousetrap. The quest for an ideal method of sternal closure. Eur J Cardiothorac Surg 33: 767-768.
- Schimmer C, Reents W, Berneder S, Eigel P, Sezer O, et al. (2008) Prevention of sternal dehiscence and infection in high-risk patients: a prospective randomized multicenter trial. Ann Thorac Surg 86: 1897-1904.
- Fawzy H, Osel-Tutu K, Errett L, Latter D, Nonneau D, et al. (2011) Sternal plate fixation for sternal wound reconstruction: initial experience (retrospective study). J Cardiothrac Surg 6: 63.
- Raman J, Lehmann S, De Guzman BJ, Aklog L, Garrett E, et al. (2012) Sternal Closure With Rigid Plate Fixation Versus Wire Closure: A Randomized Controlled Multicenter Trial. Ann Thorac Surg 94: 1854-1861.
- Raman J, Song DH, Bolotin G, Jeevannandam V (2006) Sternal closure with titanium plate fixation--a paradigm shift in preventing mediastinitis. Intera Cardiovasc Surg 5: 336-339.
- Dalton ML, Connally SR, Sealy WC (1992) Julian’s re-introduction of Milton’s operation. Ann Thorac Surg 53: 532-533.
- Arnoni RT, Dantas DC, Arnoni A, Neto CN, Nrto CA (2013) Assessment of sternal closure using titanium plate. Rwv Bras Cir Cardiocxasc 28: 386-390.
- Dai K, Wu X, Zu X (2002) An investigation of the selective stress-shielding effect of shape-memory sawtooth-arm embracing fixator. In Chu YY, Zhao LC (ed.). Shape memory materials and its applications. Trans Tech Publication, Switzerland.
- Su JC, Liu XW, Yu BQ, Li ZD (2010) Shape memory Ni-Ti alloy swan-like bone connector for treatment of humeral shaft nonuion. Int Orthop 34: 369-375.
- Zhao X, Zhu ZA, Sun YH, Wang Y, Zhao J, et al. (2012) Nickel-titanium shape-memory sawtooth-arm embracing fixator for periprosthetic femoral fractures. Int Orthop 36: 619-626.
- Kawakita E, Wang Z, Kato T, Inaba T and Kasai Y (2012) Basic Research on a Cylindrical Implant Made of Shape-Memory Alloy for the Treatment of Long Bone Fracture. Open Orthopae J 6: 239-244.
Citation: Yang J, Li Z, Lei H, Peng L, Qingtao F, et al. (2022) A novel Method for Sternal Fixation in Cardiac Surgery: Initial Experience. J Angiol Vasc Surg 7: 096.
Copyright: © 2022 Jitao Yang, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.