A Particular Case of Gallstoneileus: Diagnostic Imaging and Treatment
*Corresponding Author(s):
Caterina BattagliaDepartment Of Experimental And Clinical Medicine, “Magna Graecia” University, Catanzaro, Italy
Email:caterina.battaglia@unicz.it
Abstract
Gallstone ileus is a rare condition that affects females and older adults. It is caused by a connection between the bowel and the gallbladder that allows the migration of gallstones into the bowel leading to mechanical obstruction. In this case report, we present a case of an 88-year-old female who came to our observation for abdominal pain and vomiting. With the help of a series of radiological investigations, we arrived at the diagnosis of a rare disease called “Gallstone ileus”.
Introduction
Gallstone ileus is an uncommon mechanical occlusive syndrome caused by the migration of one or more gallstones from the bile ducts into the intestinal lumen in patients with a history of cholecystitis or cholecystic calculus. In most cases, the calcolotic formations (often voluminous 2-3cm) migrate through a cholecystic or choledochal spontaneous fistula up to the distal tract of the ileum. In some rare cases, it may have other localizations: proximal ileum, fasting, colon, and stomach/duodenum (Bouveret syndrome). Clinically, patients present with non-specific abdominal symptomatology: nausea, vomiting and diffuse abdominal pain that may vary depending on the location of the obstruction. Abdominal Computed Tomography (CT) is consideredthe gold standard and permits us to find the socalled “Rigler Triad” and to make a preoperative diagnosis.The presence of at least two signs between pneumonia, complete or partial obstruction of the small intestine, and presence of ileal endoluminal calculus are pathognomonic for diagnosis. Unfortunately, is present only in 40% of patients and the three signs only in 10% [1]. In recent years, ultrasonography also become increasingly important; In fact, ultrasound is helpful for the research of the three signs of “Rigler Triad” and allows to verify the presence of residual stones in the gallbladder or choledochal with a sensitivity higher than the radiographic examination [2-4]. The association of ultrasound with the x-ray examination of the abdomen increases the diagnostic sensitivity (definitive diagnosis 74%), especially when the abdominal X-ray is made with an oral contrast agent that could detect two other additional signs: “Forget sign” (passage of the contrast around a radiopaque calculation with a snake-head appearance) and “Petren sign” (enhancement of the contrast agent between the gallbladder and small intestine through the fistulous path) [2,3]. Indeed, CT is the examination with the highest diagnostic sensitivity and specificity. It really sensitive to evaluate the site of the obstruction and could also give information about the size of the ectopic calculus, as demonstrated in the literature, that could be founded through the rectum [4].
Case Presentation
In December 2021, an 88-year-old female patient came to our observation and arrived at the Emergency Room for diffuse abdominal pain and vomiting in the clinical suspicion of intestinal occlusion. The abdominal CT examination performed in the primary conditions only highlights that the gallbladder appeared with thickened walls, fluid and aerial material in coexisting air density bubbles, and diffuse intraparenchymal aereobilia (Figure 1). We appreciate close relationships of contiguity between the gallbladder and the adjacent duodenal tract with signs of imbibition of the surrounding and locoregional fat, coexisting fluid distension of some intestinal loops with a leveled appearance, and fluid peritoneal imbibition (Figure 2); moreover, it is found in the context of one of these loops, in the hemiabdomen at left, a nuancedly hyperdense formation with a size of 30 mm with suspect of lithiasis meaning (Figure 3).
 Figure 1: CT axial showed pneumobilia, particularly noticeableinthe left intrahepatic biliary tree.
Figure 1: CT axial showed pneumobilia, particularly noticeableinthe left intrahepatic biliary tree.
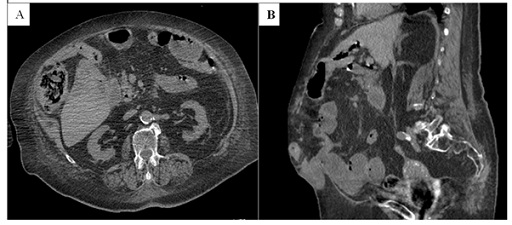 Figure 2: CT axial (A) and Sagittal (B) showedthe relationship between gallbladder and duodenum.
Figure 2: CT axial (A) and Sagittal (B) showedthe relationship between gallbladder and duodenum.
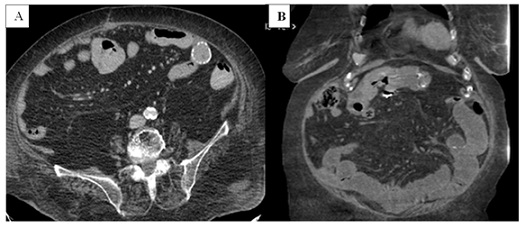 Figure 3: CT axial (A) and Coronal (B) showed anoval/rounded formation with calcific walls in a left loop from probable Lithiasis Formation.
Figure 3: CT axial (A) and Coronal (B) showed anoval/rounded formation with calcific walls in a left loop from probable Lithiasis Formation.
The patient was then admitted to the Department of General Surgery of our Hospital and subjected to radiological investigation with contrast (Gastrografin 360 mg) for the study of the gastro-trans-intestinal tract that confirmed the diagnosis of occlusion of the small intestine characterized by marked dilation of the fast-ileal loops, lack of opacification of the colic frame and fistulabillion-duodenal (Figure 4).
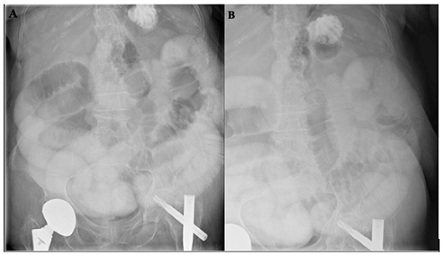 Figure 4: PA (A) and Oblique (B) direct abdominal radiographs showed marked dilation of the fast-ileal loops.
Figure 4: PA (A) and Oblique (B) direct abdominal radiographs showed marked dilation of the fast-ileal loops.
The radiological suspicion of gallstone ileus intestinal occlusion is confirmed, as indicated in the emergency surgical procedure by enterolitotomy, closure of the fistulous path, and cholecystectomy executable in two stages as happened in our case considering the age and comorbidities of the patient.
Discussion
The gallstone ileus was first described in 1654 by a Danish physician, Thomas Bartholin (1616-1680). It is a rare cause of obstruction of the small intestine (1-3%). In elderly patients, however, it can affect up to 25% of cases and is more frequent in women and patients with biliary lithiasis. It’s a condition related to patients with a history of gallbladder lithiasis and recurrent episodes of cholecystitis where the high-pressure effect, inflammation, and ischemia cause erosion of the bowel wall itself and choledochal, resulting in the formation of a bilious fistular pathway digestive, frequently between the gallbladder and the duodenum which follows the migration of the calculus into the enteric tract where it usually stops at the ileum terminal/ileocecal valve determining a typical picture of the acute abdomen from mechanical occlusion [5]. The literature describes at least three types of bilo-digestive fistulas: cholecyst-duodenal (65-77%), cholecyst-colic (10-25%), and cholecyst-gastric (5%) [6]. The evacuation of the calculation through the rectum can occur if the calculation’s size does not exceed 2 cm. Radiological diagnosis has significantly improved with the increasingly widespread use of CT showing better than direct abdominal X-ray; Rigler’s triad is a small bowel obstruction picture associated with pneumonia and evidence of gallstone along the lumen of the enteric tract. The calculation, usually large (2-3cm) only in 12% of cases could be calcific, but sometimes it is difficult to identify given its similar density to intestinal contents. In addition, in the radiological suspicion of gallstone ileus, the investigation can be supplemented with X-rays with a contrast agent (Barium or Gastrografin) to research the site of fistulation, often between the gallbladder and the duodenum, which is very useful for therapeutic purposes.
The mortality of this particular disease is unfortunately still very high; this is also about the increased age of the patients, the comorbidities with which it is often associated (dysmetabolic and cardiovascular), the late onset of symptoms, and the difficulty of early diagnosis [7]. However, today, with a CT scan, it is possible to make an accurate pre-surgery diagnosis allowing surgeons to make a better plan of surgery and avoid exploratory laparotomy with the risk of complications. The therapeutic choice in the gallstone ileus can’t be separated from surgery in a single time when the calculus exceeds 2.5 cm. The surgical intervention consists of enterolitotomy, closure of the fistulous via and cholecystectomy, even in subjects with a high risk (elderly, diabetic, obese, cardiopathic) which are adequately prepared for surgery to reduce the possibility of postoperative complications. More conservative approaches have recently been proposed in laparoscopy and extracorporeal lithotripsy; endoscopic extraction can be performed in patients with Bouveret syndrome, occlusion of the duodenum and colon, especially in older patients that are not eligible for surgery [8]. Lithotripsy is classified into several types: mechanical, electrohydraulic, and extracorporeal. The latest is the most used but with minimal effect for the possibility of recurrence in the reconstitution of the calculation after its fragmentation. Therefore, it is believed that the only enterolitotomy is the procedure of choice in the urgent treatment of intestinal obstruction from the biliary ileum.
References
- Sammartano A, Frazzetta M, Furgiuele G, Frazzetta F, Vetri G, et al. (2006) Ileo biliare: diagnosi e trattamento. Case report. Journal of the Italian Association of Hospital Surgeons 27: 363-367.
- Beuran M, Ivanov I, Venter MD, Davila C (2010) Gallstone ileus--clinical and therapeutic aspects. J Med Life 3: 7.
- Ploneda-Valencia CF, Gallo-Morales M, Rinchon C, Navarro-Muñiz E, Bautista-López CA, et al. (2017) Gallstone ileus: An overview of the literature. Rev Gastroenterol Mex 82: 248-254.
- De Giorgi A, Caranti A, Moro F, Parisi C, Molino C, et al. (2015) Spontaneous Resolution of Gallstone Ileus with Giant Stone: A Case Report and Literature Review. J Am Geriatr Soc 63: 1964-1965.
- Zimadlová D, Hoffmann P, Bártová J (2009) Gallstone ileus: case report and review of literature. Page no: 136-139.
- Ganz E (2018) Trattamento dell’ileo biliare associato a fistola colecisto-duodenale: accorgimenti per ridurre la mortalità. Chirurgia.
- Yu C-Y (2005) Value of CT in the diagnosis and management of gallstone ileus. World J Gastroenterol 11: 2142-2147.
- Maiss J, Hochberger J, Hahn EG, Lederer R, Schneider HT, et al. (2004) Successful laserlithotripsy in Bouveret’s syndrome using a new frequency doubled doublepulse Nd:YAG laser (FREDDY). Scand J Gastroenterol 39: 791-794.
Citation: Battaglia C, Natoli N, Ferrarelli A, Barresi D, Petullà M, et al. (2022) A Particular Case of Gallstoneileus: Diagnostic Imaging and Treatment. J Clin Stud Med Case Rep 9: 0145.
Copyright: © 2022 Caterina Battaglia, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.