A Pilot Study on Cultural Stress Anxiety Syndrome, Its Implications on Aging, Gene Expression and Treatment Strategies
*Corresponding Author(s):
Howard Murad MD., FAADDepartment Of Medicine, Inclusive Health Medical Group, University Of California, Los Angeles, California, United States
Tel:+1 8889968723,
Email:drmurad@murad.com
Abstract
Introduction
With advances in technology and our interconnectedness enhanced, the evolution of human life has created a new type of stress, Cultural Stress (CS) and this type of stress has given way to a recognizable syndrome, Cultural Stress Anxiety Syndrome (CSAS), where isolation, anxiety, sedentary lifestyles and depression are the norm and may hasten senescence.
Objective
The purpose of this pilot study is to explore the effectiveness of an inclusive health method to treat CSAS.
Methods
Six female patients were treated for 24 weeks with an inclusive health protocol (internal care, external care and emotional care) designed to reverse CSAS, rejuvenate cellular health and slow related degenerative cell aging processes. Clinical tests such as a comprehensive metabolic panel, blood pressure screenings, BMI/weight, stress test, as well as questionnaires, interviews and journaling were used to establish baseline measures, mid-point and final results. This included cohen perceived stress scale; patient health questionnaire PHQ-9; cultural stress questionnaire; dermatology self-reporting skin questionnaire; appearance questionnaire and video interviews; omnia photos; visia photos; clarity pro evaluations; blood pressure and body composition using an RJL system; skin biopsies and a global gene expression analysis using affymetrix microarrays.
Results
Subjects eliminated the symptoms of CSAS and gene expression examination showed positive results in down-regulation and up-regulation of the genes that influence senescence. Our findings show that inclusive treatment for CSAS can produce positive changes in total wellness and may reduce aging. In specific, we found that treatments that support the cellular water principle theory-which aims to fortify cells and connective tissue, Increase Intracellular Water (ICW) and boost cellular immunity-and address internal, external and emotional stress due to CS, may be useful to encourage maximal youth in aging patients and stave off age-related cellular degeneration.
Discussion
Accordingly, lifestyle and behavioral management therapies that improve cell health and fortification, in concert with medical treatments, may have the most profound effects on CSAS and epigenetic aging factors.
Keywords
Aging; Anxiety; Depression; Epigenetics; Life stress; Psychological stress
INTRODUCTION
Epidemiological studies are clear about the deleterious effects of stress on health and aging [1-3]. Stress can cause disease, enhance aging and shorten lifespan [4-6]. Although complex, most kinds of stress are easy to identify: acute stress, episodic acute stress, chronic stress and all types of stress share similarities in how they affect the way the body functions [7,8]. However, more recent examination has produced the need for a new category of stress called Cultural Stress (CS) [9]. CS identifies stress from political, climatological, technological and cultural changes and it is a direct result of our interconnectedness and advances in technology. It is also symptomatic of long commutes, overpopulation, noise pollution, toxin exposure through consumables [10] and the incessant use of smart phones, to name a few things. While CS is manmade, it is largely unavoidable in today’s modern society, for those who live on the grid, unless a conscious effort is made to prevent exposure. Even though CS is wholly unnecessary for survival, it can be hard to identify as it is akin to the constant, perhaps unidentifiable, yet equally obtrusive hum of a refrigerator and exists like a ceaseless ringing phone that demands subconscious and conscious management. Patients, most of the time, are conditioned to the continuous stress of CS and are, therefore, unaware that the collection of symptoms and anxiety they experience can be traced back to CS. CS superimposes all other stress types and may even be the cause of acute, episodic acute or chronic stress.
Until now, stress has been hard to define appropriately enough to establish a clear treatment model that addresses all patients’ specific needs [9,11]. Currently, about 12% of all Americans take antidepressants to handle stress [12]. Another report indicates that physicians prescribe these drugs for as many on-label uses as they do for off-label use [13]. An NBC report states that one in six Americans currently takes some kind of psychiatric drug [12]. Clearly, stress models of the past fail to identify holistic or inclusive treatments that attack the causes of stress, if they can be addressed. Rather, treatment of stress’ symptoms come in the form of vague preventive strategies or prescribed medications, which may also produce unwanted side-effects. Moreover, stress-induced symptoms and exacerbations in patients can present in various ways and to certain degrees, depending on each person’s stress threshold, given health, coping skills or even genetics [3]. Indeed, conventional treatments have largely addressed symptoms and are only commenced once health decreases and disorders are present.
We believe, however, that if CS is decreased or eliminated and resultant CSAS is attenuated, then overall health may improve and senescence could be postponed. Researchers have clearly established a bi-directional relationship between stress and body homeostasis, regardless of the stress type. Systemically, the body is programmed to acclimatize to extrinsic and intrinsic influences and stress causes both adaptive and resistance responses [14]. Because of this, we postulate that treatment of CSAS will not only eliminate the toll its symptoms take on health, but CSAS treatment may also help to alleviate the effects of other types of stress, in specific, chronic stress. Accordingly, we believe that CSAS is a serious, yet unrecognized problem that encourages health declines and may work to hasten age-related processes. While several singular methods have been used in the past to treat stress, CSAS requires comprehensive, multidisciplinary treatment. As such, within this pilot study, we hypothesized if one can reduce stress including CS and resultant CSAS to improve overall health by engaging in inclusive health activities (activities that function on the cellular and mechanistic level, influence intracellular water balance and genetic expression), then one may benefit from positive health outcomes that influence senescence.
METHODS
Defining cultural stress anxiety syndrome
Understanding the effects of stress including CSAS
Isolation
Anxiety
Sedentary lifestyle
Depression
Attack root causes of cultural stress
The cellular water principle theory
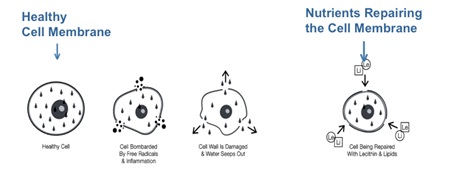 Figure 1: Cell deterioration and fortification. This figure illustrates the cellular water principle theory.
Figure 1: Cell deterioration and fortification. This figure illustrates the cellular water principle theory.EVALUATION AND TREATMENT
External care: To address innate immunity; strengthen cutaneous defenses to external influences or invaders. At the start of the study and each day after, the subjects performed a daily skin care regimen. External care included patient-specific cleansers, treatments and hydration to repair damage and protect and fortify the skin’s barrier function and connective tissue from external factors such as UV rays as well as collagen-deposition and -formation encouraging agents and treatments.
Internal care: To encourage adaptive immunity. Diagnostic tests at day one, assisted in determining systemic disease such as endocrine system or vascular disorders, so therapeutic, systemic care could be initiated. Therapeutic care during the first week of treatment included nutritional guidance on how to eat a low-acid diet replete with vegetables and fruits, lean meats and minimally processed foods. It also included formal physical activity classes two times a week during the entire study such as hiking and dance classes and encouraged participants to increase activity at home to reduce sedentary lifestyles. Also on day one of the study, our subjects commenced needs-based prescription medication and supplements including sleep-encouraging supplements:
• A supplement designed to encourage restful sleep including chamomile, valerian, lavender, melatonin and GABA
• Multivitamin and mineral supplement. An iron-free, comprehensive and balanced formula containing all the major vitamins, minerals and trace minerals
• Antioxidant supplement formula
• High-potency B complex supplement providing all eight essential B vitamins: thiamine (B1), riboflavin (B2), niacin (B3), pantothenic acid (B5), pyridoxine (B6), folic acid (B9), cyanocobalamin (B12), biotin (B7)
• Essential fatty acid supplement providing omega-3 fatty acids. This was in the form of fish oil, flaxseed oil, or ground flaxseeds added to food, or in capsule form
• Lecithin supplement. Soy lecithin granules were sprinkled on or added to foods or added via liquid soy lecithin in capsule form
• Glucosamine
• Calcium supplement for bone health between 1000 mg to 1500 mg of calcium with vitamin D daily, depending on the subject’s dietary intake of calcium
Emotional care: To support psychological and social balance. Stress reduction “feel-good” services such as those provided within the spa environment were used, as well as activities like yoga, support group participation, art classes, positive living lectures, daily reading of life-affirmation flashcards and counseling to nurture the psyche. Eleven insight cards, a journal and an explanation of CS were given at the beginning of the study and subjects were asked to download an app that had more life-affirming quotes and artwork. The insight cards were used as a tool to promote well-being and reduce CS. Focused attention to the cards was recommended twice a day and journaling was once a day during the entire study.
During the 24-week study, participant performed a self-assessment of emotional and physical well-being by completing several brief questionnaires. In-office tests were also performed:
• Cohen perceived stress scale
• Patient health questionnaire PHQ-9, cultural stress questionnaire by Murad
• Dermatology self-reporting skin questionnaire
• Appearance questionnaire and video interviews
• Omnia photos, visia photos, and clarity pros evaluations
• Blood pressure and body composition with an RJL system
• Blood tests (complete metabolic panel)
• Skin biopsy
• Global gene expression analysis using affymetrix microarrays
Blood and skin biopsy samples were collected at baseline, 12 weeks and 24 weeks to measure every single gene in the body. Our pilot study focused on the 12-week dataset as this analysis contains the use of the benjamini-hochberg FDR correction. Accordingly, there is a large amount of data with the FDR correction in both the 12-week blood and skin sample datasets.
A body composition using the RJL system allowed scientific data for cellular health among the subjects. The data included body fat, fat-free mass, intracellular water, extracellular water and total-body water percentages. Clarity pro, an analytical machine, monitored the progression of the subjects’ skin condition throughout the study. The technology allowed baseline, week 12 and week 24 data comparisons in order to detect any changes topically for each individual subject. For further investigation regarding gene expression, the samples from the blood tests and skin biopsies were analyzed. As expected, the blood and skin datasets had little in common. Based on the small overlap in specific genes, each tissue was further analyzed independently (Figure 2).
Global gene expression analysis was carried out using affymetrix microarrays to identify gene expression changes correlated with improved health outcomes as a result of the program. Affymetrix microarrays contain approximately 45,000 transcripts representing the ~23,000 human genes and are an ideal method for screening the entire genome. Samples were processed according to standard affymetrix microarray protocols.
Data analysis was conducted using gene spring software. Paired t-tests were performed to identify statistically significant changes in gene expression between the following time points:
• 12 Week versus Baseline (skin)
• 12 Week versus Baseline (blood)
• 24 Week versus Baseline (skin)
• 24 Week versus Baseline (blood)
Patients were given ongoing questionnaires and interviewed on the status of their current stress levels. This was done both orally and through written responses, video interviews and journaling twice daily. Finally, an assessment of current exposure to CS was necessary to determine external influences that may enhance CSAS. Depending on stress levels and symptoms determined, medical interventions were explored with the objective of only short-term use and discontinued once symptoms reduced enough and general health and cellular immunity improved. Also, patients were instructed in how to avoid CS so as not to encourage CSAS, with the following tips [20]:
Tips for reducing cultural stress
- The first step in reducing CS is to determine its sources. Once the sources are identified, develop a plan of action to reduce their impact
- Practice being mindful: Take some time each day to meditate or be quiet and enjoy the simple rhythms of life
- If you are stuck in traffic and late for an appointment, accept the fact that you can’t control the situation. One thing you can control is how you react to these situations. Try to make the best of it. Why have a bad day when you can have a good day?
- Exercise regularly: Go for a walk, do yoga or take an exercise class. Being physically active, even for just a few minutes can make a difference in the way you feel
- Nourish your body for optimum health: Make it a habit to avoid the Standard American Diet. Get foods that encourage and increase the water content in your body - a diet full of whole grains, fresh fruit and vegetables, good fats and proteins. Take a nutritional supplement to fill the nutritional gaps in your diet
- Get a good night’s sleep: Americans sleep less than people in any industrialized country in the world. You need seven to nine hours of sleep every night to fully restore the body. Don’t lose sleep; find the time to recharge your body at night so you have the energy to face the challenges that come up every day
Mind-Body connection
Aside from the mind, the body may be addressed with exercise techniques that reduce stress and improve circulation, as well as tackle sedentary lifestyles. Our study’s participants were encouraged to join support groups, cooking classes, walking clubs, exercise groups two to three times per week and sign up for new experiences such as dancing, art, or photography classes. They were challenged to do more things like hiking and attend cooking classes. All six participants met twice a week with a trainer to exercise. They also attended an art therapy class that encouraged coloring outside the lines and laughter. Pet adoption was also suggested as pets have been shown to help reduce stress.
RESULTS
At the midpoint of the study, based on self-assessments, the participants also reduced overall depression from 33% to 24%. Intracellular water percentages increased within the overall group. Clarity pro analyses also indicated noticeable improvements in facial skin. The women were able to reduce wrinkles, sun damage, acne, and UV damage. With such results, an increase in confidence allowed the women to handle new challenges in their daily lives, such as promotions and even address issues preventing them from being better mothers. All in all, the women successfully completed the program with various internal, external and emotional improvements. The midpoint results, which had the most prominent change among the women, showed NFAT5 activity was reduced. In fact, biopsies showed 1,425 genes were expressed in a positive way to slow age-related deteriorations. In the blood samples, 200 gene-expression markers showed reductions and increases in a positive way, as well. Of those 200 markers, 100 overlapped with tissue sample results and both tissue and blood samples produced identical positive results (Table 1).
| Number of Two-Fold Genes | |||||
| 12 Wk-vs-Wk 0 | 24 Wk-vs-Wk 0 | ||||
| No correction | With FDR | No correction | With FDR | ||
| Blood | Increased | 240 | 3 | 60 | 0 |
| Decreased | 3357 | 359 | 168 | 0 | |
| Total | 3597 | 362 | 228 | 0 | |
| Skin | Increased | 156 | 61 | 80 | 0 |
| Decreased | 2532 | 1513 | 168 | 0 | |
| Total | 2688 | 1574 | 248 | 0 | |
Summary of key gene expression findings
• NFAT5 is a molecule that is increased in response to hypertonic stress
• NFAT5 is a transcription factor that regulates multiple biological functions and genes
• A decrease in NFAT5 at 12 weeks suggests that the levels were higher at baseline. This is consistent with the idea that at baseline the cells were exposed hypertonic stress that was diminished by participation in the inclusive health protocol
• Each of the datasets (blood and skin) contains multiple genes that regulate or are regulated by NFAT5
Reduction of NFAT5 during the period of the study with the most changes within the three-facet approach indicates a correlation between inclusive health therapies and whole body wellness (Figures 3-6). Changes in environmental conditions have been scientifically proven to change protein expression due to increases in euchromatin and heterochromin in the nucleosome structures of the DNA. While such changes in epigenetics can have positive or negative effects on individuals health-wise such as the inactivation or activation of tumor suppression genes like connexin [50], the CSAS inclusive health program seemed to have only positive effects on reducing negative transcription factors such as NFAT5. These results showed that an inclusive protocol based on cellular health could reverse CSAS, improve health and delay cellular deteriorations including those due to aging.
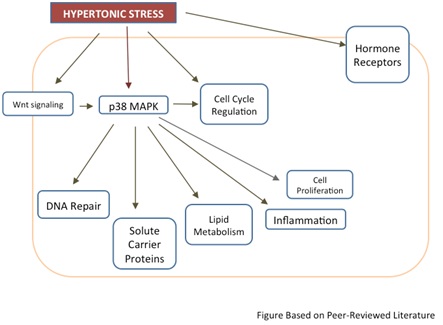 Figure 3: Normal responses to hypertonic stress. This figure illustrates the normal reaction to hypertonic stress on biological function.
Figure 3: Normal responses to hypertonic stress. This figure illustrates the normal reaction to hypertonic stress on biological function.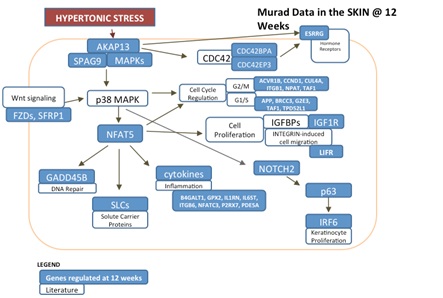 Figure 4: Responses to hypertonic stress in skin biopsies. This figure illustrates the responses, within skin samples, to hypertonic stress after 12 weeks of treatment.
Figure 4: Responses to hypertonic stress in skin biopsies. This figure illustrates the responses, within skin samples, to hypertonic stress after 12 weeks of treatment.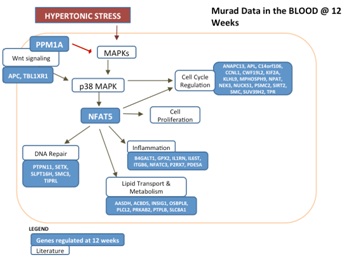 Figure 5: Responses to hypertonic stress in blood tests. This figure illustrates the responses, within blood samples, to hypertonic stress after 12 weeks of treatment.
Figure 5: Responses to hypertonic stress in blood tests. This figure illustrates the responses, within blood samples, to hypertonic stress after 12 weeks of treatment.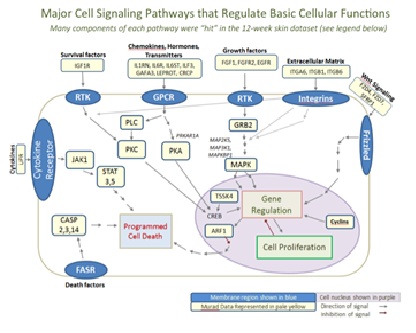 Figure 6: Regulation of biological pathways. This figure summarizes the data collected and shows that multiple, major mechanisms were contained within the dataset(s).
Figure 6: Regulation of biological pathways. This figure summarizes the data collected and shows that multiple, major mechanisms were contained within the dataset(s).Hormone regulation
AR [Androgen Receptor]
CRCP [CGRP Receptor Component]
ESRRG [Estrogen-Related Receptor Gamma]
GLCCI1 [Glucocorticoid Induced Transcript 1]
GNRHR2 [Gonadotropin-Releasing Hormone (Type 2) Receptor 2]
GRB2 [Growth Factor Receptor-Bound protein 2]
IGF1R [Insulin-like Growth Factor 1 Receptor]
LEPROT [Leptin Receptor Overlapping Transcript]
PDGFA [Platelet Derived Growth Factor Alpha polypeptide]
PGRMC1 [Progesterone Receptor Membrane Component 1]
PRLR [Prolactin Receptor]
PTGFR [Prostaglandin F Receptor]
THRAP3 [Thyroid Hormone Receptor Associated Protein 3]
Additional mechanisms identified using biological pathways analysis
| Gene Id | Gene Name |
| IGF1R | Insulin-like Growth Factor 1 Receptor |
| IL1RN | Interleukin 1 Receptor Antagonist |
| IL6R, IL6ST | Interleukin 6 Receptor& Interleukin 6 Signal Transducer |
| ILF3 | Interleukin Enhance Binding Factor 3 |
| GAFA3 | FGF-2 Activity –Associated Protein 3 |
| LEPROT | Leptin Receptor Overlapping Transcript |
| CRCP | CGRP Receptor Component |
| FGF1 | Fibroblast Growth Factor 1 |
| FGFR2 | Fibroblast growth factor receptor 2 |
| EGFR | Epidermal Growth Factor Receptor |
| ITGA^ | Integrin, Alpha 6 |
| ITGB1 | Integrin, Beta 1 |
| ITGB6 | Integrin, Beta 6 |
| FZD4, FZD7 | Frizzled Homolog 4& 7 |
| SFRP1 | Secreted Frizzled-Related Protein 1 |
| PLCB4, PLCZ1 | Phospholipase C, Beta 4& Zeta 1 |
| CREB | (TSSK4) Positive Regulation of CREB Transcription Factor Activity |
| GRB2 | Groeth Factor Receptor-Bound Protein 2 |
| CASP2, CASP3, CSAP14 and CFLAR | Caspase 2,3& 14, and the CASP8 and FADD-like Apoptosis Regulator |
| JAK | Janus Kinase 1 |
| STAT3 | Signal Transducer and Activator of Transcription 3 |
| STAT5 | Signal Transducer and Activator of Transcription 5B |
| ARF1 | ADP-Ribosylation Factor 1 |
| MAP2K5, MAP3K1, MAPKBP1 | Mitogen-Activated Protein Kinase Kinase 5, Mitogen-Activated Protein Kinase Kinase 1, Mitogen-Activated Protein Kinase Binding Protein 1 |
| LIFR | Leukemia Inhibitory Factor Receptor |
| CCND1, CCNG2, CCNK, CCNL1 | Cyclins D1, G2, k & L1 |
| PRKAR1A(PKA) | Protein Kinase, cAMP-Dependent, Regulatory, Type 1, Alpha |
| PRKCI(PKC) | Protein Kinase C, Iota |
Table 2: Genes listed in the major cell signaling pathways.
Major transcription factors regulated in blood
Skin sample pathways
• Cell-cell adhesion
• Extracellular matrix regulation
• Epidermal growth factor pathway
• Integrin-regulated matrix functions
• Cell proliferation and differentiation
• TGFβ-Induced Regulation of the Cell Cycle
• Wnt Regulation of the Cell Cycle
• Cellular metabolism
• Hormone receptors
Cellular metabolism
• Several ATPase family genes: ATP1B1, ATP13A3, ATAD2B, ATP2B4, ATP6V1A, ATP6V1C1, ATP6V1G2
• Cellular respiration genes: CYCS [Cytochrome C], UQCRC2 [Ubiquinol-Cytochrome C Reductase Core protein II], NDUFS1 [NADH-Coenzyme Q Reductase]
• ~20 solute carrier /transporter molecules: SLC2A4 [Solute Carrier family 2 (facilitated glucose transporter), member 4], SLC17A5 [Solute Carrier family 17 (anion/sugar transporter), member 5], Other membrane transporters: SLC10A1, SLC11A2, SLC13A1, SLC16A10, SLC16A7, SLC23A2, SLC26A2, SLC26A2, SLC35E1, SLC38A1, SLC38A4, SLC38A7, SLC39A6, SLC39A8, SLC39A8, SLC46A1, SLC4A1, SLC4A4, SLC7A8, SLC8A1
• ~40 zinc-finger related genes (DNA transcription): ZBED6, ZBTB33, ZBTB38, ZBTB40, ZBTB43, ZC3H11A, ZDHHC21, ZEB1, ZEB2, ZFP106, ZFR, ZFYVE9, ZKSCAN1, ZMYM5, ZMYM6, ZMYND11, ZNF148, NF22, ZNF248, ZNF254, ZNF264, ZNF275, ZNF292, ZNF395, ZNF396, ZNF397OS, ZNF434, ZNF440, ZNF479, ZNF480, ZNF496, ZNF551, ZNF567, ZNF621, ZNF641, ZNF652, ZNF704, ZNF91, ZSCAN18
• LIPE [Hormone-sensitive lipase ]
• STAT3 and STAT5B [Signal Transducer and Activator of Transcription 3 and 5B]
Skin function: Barrier and extracellular matrix integrity
COL4A3 [Collagen, Type IV, Alpha 3]
COL6A1 [Collagen, Type VI, Alpha 1]
DEFA1 [Defensin Alpha 1]
BMPR2 [Bone Morphogenetic Protein Receptor, Type II (Serine/Threonine kinase)]
CDH1 and CDH4 [Cadherin 1 and 4]
DCT [Dopachrome Tautomerase]
DEFA1 [Defensin Alpha 1]
DSG2 [Desmoglein 2]
ITGA6, ITGB1, ITGB6 [Integrins A6, B1, and B6]
LAMA4 [Laminin A4]
PLOD2 [Procollagen-Lysine 2-Oxoglutarate 5-Dioxygenase 2]
S100A1, S100B [S100 Calcium Binding Proteins A1 and B]
SERPINB13 [Hurpin, Serine Protease Inhibitor 13]
TIMP3 [TIMP Metallopeptidase Inhibitor 3]
TNXB [Tenascin XB]
DISCUSSION
This pilot study offers correlations on decreased intracellular water, cell deterioration, healthy activities and stress and its results accurately indicate the importance of the epigenetic factors of aging, such as the environmental implications in the lifestyles and the management of behavioral therapies, but only in a small sample of six adult women. A full review of the scientific literature at an international level and the use of a sample representative of gender, age groups, educational levels, racial groups, cultural groups and diverse environmental context across the sexes and age groups, as well as a consultation of web of science databases and scopus would help to better define inclusive health protocols for CSAS. Admittedly, this early study does not represent an exhaustive review of the scientific literature at the international level, nor a complete review of the complementary studies on environmental stress anxiety in aging and its implications with unhealthy environments, including isolation and sedentary lifestyles and from the perspectives of environmental gerontology and epigenetics. The results found, however, offer new thoughts on how CS and its related CSAS might be treated with an inclusive health protocol, which further, international studies may revisit and build on.
As technology increases and the world becomes more connected, it is probable that stress sources will only increase and symptoms in patients will multiply. CS is pervasive, unrelenting and intrusive. Patients must consciously recognize it, turn it off or disconnect and divert energies to mindful relaxation, as CS is unnecessary for survival. Through technological advances, it seems very possible that future therapy for isolation and stress may include the addition of artificial intelligence in the form of robots for companionship. The pharmaceutical industry may also provide a better solution for depression that includes a rapid-acting medical drug intervention. This intervention could be useful to halt the effects of life-changing, severe emotional stress and, in emergency situations, stop thoughts of suicide within minutes. As an aside, it is clear that extrinsic stressors have caused life-altering mental disorders when considering the 24% increase in suicide between 1999 and 2014 and the continually growing rates [51]. We believe that unabated, CSAS not only ages patients, it may put them at increased risk for suicide. Using a comprehensive system that features therapies in line with the cellular water principle theory may help to undo the intrinsic effects of stress, while mental therapies can help patients deal with extrinsic CS and emotional instability. While this study offers compelling pilot data, caution should be taken as it only included six subjects. Larger, more long-term studies are warranted to help physicians treat aging patients struggling with living in today’s stressful world.
REFERENCES
- Cohen S, Williamson GM (1991) Stress and infectious disease in humans. Psychol Bull 109: 5-24.
- Seaward BL (2016) Essentials of managing stress. Jones & Bartlett Publishers, Burlington, Massachusetts, USA.
- McEwen BS (1998) Protective and damaging effects of stress mediators. N Engl J Med 338: 171-179.
- Epel ES, Blackburn EH, Lin J, Dhabhar FS, Adler NE, et al. (2004) Accelerated telomere shortening in response to life stress. Proc Natl Acad Sci USA 101: 17312-17315.
- Herbert TB, Cohen S (1993) Stress and immunity in humans: a meta-analytic review. Psychosom Med 55: 364-379.
- Murad H (2009) Thoughts on the Process of Aging. COSMETIC Cosmetic Dermatology 22.
- Karasek R, Theorell T (1992) Healthy work: stress, productivity, and the reconstruction of working life. Basic books, New York City, New York, USA.
- Boyce WT, Barr RG, Zeltzer LK (1992) Temperament and the psychobiology of childhood stress. Pediatrics 90.
- Murad H (2015) Conquering Cultural Stress: The Ultimate Antiaging Secret. Wisdom Waters Press.
- https://www.atsdr.cdc.gov/substances/index.asp
- Selye H (1973) The Evolution of the Stress Concept: The originator of the concept traces its development from the discovery in 1936 of the alarm reaction to modern therapeutic applications of syntoxic and catatoxic hormones. American scientist 61: 692-699.
- Fox M (2016) One in 6 Americans Take Antidepressants, Other Psychiatric Drugs: study. NBC News, New York City, New York, USA.
- Calderone J (2014) The Rise of All-purpose Antidepressants. Scientific American, USA.
- Selye H (1951) The general-adaptation-syndrome. Annual Review of Medicine 2: 327-342.
- Murad H (2010) The Water Secret: The Cellular Breakthrough to Look and Feel 10 Years Younger. Wiley, New York, USA.
- Slominski A (2007) A nervous breakdown in the skin: stress and the epidermal barrier. J Clin Invest 117: 3166-3169.
- Schmitt J, Romanos M, Pfennig A, Leopold K, Meurer M (2009) Psychiatric comorbidity in adult eczema. Br J Dermatol 161: 878-883.
- Pohlman B, Becker G (2006) “Stress Knocks Hard on Your Immune System”: Asthma and the Discourse on Stress. Med Anthropol 25: 265-295.
- McCubbin HI, Joy CB, Cauble AE, Comeau JK, Patterson JM, et al. (1980) Family stress and coping: A decade review. Journal of Marriage and Family 42: 855-871.
- Murad H, Cultural Stress: A Modern Threat to Health. Corporate Wellness Magazine, Palm Beach, USA.
- Weiss B, Bellinger DC (2006) Social ecology of children's vulnerability to environmental pollutants. Environ Health Perspect 114: 1479-1485.
- https://www.cdc.gov/obesity/data/adult.html
- Ullman K (1999) Doctors Waking Up to Benefits of Sleep Deprivation Treatment for Depression. Web MD, New York City, New York, USA.
- Farag NH, Moore WE, Lovallo WR, Mills PJ, Khandrika S, et al. (2008) Hypothalamic-pituitary-adrenal axis function: relative contributions of perceived stress and obesity in women. J Womens Health (Larchmt) 17: 1647-1655.
- White H, McConnell E, Clipp E, Bynum L, Teague C, et al. (1999) Surfing the net in later life: A review of the literature and pilot study of computer use and quality of life. Journal of Applied Gerontology 18: 358-378.
- Krause N (1991) Stress and isolation from close ties in later life. J Gerontol 46: 183-194.
- Thomée S, Eklöf M, Gustafsson E, Nilsson R, Hagberg M (2007) Prevalence of perceived stress, symptoms of depression and sleep disturbances in relation to information and communication technology (ICT) use among young adults – an explorative prospective study. Computers in Human Behavior 23: 1300-1321.
- Perissinotto CM, Stijacic Cenzer I, Covinsky KE (2012) Loneliness in older Persons: A Predictor of Functional Decline and Death. Arch Intern Med 172: 1078-1083.
- Hawthorne G (2006) Measuring social isolation in older adults: development and initial validation of the friendship scale. Social Indicators Research 77: 521-548.
- Webel AR, Longenecker CT, Gripshover B, Hanson JE, Schmotzer BJ, et al. (2014) Age, stress, and isolation in older adults living with HIV. AIDS Care 26: 523-531.
- Shankar A, McMunn A, Banks J, Steptoe A (2011) Loneliness, social isolation, and behavioral and biological health indicators in older adults. Health Psychol 30: 377-385.
- Bentkover JD, Aldern C, Lerner D, Richardson E, Chadha AB, et al. (2015) Consumer Information and Treatment Resources for Posttraumatic Stress Disorder: Within Reach but Not Grasp. Harv Rev Psychiatry 23: 426-437.
- Ulmer CS, Calhoun PS, Edinger JD, Wagner HR, Beckham JC (2009) Sleep disturbance and baroreceptor sensitivity in women with posttraumatic stress disorder. J Trauma Stress 22: 643-647.
- Owen N, Sparling PB, Healy GN, Dunstan DW, Matthews CE (2010) Sedentary behavior: emerging evidence for a new health risk. Mayo Clin Proc 85: 1138-1141.
- World Health Organization (2002) Physical inactivity a leading cause of disease and disability, warns WHO, World Health Organization, Geneva, Switzerland.
- Soong J (2010) 6 Common Depression Traps to Avoid. WebMD, New York, USA.
- Zs-Nagy I (1997) The membrane hypothesis of aging: its relevance to recent progress in genetic research. J Mol Med (Berl) 75: 703-714.
- Zs-Nagy I (2001) Enzyme activities in the light of the membrane hypothesis of aging: [An answer to K. Kitani, Mech. Ageing Dev. 107 (1999) 299–322]. Mechanisms of Ageing and Development 122: 811-821.
- Zs-Nagy I, The Membrane Hypothesis of Aging (The frustrating decades of biological aging theories and the hopes for the future). International AntiAging Systems.
- Murad H (2008) Sealed for Your Protection. Dermascope, Texas, USA.
- Murad H (2008) Skin Immunity, The Next Generation of Skin. Les Nouvelles Esthetiques & Spa 7: 130-136.
- O'Sullivan RL, Lipper G, Lerner EA (1998) The neuro-immuno-cutaneous-endocrine network: relationship of mind and skin. Arch Dermatol 34: 1431-1435.
- Brazzini B, Ghersetich I, Hercogova J, Lotti T (2003) The neuro-immuno-cutaneous-endocrine network: relationship between mind and skin. Dermatol Ther 16: 123-131.
- Chrousos GP (2000) Stress, chronic inflammation, and emotional and physical well-being: concurrent effects and chronic sequelae. J Allergy Clin Immunol 106: 275-291.
- Murad H (2005) The Cellulite Solution: A Doctor's Program for Losing Lumps, Bumps, Dimples, and Stretch Marks. St. Martin’s Press, UK.
- Di Pasquale MG (2007) Amino Acids and Proteins for the Athlete: The Anabolic Edge, (2ndedn). CRC Press, Boca Raton, Florida, USA.
- Sapolsky RM (2004) Organismal stress and telomeric aging: An unexpected connection. Proc Natl Acad Sci USA 101: 17323-17324.
- Jiang H, Ju Z, Rudolph KL (2007) Telomere shortening and ageing. Z Gerontol Geriatr 40: 314-324.
- Ritz P (2001) Chronic cellular dehydration in the aged patient. J Gerontol A Biol Sci Med Sci 56: 349-352.
- Yamasaki H, Omori Y, Zaidan-Dagli ML, Mironov N, Mesnil M, et al. (1999) Genetic and epigenetic changes of intercellular communication genes during multistage carcinogenesis. Cancer Detect Prev 23: 273-279.
- Vasilogambros M (2016) Rising Suicide Rates. The Atlantic Daily, Washington, D.C., USA.
Citation: Murad H (2017) A Pilot Study on Cultural Stress Anxiety Syndrome, Its Implications on Aging, Gene Expression and Treatment Strategies. J Gerontol Geriatr Med 3: 013.
Copyright: © 2017 Howard Murad MD., FAAD, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.