A Population-Wide Assessment of Decrease in Intracellular Hydration with Age and Certain Health Conditions
*Corresponding Author(s):
Howard MuradMurad Inclusive Health Medical Group, 121 Park Pl 1st Floor, El Segundo, CA 90245, United States
Tel:+1 3109947771,
Email:howardmuradmd@icloud.com
Abstract
Objectives: The membrane hypothesis of aging suggests that age-related changes in the balance of Intracellular Water (ICW) to Extracellular Water (ECW) may play a significant role in the degenerative processes associated with aging. This study presents a comprehensive analysis of changes in cellular water balance related to aging, demographic factors, and various medical conditions.
Methods: This is a meta-analysis study that uses data from three years of the National Health and Nutrition Examination Survey (NHANES) and from a private medical practice, for a total of 11,228 participants between the ages of 18 and 90. The study investigates the relationship between ECW/ICW and factors such as age, gender, race, and health conditions including diabetes, heart disease, and stroke. Fixed-effect generalized linear regression were used to determine significance of factors on ECW/ICW ratio, and Kruskal-Wallis tests were used to assess differences between healthy and unhealthy patients.
Results: The findings reveal a significant increase in ECW/ICW with age, especially in males compared to females. This is true within racial groups for Non-Hispanic Whites, Non-Hispanic Blacks and Mexican Americans. There is also a consistent pattern of ECW/ICW increase in certain medical conditions, including diabetes, congestive heart disease, congestive heart failure, heart attack, stroke and arthritis. However, there was no change in ECW/ICW with the presence of hypertension, high cholesterol, angina pectoris, or osteoporosis.
Conclusion: This investigation provides strong support for the understanding of imbalance of cellular water content with the onset of aging and disease and suggest that increased ECW/ICW may be useful as a diagnostic tool.
Keywords
Aging; Extracellular water; Intracellular water; Membrane hypothesis
Introduction
Health-related and cosmetic changes evident in the aging process, while visibly apparent and extensively analyzed, still present an enigma regarding their underlying physiological mechanisms. These changes encompass a wide range of issues, from subtle cosmetic alterations to more profound health implications, including cancer, cardiovascular diseases, cognitive decline, orthopedic complications and metabolic disorders like diabetes. Given that aging involves a complex interplay of many factors, disentangling the individual contributions of each becomes a formidable task. Nevertheless, unraveling these mechanisms holds substantial medical and socioeconomic significance, particularly for societies witnessing an increasing proportion of older individuals. Central to the discourse on aging is the membrane hypothesis, which posits that changes in cell membrane composition disrupt the balance between Intracellular Water (ICW) and Extracellular Water (ECW) and play a pivotal role in the natural aging trajectory [1]. One of the key aspects of the hypothesis is that there is a relative decrease in ICW compared to ECW as one ages, and this change in water distribution can impact cell function and overall physiological processes. The shift in ECW/ICW balance can affect various cellular functions, such as nutrient transport, waste removal, and cellular signaling, all of which are crucial for maintaining healthy cellular activity. The molecular mechanism by which the membrane hypothesis explains aging remains unknown to date, but we propose that cellular water balance is a reflection of the convergence of all processes related to aging. What is unknown is whether the changes in water balance are a common pathway affected by all forces of aging or the balance change itself is a pathway that acts upon all forces of aging. We believe that both are worthy of more study and the route to supporting either hypothesis begins in the same place with a thorough understanding of how cellular water balance changes with aging. Here we are utilizing the power of two large-scale datasets to aid in that undertaking.
Bioelectrical Impedance Analysis (BIA) is a non-invasive, inexpensive, and rapid method to quantify the amounts of intracellular and extracellular water that make up total body water in human beings. These features make it an efficient research tool to study body water as a function of age and health in large, cross-sectional populations. BIA measures the extent to which water-soluble ions can carry electrical current through the body and can detect ECW/ICW by measuring the impedance to electric current presented by intact, competent fatty membranes around cells [2]. As a result, the relative contributions to the aqueous compartment by all current flowing through cells, and all current flowing outside and around cells, can be distinguished and quantified as part of a three-compartment model of the body. These three compartments, therefore, are 1) fat mass, and 2) fat-free mass represented by total body water, which is further subdivided into 2a) ECW and 2b) ICW.
Changes in ECW/ICW balance may serve as a convergence point for many factors including aging, illness, lifestyle habits, stress and dietary patterns [3]. Several studies have shown that ECW/ICW levels increase with age and that fluid imbalance is present with other medical conditions [4,5]. Elevated ECW/ICW was shown to negatively correlate to muscle strength and positively correlate to frailty and kidney failure [6-9]. Changes in ECW/ICW have been shown to occur during the transition of cells from healthy to cancerous [10]. However, other studies have reported no effect or mixed findings, and few studies have focused on general, population-wide changes [2,11-13]. Overall, the effects of consistent, gradual loss of water throughout a lifetime are not well known, and a comprehensive study that elucidates the intrinsic relationship between ECW/ICW and the natural aging process is needed.
This analysis compiles data from three years of nationally representative health examinations (NHANES, ref. [14-16]) and seven years of data from a private medical-office cohort, representing a cross-sectional sample of over 11,000 participants (Table 1). Together, these data provide great advantages in terms of both statistical robustness and population representation, which will help to detect reliable patterns that are essential for understanding the complex process of aging. This analysis aims to explore the potential changes in ICW level with age while factoring in race, gender, and body composition, and to determine if there is a correlation between change in ICW in individuals that have certain health conditions.
|
Survey |
Total Interviewed |
Total Examined |
Total in Analysis |
Age Range in Analysis |
|
NHANES 1999-2000 |
9,965 |
9,282 |
2,550 |
18-49 |
|
NHANES 2001-2002 |
11,039 |
9,701 |
3,004 |
18-49 |
|
NHANES 2003-2004 |
10,348 |
9,643 |
2,693 |
18-49 |
|
ANON |
3,068 |
3,068 |
2,981 |
18-90 |
|
|
11,228 total participants |
|||
Table 1: Data Summary. Data used in the analysis represents full data subsetted by those in the age range and those who were given a BIA during the NHANES exam.
Methods
- NHANES Sample
The primary data used in this study are from the nationally-representative, cross-sectional NHANES from the years 1999-2000, 2001-2002 and 2003-2004 [14-16]. NHANES is a major program of the National Center for Health Statistics, a unit of the Centers for Disease Control and Prevention, which aims to assess the health and nutritional status of the United States population. The program involves personal interviews, laboratory tests, and physical examinations in participants’ homes and in mobile examination centers. To increase reliability and to ensure an accurate representation of the US population, NHANES employs a multistage probability sampling design wherein some subgroups are oversampled; these include non-Hispanic Black persons, Hispanic persons, low-income white persons, and adults ≤80 years of age.
These years of NHANES data were chosen because they are the most recent surveys to include a Bioelectrical Impedance Analysis (BIA) to detect cell water balance. BIA measures are only recorded for male and female individuals aged 8-49 and excluded females with a positive urine pregnancy test and those who self-reported as pregnant. The relevant measures taken from the BIA include: estimated intracellular and extracellular water volumes, estimated total body water volume, resistance of intracellular and extracellular fluid, and cell membrane capacitance Additionally, for each participant demographic data (age, race/ethnicity, gender, annual household/family income) and body measurements (weight, BMI, estimated fat mass, Fat-Free Mass [FFM]) were collected.
- Independent medical group sample
In addition to the NHANES data, an independent cohort of 3,068 patients of Murad Medical Group, (which later became Murad Inclusive Health Medical Group and is here abbreviated as MMG/MIHMG) was evaluated. This sample was composed of male and female participants ages 10-90 who visited MMG/MIHMG for their personal care between 2004 and 2011 and volunteered to have their body composition data collected and analyzed by means of bioelectrical impedance analysis. Individuals with abnormal heart rhythms or who were (or suspected they might be) pregnant were excluded. Race and ethnicity were not included as variables in this dataset. Each participant was assessed for age, height, weight, resistance, reactance, impedance, target weight, body mass index, basal metabolic rate, daily energy expenditure, phase angle, fat weight, fat-free mass weight, total body water, intracellular water and extracellular water. Body composition was measured using an RJL Systems Bioelectrical Impedance Analyzer, an instrument that measures how an alternating current signal introduced into the body is affected by the body’s composition.
- Relationship between ECW/ICW and age
Data from both the NHANES and MMG/MIHMG group were separately analyzed via fixed-effect generalized linear regression to model the relative impact of the factors age, gender and race on ECW/ICW ratio. Because total body water decreases rapidly from birth through puberty, only data from adult participants (18 and older) were analyzed so as to assess stable values and not artificially inflate any decrease due to age. Models were compared using both likelihood ratio test and Akaike Information Criterion. Age and gender were significant factors, with race affecting the fit only when included by gender. Slope coefficients (β), standard error and significance (p-value) are shown in table 2.
|
Data |
Gender |
Race |
Age Coef Slope, β (SE) |
p-value |
n |
|
NHANES |
Female |
All |
0.0005 (0.0002) |
<0.0047 |
2741 |
|
|
|
Non-Hispanic White |
0.0010 ( 0.0003) |
0.0001 |
1167 |
|
|
|
Non-Hispanic Black |
0.0009 (0.0004) |
0.0138 |
614 |
|
|
|
Mexican American |
-0.0008 (0.0003) |
0.0059 |
716 |
|
|
|
Other Hispanic |
0.0001 (0.0009) |
0.8852 |
148 |
|
|
|
Other/Multiracial |
0.0005 (0.0007) |
0.4674 |
96 |
|
|
Male |
All |
0.0013 (0.0001) |
<0.0001 |
2934 |
|
|
|
Non-Hispanic White |
0.0013 (0.0002) |
<0.0001 |
1221 |
|
|
|
Non-Hispanic Black |
0.0015 (0.0003) |
<0.0001 |
644 |
|
|
|
Mexican American |
0.0010 (0.0002) |
<0.0001 |
796 |
|
|
|
Other Hispanic |
0.0015 (0.0006) |
0.0190 |
136 |
|
|
|
Other/Multiracial |
0.0011 (0.0008) |
0.1658 |
137 |
|
MMG/MIHMG |
Female |
NA |
0.0009 (0.0001) |
<0.0001 |
2320 |
|
|
Male |
NA |
0.0010 (0.0001) |
<0.0001 |
661 |
Table 2: Regression models for ECW/ICW factored by Gender, Age, and Race. Generalized linear regression models, significant factors in bold. Plotted in figure 1.
- Relationship between ECW/ICW and health
To assess a correlation between the health of individuals and their ECW/ICW, additional data was used from NHANES examinations, lab tests, and participant questionnaires. Medical conditions were determined by whether or not the respondent had been told by a doctor or health professional that the condition was present. These included: diabetes, hypertension, high cholesterol, congestive heart failure, coronary heart disease, angina pectoris, myocardial infarction (heart attack), stroke, emphysema, osteoporosis, and arthritis. Individual sample numbers varied for each condition and are shown in table 3. Generalized linear regression was used to model the level of ECW/ICW on the presence of each condition and the other potentially predictive variables: age, gender, race. Models were again compared via LRT and AIC and coefficients, standard error, and significance are in table 3. When the presence of the medical condition was determined to be a significant factor, comparisons were made between the mean ECW/ICW of participants with and without the medical diagnosis stratified by other significant categorical factors if relevant (here, gender proved relevant in all analyses). This was done by Kruskal-Wallis test and means, 95% confidence level, and significance are shown in table 4.
All analyses were performed in R (v4.3.1) using the packages tidyverse (v2.0.0) and janitor (v2.2.0).
|
|
Regression model variables |
|
|||
|
Medical Condition |
Age Variable (β, p-value) |
Gender, ref = Female (β, p-value) |
Medical condition present (β, p-value) |
Race (see text for significance) |
n (without, with condition) |
|
Diabetes |
-0.002, <0.0001 |
0.072, <0.0001 |
-0.046, <0.0001 |
significant |
12529, 199 |
|
Hypertension |
0.0003, 0.0001 |
-0.097, <0.0001 |
0.0003, 0.926 |
significant |
6789, 826 |
|
High cholesterol |
0.001, <0.0001 |
-0.095, <0.0001 |
-0.002, 0.548 |
significant |
1879, 732 |
|
Congestive heart failure |
0.001, <0.0001 |
-0.095, <0.0001 |
0.037, 0.036 |
insufficient |
5059, 22 |
|
Coronary heart disease |
0.001, <0.0001 |
-0.096, <0.0001 |
0.051, 0.004 |
insufficient |
5060, 21 |
|
Angina pectoris |
0.001, <0.0001 |
-0.096, <0.0001 |
0.015, 0.275 |
insufficient |
5052, 33 |
|
Heart attack |
0.001, <0.0001 |
-0.096, <0.0001 |
0.034, 0.031 |
insufficient |
5058, 27 |
|
Stroke |
0.001, <0.0001 |
-0.095, <0.0001 |
0.039, 0.006 |
insufficient |
5048, 33 |
|
Emphysema |
0.001, <0.0001 |
-0.095, <0.0001 |
0.042, 0.046 |
insufficient |
5066, 15 |
|
Osteoporosis |
0.001, <0.0001 |
-0.095, <0.0001 |
0.022, 0.060 |
insufficient |
5032, 49 |
|
Arthritis |
0.001, <0.0001 |
-0.095, <0.0001 |
0.009, 0.0286 |
NA |
4640, 445 |
Table 3: Increased ECW/ICW is directly associated with presence of medical conditions. Based on generalized linear models, significant conditions in bold. Coefficients are only shown if they were present in the best fit model. Specific values for racial comparisons are not shown; some factor combinations resulted in insufficient sample data to draw meaningful conclusions.
|
Medical Condition |
Mean of Condition Present - Mean Condition Absent (95% CI) |
p-value |
|
Diabetes |
Female:-0.004 (-0.014, 0.023) Male: 0.029 (0.0001, 0.057) |
0.537 0.054 |
|
Congestive heart failure |
Female: 0.011 (-0.055, 0.032) Male: 0.071 (0.019, 0.122) |
0.545 0.002 |
|
Coronary heart disease |
Female: 0.058 (-0.153, 0.036) Male: 0.060 (0.006, 0.126) |
0.090 0.037 |
|
Heart attack |
Female: 0.020 (-0.102, 0.060) Male: 0.056 (0.001, 0.110) |
0.874 0.023 |
|
Stroke |
Female: 0.038 (-0.081, 0.083) Male: 0.053 (0.011, 0.119) |
0.076 0.052 |
|
Emphysema |
Female: 0.0625 (0.009, 0.134) Male: 0.037 (-0.099, 0.042) |
0.057 0.091 |
|
Arthritis |
Female: 0.004 (-0.016, 0.007) Male: 0.034 (0.0185, 0.050) |
0.850 <0.0001 |
Table 4: Kruskal-Wallis test for difference in ECW/ICW between unhealthy and healthy NHANES participants. Difference in means for medical conditions that affected ECW/ICW, significant values in bold. Plotted in Figure 3.
Results
- ECW/ICW increases with age
In both the pooled NHANES data and the MMG/MIHMG data there is a significant increase in ECW/ICW with age (Figure 1A and B, respectively). From the NHANES data, female ECW/ICW increased by 0.05% with every year of life and male ECW/ICW increased by 0.13% (Table 2). The MMG/MIHMG data showed a similar pattern for ECW/ICW with female values increasing by 0.09% and male values increasing by 0.10% (Figure 1B). One important note is that the NHANES data has a maximum age of 49 because BIA data are not taken for older individuals, while the MMG/MIHMG data extend to age 90. When the MMG/MIHMG data are restricted to individuals no older than 49, the trajectories are approximately the same, with female ECW/ICW increasing by 0.09% and male ECW/ICW increasing by 0.08% with age. Racial groupings were not available for these data.
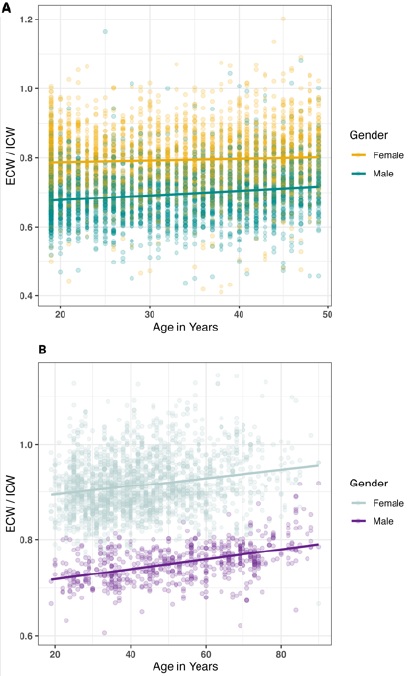 Figure 1: Cell water content levels separated by gender and dataset. Ratio of Intracellular Water (ICW) to Extracellular Water (ECW) separated by gender for pooled NHANES data (A) and for MMG/MIHMG data (B). All lines show significant correlations from linear regression models, see Table 2 for significance and coefficients.
Figure 1: Cell water content levels separated by gender and dataset. Ratio of Intracellular Water (ICW) to Extracellular Water (ECW) separated by gender for pooled NHANES data (A) and for MMG/MIHMG data (B). All lines show significant correlations from linear regression models, see Table 2 for significance and coefficients.
Male ECW/ICW levels were shown to be lower overall compared to female levels but had greater increase over time (p <0.0001). Gender differences in ECW/ICW were driven by decreases in intracellular water over time exceeding decreases in extracellular water. Both decreased with age, but ICW decreased at a faster rate. From the NHANES data, when adjusted by weight, ICW decreased at a rate of 0.10% per year in males and 0.04% in females, compared to a decrease of only 0.02% in ECW in both males and females. In the MMG/MIHMG data, ICW decreased by 0.07% in males and 0.04% in females, while ECW decreased by 0.02% in males and increased by 0.02% in females. Overall, the larger magnitude of the slope in ICW compared to ECW shows that this loss in ICW is the primary component of the increase in ECW/ICW with age. This finding supports the membrane hypothesis of aging.
The pattern of ICW loss with age existed across all racial groups but was only highly significant in some. Both Non-Hispanic White and Non-Hispanic Black males and females showed the greatest loss of ICW over time (Figure 2A). The best fit generalized linear model for these data indicated that age, gender and race were all significant in predicting ECW/ICW increase (Table 2). Between racial groups, ECW/ICW there were differences. No significant effect on ECW/ICW from age was seen for Other Hispanic or Multiracial females and for Other Hispanic males. These groups do have sample sizes comparatively smaller than other racial groups (Table 2), so the presence of the pattern but lack of significance could be due to sampling limitations. The most striking deviance from the pattern of increased ECW/ICW with age is seen in Mexican American females (p = 0.0059). This group shows an overall decrease in ECW/ICW with age, however this appears to be due to this group not being modeled well linearly, unlike the other racial groups (Figure 2B). When the linear models for each subgroup are tested for segmented breaks, it is revealed that an appropriate break occurs at age 37 in Mexican American females, but all other groups are suitably fit to a single model (Chow test: p < 0.00006). When Mexican American women’s data is split into those under 37 and those over 37, their ECW/ICW is also shown to decrease prior to 37 and increase with age afterwards. Other groups do not show a significant difference in their change in ECW/ICW prior to 37.
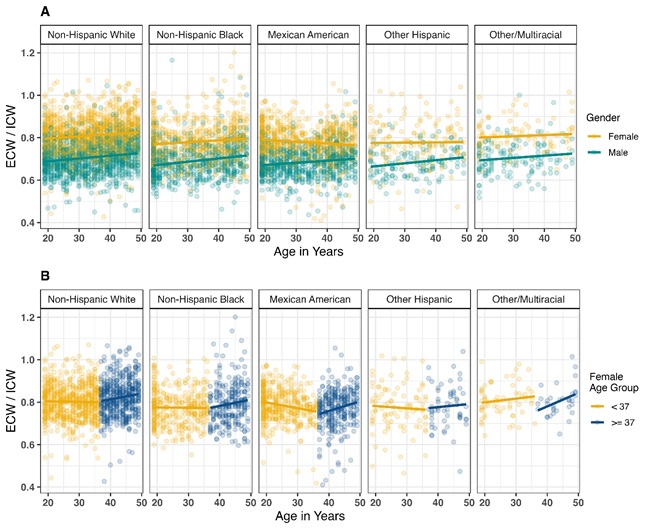 Figure 2: Cell water content levels separated by gender and dataset. A) NHANES data showing the ratio of Intracellular Water (ICW) to Extracellular Water (ECW) separated by gender and race. All lines show significant correlations from linear regression models, see Table 2 for significance and coefficients. B) The same female data as displayed in part A, but modeled with separate linear models before and after age 37. Here, even Mexican American females show an increase in ECW/ICW with advanced age.
Figure 2: Cell water content levels separated by gender and dataset. A) NHANES data showing the ratio of Intracellular Water (ICW) to Extracellular Water (ECW) separated by gender and race. All lines show significant correlations from linear regression models, see Table 2 for significance and coefficients. B) The same female data as displayed in part A, but modeled with separate linear models before and after age 37. Here, even Mexican American females show an increase in ECW/ICW with advanced age.
- ECW/ICW increases with certain medical conditions
To determine whether ECW/ICW level can be used as an overall indicator of health, it was evaluated using generalized linear regression models which included the presence of medical conditions that participants disclosed through NHANES. The medical conditions tested were diabetes, hypertension, high cholesterol, congestive heart failure, coronary heart disease, angina pectoris, myocardial infarction (heart attack), stroke, emphysema, osteoporosis and arthritis. The best fit models (as determined by likelihood ratio and AIC) are presented in table 3 and all include age, gender, and presence of condition. As expected, the coefficient for gender was the greatest, since men have a lower ECW/ICW overall compared to women. The effect from age was similar across all conditions and similar to the overall increase in age for the sample as a whole.
Supporting the hypothesis that cellular water level is affected by patient health, ECW/ICW was shown to be significantly affected by the presence of diabetes, heart attack, heart disease, heart failure, stroke, emphysema and arthritis (Table 4, Figure 3). These effects were primarily only seen in male patients, but for emphysema was also found to be significant in the ECW/ICW ratio of female patients. For all significant differences in ECW/ICW between healthy and unhealthy patients, unhealthy patients had higher ECW/ICW. The differences were fairly dramatic, with the largest being males with coronary heart failure having 7% higher ECW/ICW than healthy males. For many of the medical conditions, there was an insufficient sample size within races to make any meaningful comparisons between them, but for patients diagnosed with diabetes race was somewhat of a factor. Pairwise comparisons between races were mostly not significant, but Mexican Americans did have slightly lower ECW/ICW than Non-Hispanic Whites (mean = -0.006, 95% CI = [-0.012, -0.0002], p = 0.034). This is largely due to the decrease in ECW/ICW in Mexican American females, but they were not significantly different from racial groups other than Non-Hispanic Whites.
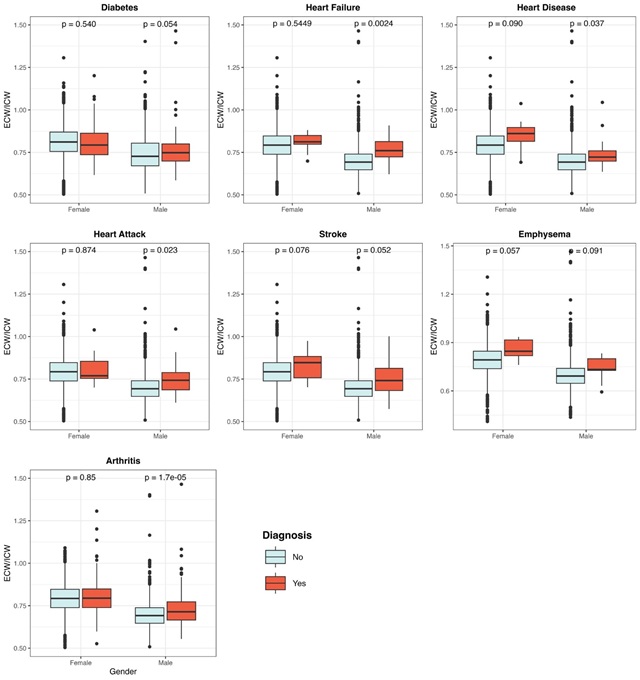 Figure 3: Increased ECW/ICW levels correspond to diagnosis of certain medical conditions. Data represents doctor diagnosis of presence (red/Y) or absence (blue/N) of medical condition. Significant findings from NHANES data models compared using Kruskal-Wallis test. (See Table 3 for means; Table 2 for n-values.)
Figure 3: Increased ECW/ICW levels correspond to diagnosis of certain medical conditions. Data represents doctor diagnosis of presence (red/Y) or absence (blue/N) of medical condition. Significant findings from NHANES data models compared using Kruskal-Wallis test. (See Table 3 for means; Table 2 for n-values.)
Discussion
The membrane hypothesis of aging posits that, over time, changes in the composition of cellular membranes result in a decreased ability to preserve intracellular solute and water content. As this process proceeds, the overall solute density of the cell increases to the point that it impacts the normal functioning of cellular biochemical machinery, resulting in the process we call aging. The observed ICW decline with age in this study, derived from an extensive dataset of 11,228 participants representing a broad spectrum of backgrounds, lends considerable strength to the validation of the membrane hypothesis of aging.
Of particular significance is that this pattern is true even for individuals that have not reached advanced ages. The NHANES data is limited by BIA exams only being performed on patients under 49. Ideally, to see the effects of aging on ECW/ICW, the sample would include the later years of patients’ lives, but the increase is seen even in younger patients and is fairly consistent over lifespan. The MMG/MIHMG data extend the upper bound of age to 90 and show a similar increase to the NHANES data for females (0.09 and 0.05, respectively), and males (0.10 and 0.13, respectively). The MMG/MIHMG data may not represent the general population since these are individuals who have sought out medical consultation and may be more concerned with health overall, as compared to the NHANES patients who are chosen at random. The finding of increasing ECW/ICW with age is consistent with previous large scale studies of Japanese populations [7,9,17] and other studies measuring the impacts of cellular water content and age on body composition and frailty [6,13]. Future research will need to be structured to ensure accurate representation of population subgroups in order to more accurately assess potential variations between groups, but the observed similarities between American and Japanese populations, despite their distinct cultural backgrounds, lend credence to the robustness of these results.
Additionally, for this study, the patterns of decreasing ICW levels with age held constant across all racial groups and genders. ECW/ICW was shown to increase with age for all groups, with the exception of Mexican American females, where a significant decrease was seen with age, and no significant change in ECW/ICW was found for Other Hispanic males and females and Other/Multiracial males. The lack of significance in the “other” racial groups is possibly explained by sample sizes that are approximately 4.5-6 fold less than the next smallest racial group. The pattern of ECW/ICW increase with age is seen in these groups; however, the significance is lacking. We anticipate that with increased sampling these groups would also show significant effects. The case of Mexican American females is more interesting; here, a decrease in ECW/ICW is seen until age 37 at which point ECW/ICW increases in a similar fashion to all other groups. This decrease earlier in life is not seen in other racial groups. Because the NHANES data is limited to ages under 49, it cannot be known from this data if the rate at which Mexican American females increase in ECW/ICW past age 37 is similar to that of other groups, but that approximate age is where many females start to show increases (Figure 2B). These results suggest that the pattern of overall increase in ECW/ICW with advanced age holds true, but that there may be underlying subtleties regarding when this increase begins to occur. ECW/ICW is known to decrease precipitously over the first ten years of life and more research should be conducted to determine at what ages ECW/ICW is perhaps stable and when it begins to increase with advancing age.
The findings here show that many medical conditions, including diabetes, congestive heart failure, coronary heart disease, myocardial infarction (heart attack), stroke, and arthritis are directly associated with increased ECW/ICW level. Notably, the NHANES data only included patients who have self-reported being diagnosed with the medical condition. This would exclude patients who had not been evaluated for these conditions and might represent a bias towards underestimating the impact of these conditions on cellular water levels. The relationship between cellular water content and various medical conditions is an emerging field of study and there is evidence of imbalances being significantly correlated to patient health outcomes. Differences in ECW/ICW levels have been particularly useful as a method of early detection for certain conditions. Namba et al. were able to use elevated ECW/ICW levels as significant predictors of worse outcomes, including higher mortality, in patients with congestive heart failure [11]. Increased ECW/ICW levels were also shown to be a useful diagnostic for determining mortality risk in diabetes patients undergoing hemodialysis [18]. Additionally, elevated ECW/ICW was shown to be independent of other markers of kidney disease and was present even in patients without kidney failure, leading researchers to believe it could be a valuable tool for early detection before the progression of more severe complications [9]. This evidence shows that fluid imbalance should be given more attention in the study of these diseases and as an indicator in the overall health of patients.
The results of this study underscore the significance of including cellular water levels in the investigation of aging and health. The consistency of the observed patterns across different genders and racial groups and their alignment with findings from culturally distinct populations affirm the robustness of these conclusions. To further unravel the dynamics of how cellular water content changes over time and in response to age and various medical conditions, future research should employ longitudinal methodologies, which would enable a deeper exploration of the underlying mechanisms within individuals. This study represents the most comprehensive analysis to date of the variations in ECW/ICW relative to demographic factors and reinforces cellular water content as a valuable area for ongoing research.
Acknowledgments Section
We acknowledge the contributions of Dr. Josie Griffin from Reed College, who provided extensive data analysis support and critically reviewed the manuscript, substantially improving its content.
Declaration of Conflicting Interest
The authors have no conflicting interest to declare.
Funding Statement
NHANES research is funded by the US government. Murad Inclusive Health Medical Group’s data and subsequent analysis were self-funded by Dr. Howard Murad.
Ethical Approval and Informed Consent Statements
All participants signed voluntary consent forms and the data has been de-personalized.
Data Availability Statement
All NHANES datasets analyzed in this study are publicly available at https://wwwn.cdc.gov/nchs/nhanes/. The dataset from the Murad Inclusive Health Medical Group analyzed in this study is available from the corresponding author upon reasonable written request.
References
- Zs-Nagy I (1978) A membrane hypothesis of aging. J Theor Biol 75: 189-195.
- Jaffrin MY, Morel H (2008) Body fluid volumes measurements by impedance: A review of bioimpedance spectroscopy (BIS) and bioimpedance analysis (BIA) methods. Med Eng Phys 30: 1257-1269.
- Chumlea WC, Schubert CM, Sun SS, Demerath E, Towne B, et al. (2007) A review of body water status and the effects of age and body fatness in children and adults. J Nutr Health Aging 11: 111-118.
- Hooper L, Bunn D, Jimoh FO, Fairweather-Tait SJ (2014) Water-loss dehydration and aging. Mech Ageing Dev 136-137: 50-58.
- Hodes RJ (2020) National Institute on Aging, Strategic Directions for Research, 2020-2025. National Institute of Health, Maryland, USA.
- Serra-Prat M, Lorenzo I, Palomera E, Yébenes JC, Campins L, et al. (2019) Intracellular Water Content in Lean Mass is Associated with Muscle Strength, Functional Capacity, and Frailty in Community-Dwelling Elderly Individuals. A Cross-Sectional Study. Nutrients 11: 661.
- Iwasaka C, Yamada Y, Nishida Y, Hara M, Yasukata J, et al. (2023) Association of appendicular extracellular-to-intracellular water ratio with age, muscle strength, and physical activity in 8,018 community-dwelling middle-aged and older adults. Arch Gerontol Geriatr 108: 104931.
- Yamada Y, Buehring B, Krueger D, Anderson RM, Schoeller DA, et al. (2017) Electrical properties assessed by bioelectrical impedance spectroscopy as biomarkers of age-related loss of skeletal muscle quantity and quality. J Gerontol A Biol Sci Med Sci 72: 1180-1186.
- Nakajima H, Hashimoto Y, Kaji A, Sakai R, Takahashi F, et al. (2021) Impact of extracellular-to-intracellular fluid volume ratio on albuminuria in patients with type 2 diabetes: A cross-sectional and longitudinal cohort study. J Diabetes Investig 12: 1202-1211.
- Marques MPM, Batista de Carvalho ALM, Mamede AP, Dopplapudi A, García Sakai V, et al. (2020) Role of intracellular water in the normal-to-cancer transition in human cells-insights from quasi-elastic neutron scattering. Struct Dyn 7: 054701.
- Namba Y, Yunoki K, Nakamura K, Ejiri K, Oka T, et al. (2022) Differences in extracellular fluid volume between acute heart failure patients with and without high systolic blood pressure. ESC Heart Failure 9: 3358-3366.
- Chumlea WC, Guo SS, Zeller CM, Reo NV, Siervogel RM (1999) Total body water data for white adults 18 to 64 years of age: the Fels Longitudinal Study. Kidney Int 56: 244-252.
- Aloia JF, Vaswani A, Flaster E, Ma R (1998) Relationship of body water compartments to age, race, and fat-free mass. J Lab Clin Med 132: 483-490.
- Centers for Disease Control (2001) National Health and Nutrition Examination Survey 1999-2000 Data Documentation, Codebook, and Frequencies. CDC, Georgia, USA.
- Centers for Disease Control (2003) National Health and Nutrition Examination Survey 2001-2002 Data Documentation, Codebook, and Frequencies. CDC, Georgia, USA.
- Centers for Disease Control (2005) National Health and Nutrition Examination Survey 2003-2004 Data Documentation, Codebook, and Frequencies. CDC, Georgia, USA.
- Ohashi Y, Joki N, Yamazaki K, Kawamura T, Tai R, et al. (2018) Changes in the fluid volume balance between intra- and extracellular water in a sample of Japanese adults aged 15-88 yr old: A cross-sectional study. Am J Physiol Renal Physiol 314: 614-622.
- Yajima T, Yajima K (2023) Ratio of extracellular water to intracellular water and simplified creatinine index as predictors of all-cause mortality for patients receiving hemodialysis. PLoS One 18: 0282864.
Citation: Murad H, Carpenter C, Seyfzadeh M (2024) A Population-Wide Assessment of Decrease in Intracellular Hydration with Age and Certain Health Conditions. J Gerontol Geriatr Med 10: 222.
Copyright: © 2024 Howard Murad, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.