Journal of Otolaryngology Head & Neck Surgery Category: Clinical
Type: Review Article
A Rare Cause of Neonatal Respiratory Distress: Congenital Stenosis of Piriform Aperture
*Corresponding Author(s):
Rachida BouatayEnt Department, FattoumaBourguiba Hospital At Monastir, University Of Monastir, Tunisia
Tel:+216 24066013,
Email:rbouattay@yahoo.fr
Received Date: Jun 15, 2019
Accepted Date: Jul 03, 2019
Published Date: Jul 10, 2019
Abstract
Congenital Nasal Pyriform Aperture Stenosis (CNPAS) is a very rare cause of nasal airway obstruction that clinically mimics choanalatresia. CNPAS can be associated with craniofacial anomalies. We report an unusual case of CNPAS associated with solitary median maxillary central incisor that was mis diagnosed as choanalatresia. We highlight, through this case and review of literature, radiologic diagnosis criteria.
Keywords
Neonatal Respiratory Distress; Piriform Aperture
INTRODUCTION
Congenital Nasal Pyriform Aperture Stenosis (CNPAS), is a very rare cause of neonatal upper airway obstruction [1]. Its prevalence remains unknown (a few isolated cases were described in literature). It can be isolated or sometimes associated to other midline defects. The diagnosis is suggested by physical examination and confirmed by Computer Tomography (CT) findings. Therapeutic approach depends on the severity of the stenosis [2].
We report a case of CNPAS to highlight the importance of recognizing the classic signs of CNPAS on cross-sectional imaging to prevent fatal out come and to present our experience in the non-surgical management of this rare anomaly.
We report a case of CNPAS to highlight the importance of recognizing the classic signs of CNPAS on cross-sectional imaging to prevent fatal out come and to present our experience in the non-surgical management of this rare anomaly.
OBSERVATION
We report the case of a full-term female new born, resulting from a pregnancy of normal course with vaginal delivery term at a private hospital. The baby had moderate neonatal respiratory distress worsening every time feeding. The rest of the physical examination did not show any facial dysmorphism. The diagnosis of bilateral choanal atresia was evoked, and the new born was placed on a monitored unit. A CT scan was performed concluding to the diagnosis of choanalatresia. Nasofibrscopy under general anesthesia was realized showing permeable choana. The status was unchanged after 4 days of monitoring with nasogastric tube feeding. Then, the infant was referred to our department. On nasal examination, it was difficult to introduce a nasogastric tube with an anterior block age raising suspicion of CNPAS. A non contrast maxillofacial CT scan showed pyriform aperture stenosis of 4.7mm concluding to the diagnosis of CNPAS with a solitary median maxillary central incisor without other associated intracranial abnormalities (Figure1).
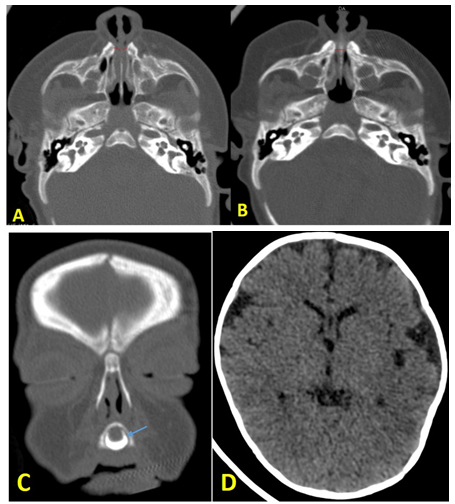
Figure 1: Axial CT scan (A, B) showing the narrowed pyriform aperture measuring 4.7 mm (red arrow) with permeablechoana; C: Coronal CT scan: View of the central mega-incisor (blue arrow); D: Axial parenchymal CT scan showing the absence of other associated cerebral abnormalities.
Decongestive nasal drops with saline solutions and feeding in the upright position were indicated. No surgical intervention was undertaken and the patient was discharged with regular follow up and was asked to report in case there was any symptomatic worsening. Gradual improvement was noted by the parents after 4 months of evolution.
DISCUSSION
Congenital airway obstruction is a problem that affects up to 1 in 5000 infants. The majority of these obstructions result from choanalatresia, which affects 1 in 8000 live births [1]. CNPAS is a rare and unsusal cause of nasal obstruction that occurs around 1 in 25,000 births [3].
CNPAS is characterized by the narrowing of the anterior bony nasal apertures. The exact etiology remains unclear. Chromosomal abnormalities with HPE genes have been reported in some cases [3]. Pyriform aperture stenosis occurs due to embryological malformations of the primary palate, which are associated with a hard triangular-likepalate and the bone over growth of the nasal process of the maxilla [4]. CNPA scan be isolated or often is associated with other malformations mainly the triangular-shape palate and the single central megaincisor, which is found in up to 75% of these patients [4] such as the case of our patient.
In fact, Solitary Median Maxillary Central Incisor (SMMCI syndrome) is a developmental abnormality, including midline structures of the head which involves the brain (holoprosencephaly), cranial bones and maxilla, and nasal airways (choanalatresia or CNPAS) [5,6]. In our case, there was no other abnormality associated.
Clinical presentation can be variable, with respiratory distress at birth, cyanosis relieved by crying, or difficulty in breathing during feeding [6]. These signs may occurs on after delivery or during the first months of life, depending on the grade of the stenosis [7].
The main differential diagnose is choanal atresia that is a congenital narrowing of the posterior nasal airway by a bony or membranous septum [2].The symptoms of choanal atresia vary based on the age of the patient and whether the atresiais unilateral or bilateral. Bilateral choanal atresia presents early in new borns, who are obligate nasal breathers, with either respiratory distress noted around the time of birth or breathing difficulties during the first oral feed [8,9].
Other traumatic causes of neonatal nasal obstruction, Skull base defects such as meningoencephalocele and tumoral processes should be eliminated [1].
The diagnosis is suggested by physical examination due to in ability to pass a nasogastric tube or slim nas endoscope within the first 1cm of the nostrils. The diagnosis is confirmed by CT findings of a whole pyriform aperture width < 8 to11 mm (measured on an axial level of the inferior meatus) in a full-term neonate [2]. CT scan should be performed with thin section (1.5 mm) images obtained by axial sections parallel to the anterior hard palate. Infact, apparent narrowing may be caused by oblique imaging findings [5].
These conditions were not respected in the first CT scan done for our patient conducting to a misdiagnosis of choanal atresia.
Initial treatment is usually conservative such as nasal saline solutions, decongestants or intranasal steroids, at least for 15days. Close follow up until growing expansion of the nasal cavity is essentail. Surgical interventions are reserved for cases with severe stenosis after conservative treatment [4,8].
Timing of surgery and the pyriform aperture width that predicts the need for surgical intervention are still controversial in literature. In fact, many authors reported surgical intervention in cases with sleep apnea, repeat intubation attempts or failure of extubation, feeding problems accompanied by cyanosis, and cases unresponsive to conservative therapy [8,10]. Gonik et al published a review of 16 patients and found that the average size of the pyriform aperture did not correlate with the need for surgery [11].
A systemic review of data available from the literature with statistical analysis showed that a width of 5.7 mm is associated with an 88% chance that the patient will undergosurgery [12].
In our case, No active intervention was undertaken since the evolution was spontaneously favorable after a strict observation of 15 days with conservative treatment.
Surgical procedure consists in pyriform aperture enlargement through an endo-oral sublabial approach with diamond burs. This is a safe approach that provides adequate field exposure, preventing damage to nasolabial soft tissues without visible scarring although that some complications such as injuries to lacrimal system and to the tooth buds has been observed [1,2].
Other authors used boogies for gradual dilatation of nasal without drilling because, in neonates, the nasal bone is soft and can be dilated [5,7]. Stents are retained for only 6-7 days in cases to limit scar related stenosis and recurrence [1].
Dilatation is considered appropriate when a 3.5 mm endotracheal tube can be passed [4]. The evolution is progressively favorable in parallel with the growth of the bones of the nose and the spacing of the two processes which cause the narrowing. A diameter of 5 mm or more at the level of the inferior meatus on a CT scan at birth indicates chances of successful conservative management [1].The prognosisis good if no severe malformations are associated [13].
CNPAS is characterized by the narrowing of the anterior bony nasal apertures. The exact etiology remains unclear. Chromosomal abnormalities with HPE genes have been reported in some cases [3]. Pyriform aperture stenosis occurs due to embryological malformations of the primary palate, which are associated with a hard triangular-likepalate and the bone over growth of the nasal process of the maxilla [4]. CNPA scan be isolated or often is associated with other malformations mainly the triangular-shape palate and the single central megaincisor, which is found in up to 75% of these patients [4] such as the case of our patient.
In fact, Solitary Median Maxillary Central Incisor (SMMCI syndrome) is a developmental abnormality, including midline structures of the head which involves the brain (holoprosencephaly), cranial bones and maxilla, and nasal airways (choanalatresia or CNPAS) [5,6]. In our case, there was no other abnormality associated.
Clinical presentation can be variable, with respiratory distress at birth, cyanosis relieved by crying, or difficulty in breathing during feeding [6]. These signs may occurs on after delivery or during the first months of life, depending on the grade of the stenosis [7].
The main differential diagnose is choanal atresia that is a congenital narrowing of the posterior nasal airway by a bony or membranous septum [2].The symptoms of choanal atresia vary based on the age of the patient and whether the atresiais unilateral or bilateral. Bilateral choanal atresia presents early in new borns, who are obligate nasal breathers, with either respiratory distress noted around the time of birth or breathing difficulties during the first oral feed [8,9].
Other traumatic causes of neonatal nasal obstruction, Skull base defects such as meningoencephalocele and tumoral processes should be eliminated [1].
The diagnosis is suggested by physical examination due to in ability to pass a nasogastric tube or slim nas endoscope within the first 1cm of the nostrils. The diagnosis is confirmed by CT findings of a whole pyriform aperture width < 8 to11 mm (measured on an axial level of the inferior meatus) in a full-term neonate [2]. CT scan should be performed with thin section (1.5 mm) images obtained by axial sections parallel to the anterior hard palate. Infact, apparent narrowing may be caused by oblique imaging findings [5].
These conditions were not respected in the first CT scan done for our patient conducting to a misdiagnosis of choanal atresia.
Initial treatment is usually conservative such as nasal saline solutions, decongestants or intranasal steroids, at least for 15days. Close follow up until growing expansion of the nasal cavity is essentail. Surgical interventions are reserved for cases with severe stenosis after conservative treatment [4,8].
Timing of surgery and the pyriform aperture width that predicts the need for surgical intervention are still controversial in literature. In fact, many authors reported surgical intervention in cases with sleep apnea, repeat intubation attempts or failure of extubation, feeding problems accompanied by cyanosis, and cases unresponsive to conservative therapy [8,10]. Gonik et al published a review of 16 patients and found that the average size of the pyriform aperture did not correlate with the need for surgery [11].
A systemic review of data available from the literature with statistical analysis showed that a width of 5.7 mm is associated with an 88% chance that the patient will undergosurgery [12].
In our case, No active intervention was undertaken since the evolution was spontaneously favorable after a strict observation of 15 days with conservative treatment.
Surgical procedure consists in pyriform aperture enlargement through an endo-oral sublabial approach with diamond burs. This is a safe approach that provides adequate field exposure, preventing damage to nasolabial soft tissues without visible scarring although that some complications such as injuries to lacrimal system and to the tooth buds has been observed [1,2].
Other authors used boogies for gradual dilatation of nasal without drilling because, in neonates, the nasal bone is soft and can be dilated [5,7]. Stents are retained for only 6-7 days in cases to limit scar related stenosis and recurrence [1].
Dilatation is considered appropriate when a 3.5 mm endotracheal tube can be passed [4]. The evolution is progressively favorable in parallel with the growth of the bones of the nose and the spacing of the two processes which cause the narrowing. A diameter of 5 mm or more at the level of the inferior meatus on a CT scan at birth indicates chances of successful conservative management [1].The prognosisis good if no severe malformations are associated [13].
CONCLUSION
CNPAS should be considered in any child with bilateral nasal obstruction even without other major facial anomalies. Key factors in identifying this condition on cross-sectional imaging should be known to confirm the diagnosis. Conservative treatment should be prioritized, but surgical treatment is required in severe cases with persistent respiratory distress.
CONFLICT OF INTEREST
None
REFERENCES
- Rao A, Godehal SM, Patil AR, Mallarajapatna G, Nandikoor S, et al.(2015)Congenital nasal pyriform aperture stenosis: A rare cause of neonatal nasal airway obstruction. BJR Case Rep1:20150006.
- Silva DP, Ribeiro D, Vilarinho S, Dias L (2018) Congenital nasal pyriform aperture stenosis: A rare cause of upperairway obstruction in newborn. BMJ Case Rep 11:227647.
- Yang S, Orta P, Renk E, Inman J (2016) Congenital nasal pyriform aperture stenosis in association with solitary median maxillary central incisor: Unique radiologic features.Radiology Case Reports 11 : 178-181.
- Fonseca EK, Murakoshi RW, Loureiro RM, Sumi DV, Soares CR, et al. (2019)Einstein (São Paulo). 17:1-2.
- Amini E, Rabbani M, Jafarpishe MS, Nazem M (2016) Congenital nasal pyriform aperture stenosis: A case with accompanying short lingual frenulum. Adv Biomed Res 5:135.
- Thomas E, Gibikote S, Panwar J, MathewJ (2010) Congenital nasal pyriform aperture stenosis: A rare cause of nasal airway obstruction in a neonate. Indian Journal of Radiology and Imaging 20: 266.
- Serrano T, Pfeilsticker L, Silva V, Hazboun I, Paschoal J, et al. (2016)Newborn nasal obstruction due to congenital nasal pyriform aperture stenosis. Spring7: 37-41.
- Iziki O, et al. (2019) An unusual cause of upperairway obstruction in newborn: Congenitalnasal pyriform aperture stenosis. Otolaryngol Open Access J 4: 000179.
- RajanR, Tunkel DE (2018) Choanalatresiaand otherneonatal nasal anomalies. Clinics in Perinatology 45 : 751-767.
- Ilhan O, Pekcevik Y, Akbay S, Ozdemir SA, Memur S,et al. (2018)Solitarymedianmaxillary central incisor, holoprosencephaly and congenital nasal pyriform aperture stenosis in a premature infant: Case report. Arch Argent Pediatr 116:130-134.
- Gonik NJ, Cheng J, Lesser M, Shikowitz MJ, Smith LP (2015) Int J PediatrInt J Pediatr Otorhinolaryngology 235-239.
- Wormald R, et al. (2015) International journal of pediatric otorhinolaryngology 79:1802-1805.
- Brown OE, Myer CM, Manning SC (1989) Congenital nasal pyriform aperture stenosis. Laryngoscope: 99: 86-91.
Citation: Bouatay R, Achour A, Harrathi K, Koubaa J(2019) A Rare Cause of Neonatal Respiratory Distress: Congenital Stenosis. J Otolaryng Head Neck Surg 5: 032
Copyright: © 2019 Rachida Bouatay, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Journal Highlights
© 2026, Copyrights Herald Scholarly Open Access. All Rights Reserved!