Journal of Reproductive Medicine Gynaecology & Obstetrics Category: Medical
Type: Case Report
A Successful Pregnancy Outcome in a Complete Septate Uterus
*Corresponding Author(s):
Catalina Renata Elizalde Martinez-PeñuelaDepartment Of Gynecology, Hospital Virgen Del Camino, Irunlarrea St 31008. Pamplona, Spain
Tel:+34 660825639,
Email:renata.elizalde.martinezpenuela@navarra.es
Received Date: Jul 15, 2017
Accepted Date: Aug 01, 2019
Published Date: Aug 08, 2019
Abstract
The incidence of congenital uterine malformation is estimated to be 3-5% in general population. Abnormal fusion of Mullerian duct in embryonic life results in variety of malformations. Here, we report a case of successful pregnancy outcome in a complete septate uterus with pregnancy in the right horn. An emergency lower segment caesarean was performed instead of delivery because of a non reassuring foetal heart rate. The diagnosis was confirmed intra operatively. A septoplasty prior to a new gestation was performed.
Keywords
MRI; Mullarian ducts; Preterm labour; Septate uterus; Ultrasound
INTRODUCTION
Uterine anomalies can lead to infertility and problems with reproduction among women. A lot of uterine malformation like septate uterus, unicornuate uterus and bicornuate uterus result from abnormal development of paramesonephric (mullarian) duct fusion during uterus development. The prevalence of uterine anomalies in the general population is about 0.5% [1]. Acien, in a review study, found a mean incidence for septate uterus 22% (complete septate 9%, partial septate 13%) among the all other types of mullarian defects [2]. In 1988 American Fertility society described congenital uterine anomalies relateted to mullarian ducts according to figure1. Septate uterus is the most frequent uterine malformation [3,4] and characterized by a muscular or fibrous wall, called the septum. The septum affects only the cranial part of the uterus (partial septate uterus) or it may reach as far as the cervix (complete septate uterus) figure1. It is diagnosed by medical image techniques, i.e., ultrasound or an MRI.
 Figure 1: Classification of congenital uterine anomalies as described by the American Fertility Society (1988).
Figure 1: Classification of congenital uterine anomalies as described by the American Fertility Society (1988).CASE REPORT
A 26 yr old 2nd gravida, presented to the OBG dept of Navarra with 2months amenorrhoea. She had a first trimester abortion in first pregnancy. She had no complaints, but an early ultrasound done at 7 wks of gestational age detected a complete septate uterus with pregnancy in the right horn (Figure 2). Per speculum examination showed one cérvix and vulva, urethra and vagina were normal. She had regular antenatal visits which are uneventful till 8 month. At 32 wks of gestation she was admitted with complain of abdominal pain. Tocolysis given and patient steroided for lung maturity. USG done revealed cervical shortening. Doppler was normal. Tocolysis stopped 48 hrs after giving corticosteroids.
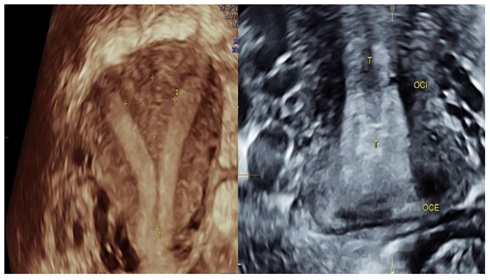
Figure 2: Three dimensional ultrasound: complete uterine sept.
At 34 wks of gestation the patient presented with prelabour premature rupture of membranes. In view of non-reassuring foetal heart rate, an emergency lower segment caesarean section was done with the following intra operative findings: A complete uterine septus with pregnancy in the right horn seen. A live male child in right occipito posterior position weighing 1.7 kg was delivered. Placenta is located anteriorly in the upper segment. By exteriorizing the uterus, findings are confirmed. She had uneventful post operative period and was discharged on 8th post operative day.
One year later, she cames to the hospital for gestational desire and after the hysterosalpingography (Figure 3) we recommend the possibility of performing a septoplasty prior to a new gestation (Figure 4). 6 months later she got pregnant and had a eutocic deivery without any problem during pregnancy.
 Figure 3: Hysterosalpingography.
Figure 3: Hysterosalpingography.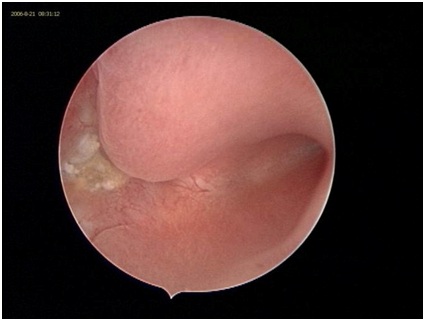 Figure 4: Histeroscopy after septoplasty.
Figure 4: Histeroscopy after septoplasty.DISCUSSION
Uterine anomalies are related to an increased risk of infertility, miscarriage, premature birth, fetal loss and cesarean delivery [5,6]. In present case, according to the patient history, septate uterus has influenced her fertility and there was a previous history of abortion. Other than a miscarriage or recurrent miscarriage, there aren’t any symptoms of a septate uterus. It’s often only diagnosed after an investigation into the cause of miscarriages. Sometimes it can be picked up during a routine pelvic exam if the septum extends beyond the uterus to include the cervix and vagina as well.
Most of the uterine septi are diagnosed by fertility subspecialists, after the patient presents with recurrent pregnancy loss. It is important that fertility specialists make the correct diagnosis of the uterine septum versus a bicornuate uterus. The uterine septum contains a separation in the uterine cavity, however the outer appearance of the uterus is normal. A bicornuate uterus at the other hand has a completely separated upper end both internally and externally. Diagnosing this properly is very important since an attempted resection of the bicornuate uterus, that is improperly diagnosed as a uterine septum might create a uterine perforation.
Ultrasonography is a simple, quick, and non invasive technique for detecting and diagnosing uterine anomalies. Despite the notable advantages of this technique, unfortunately the obstetric ultrasound scan done on our patient in her first pregnancy could not detect the septate uterus as anomalies accordance with uterus exactly and it could be probably as a result of lack of experience and poor ultrasound quality. However, our MRI images diagnosed this problem accuracy. Grimbizis et al., reported that 12 (26.1%) out of their 46 infertile patients with septate uterus had laparascopic finding of endometriosis [7]. Fayez also found endometriosis in three (43%) out of seven similar patients [3]. It seems possible that septate uterus may be involved in the pathogenesis of endometriosis and thereby plays an important role in indirect relationship within fertility. Therefore, it seems that any finding about endometriosis should be followed by careful investigation for uterine malformation especially in women affected by septate uterus.
Hysteroscopy remains the standard for evaluation of intracavitary abnormalities. Its use is especially practical, as it offers the opportunity for treatment at the time of diagnosis. The septum incision is performed with a hysteroscopic resectoscope and it may be controlled under laparoscopic supervisión.
Hysteroscopy without damaging the intact hymen is feasible and helpful for the diagnosis in the treatment of pathologic endometrial changes in women [8,9]. Although hysteroscopy is now the preferred method for treatment of the septate uterus, a report of two cases described successful removal of the septum at the time of cesarean section. The difficulty in achieving complete uterine septum caesarean has been reported [10,11], however in the in present case we didn’t found any trouble.
Most of the uterine septi are diagnosed by fertility subspecialists, after the patient presents with recurrent pregnancy loss. It is important that fertility specialists make the correct diagnosis of the uterine septum versus a bicornuate uterus. The uterine septum contains a separation in the uterine cavity, however the outer appearance of the uterus is normal. A bicornuate uterus at the other hand has a completely separated upper end both internally and externally. Diagnosing this properly is very important since an attempted resection of the bicornuate uterus, that is improperly diagnosed as a uterine septum might create a uterine perforation.
Ultrasonography is a simple, quick, and non invasive technique for detecting and diagnosing uterine anomalies. Despite the notable advantages of this technique, unfortunately the obstetric ultrasound scan done on our patient in her first pregnancy could not detect the septate uterus as anomalies accordance with uterus exactly and it could be probably as a result of lack of experience and poor ultrasound quality. However, our MRI images diagnosed this problem accuracy. Grimbizis et al., reported that 12 (26.1%) out of their 46 infertile patients with septate uterus had laparascopic finding of endometriosis [7]. Fayez also found endometriosis in three (43%) out of seven similar patients [3]. It seems possible that septate uterus may be involved in the pathogenesis of endometriosis and thereby plays an important role in indirect relationship within fertility. Therefore, it seems that any finding about endometriosis should be followed by careful investigation for uterine malformation especially in women affected by septate uterus.
Hysteroscopy remains the standard for evaluation of intracavitary abnormalities. Its use is especially practical, as it offers the opportunity for treatment at the time of diagnosis. The septum incision is performed with a hysteroscopic resectoscope and it may be controlled under laparoscopic supervisión.
Hysteroscopy without damaging the intact hymen is feasible and helpful for the diagnosis in the treatment of pathologic endometrial changes in women [8,9]. Although hysteroscopy is now the preferred method for treatment of the septate uterus, a report of two cases described successful removal of the septum at the time of cesarean section. The difficulty in achieving complete uterine septum caesarean has been reported [10,11], however in the in present case we didn’t found any trouble.
CONCLUSION
The reported prevalence of the septate uterus in different populations, including women with normal fertility, infertility, and repeated pregnancy loss, varies widely, partly because the methods used for diagnosis differ between investigators. The pooled data suggest that the prevalence in women with normal fertility and infertility is similar (approximately 1%). The prevalence in women with repeated pregnancy loss is significantly higher (mean, 3.3%) [4].
Early diagnosis and proper antenatal care is required to successfully manage a pregnancy with bicornuate uterus. Patient with mullerian duct anamolies are known to have a higher incidence of infertility, repeated first, second trimester spontaneous abortions intrauterine growth retardation, fetal malpositions, preterm labor, prelabour preterm rupture of membranes & retained placenta. Anticipation and preparedness to deal with these known complications will ensure positive outcome for the mother and baby.
The finding of a septate uterus perse is not an indication for surgical intervention because it is not always associated with poor obstetric performance. However, when a septate uterus is found in association with adverse reproductive outcome, surgical intervention ought to be considered [4]. Hysteroscopic septal incision is the best method for the preservation of the hymen and it can be performed using the microscissors, electrosurgery, or fiber optic light laser energy.
In conclusion, the diagnosis of septate uterus as a congenital anomaly can be achieved easily with MRI. It can be corrected by hysteroscopic surgery and thereby decreases the rate of abortion for women greatly.
Early diagnosis and proper antenatal care is required to successfully manage a pregnancy with bicornuate uterus. Patient with mullerian duct anamolies are known to have a higher incidence of infertility, repeated first, second trimester spontaneous abortions intrauterine growth retardation, fetal malpositions, preterm labor, prelabour preterm rupture of membranes & retained placenta. Anticipation and preparedness to deal with these known complications will ensure positive outcome for the mother and baby.
The finding of a septate uterus perse is not an indication for surgical intervention because it is not always associated with poor obstetric performance. However, when a septate uterus is found in association with adverse reproductive outcome, surgical intervention ought to be considered [4]. Hysteroscopic septal incision is the best method for the preservation of the hymen and it can be performed using the microscissors, electrosurgery, or fiber optic light laser energy.
In conclusion, the diagnosis of septate uterus as a congenital anomaly can be achieved easily with MRI. It can be corrected by hysteroscopic surgery and thereby decreases the rate of abortion for women greatly.
REFERENCES
- Nahum GG (1998) Uterine anomalies. How common are they, and what is their distribution among subtypes? J Reprod Med 43: 877-887.
- Acién P (1997) Incidence of Müllerian defects in fertile and infertile women. Hum Reprod 12: 1372-1376.
- Fayez JA (1986) Comparison between abdominal and hysteroscopic metroplasty. Obstet Gynecol 68: 399-403.
- Raga F, Bauset C, Remohi J, Bonilla-Musoles F, Simón C, et al. (1997) Reproductive impact of congenital Müllerian anomalies. Hum Reprod 12: 2277-2281.
- Rock JA, Schlaff WD (1985) The obstetric consequences of uterovaginal anomalies. Fertil Steril 43: 681-692.
- Ludmir J, Samuels P, Brooks S, Mennuti MT (1990) Pregnancy outcome of patients with uncorrected uterine anomalies managed in a high-risk obstetric setting. Obstet Gynecol 75: 906-910.
- Grimbizis G, Camus M, Clasen K, Tournaye H, De Munck L, et al. (1998) Hysteroscopic septum resection in patients with recurrent abortions or infertility. Hum Reprod 13: 1188-1193.
- Xu D, Xue M, Cheng C, Wan Y (2006) Hysteroscopy for the diagnosis and treatment of pathologic changes in the uterine cavity in women with an intact hymen. J Minim Invasive Gynecol 13: 222-224.
- Cheong ML (2010) Minihysteroscopy for examination and management of pathologic lesions of virginal reproductive tracts: Can we preserve the hymen intact? Arch Gynecol Obstet 281: 375-376.
- Lipitz S, Shalev J, Kokia E, Kushnir O, Serr DM, et al. (1990) Successful outcome of pregnancy following complete removal of uterine septum during cesarean section. Gynecol Obstet Invest 29: 78-80.
- Green LK, Harris RE (1976) Uterine anomalies. Frequency of diagnosis and associated obstetric complications. Obstet Gynecol 47: 427-429.
Citation: Martinez-Peñuela CRE, Zabaleta J, Campo G, Elizalde FJ, Pérez B (2019) A Successful Pregnancy Outcome in a Complete Septate Uterus. J Reprod Med Gynecol Obstet 4: 025.
Copyright: © 2019 Catalina Renata Elizalde Martinez-Peñuela, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Journal Highlights
© 2026, Copyrights Herald Scholarly Open Access. All Rights Reserved!