Abortion-Related Admissions to the Komfo Anokye Teaching Hospital in Kumasi, Ghana; A 4-Year Review
*Corresponding Author(s):
Compton SDDepartment Of Obstetrics And Gynecology, University Of Michigan, Michigan, United States
Email:sarahrom@umich.edu
Abstract
Introduction: Over 5 million women are admitted to hospitals every year in low-income countries due to unsafe abortion, and the annual cost of treating major complications from unsafe abortion is estimated at US$ 553 million, straining already under-resourced health systems. Abortion-related complications have been dropping in sub-Saharan Africa. This study assessed whether emergency admissions due to abortion complications are reducing at one hospital in urban Ghana.
Methods: In this retrospective, institution-based cross-sectional study in the emergency gynecology ward at the Komfo Anokye Teaching Hospital (KATH), in Kumasi, Ghana data on date of admission, age of patient, and diagnosis were extracted from logbooks from June 1, 2013 to September 30, 2017. Authors reviewed and coded all diagnoses and created a variable for abortion from women within the reproductive age group (15-49 years of age). Dates were split into quarters, and the proportion of admissions due to abortion was determined.
Results: Abortion-related admissions comprised 43.2% of all admissions in the second quarter of our analysis (June-August 2013), and this dropped to 21.4% by the end of our investigation (September 2017). There was a steady decline in abortion-related admissions to this ward over the 4 years of study.
Discussion: There was a dramatic reduction in abortion-related admissions to the KATH emergency gynecology ward during the study period. These findings confirm other work a reduction in unsafe abortion in sub-Saharan Africa. Future work is necessary to determine if this is due to safer forms of abortion or due to a reduction in unplanned pregnancies.
Keywords
Abortion; Emergency gynecology; Ghana
Highlights
- Abortion-related admissions to a teaching hospital fell from 2013 to 2017
- One-fifth of all admissions are due to abortion-related complications
- Ghanaian women need access to legal, safe abortion services
Background
Complications arising after unsafe abortion continues to be a significant cause of maternal death and a major public health challenge, especially in low-resource settings. Around 25 million unsafe abortions are estimated to take place worldwide each year, and 8 million are carried out in the least- safe conditions [1]. In Africa, from 2010 to 2014, an estimated 6.8 million abortions took place each year, nearly all of which were either “less safe” (2.2 million), or “least-safe” (3.9 million) [1]. Only 0.7 million abortions were classified as “safe”, risking the lives and health of African women. Over 5 million women are admitted to hospitals every year in low-income countries as a result of unsafe abortion [2], and the annual cost of treating major complications from unsafe abortion is estimated at US$ 553 million, straining already under-resourced health systems. Substantial proportions of abortion-related hospital admissions have potentially life-threatening complications [3] putting women at risk for life-long morbidity.
Despite a liberal abortion law [4], unsafe abortion remains common in Ghana, and abortion-related complications remain a leading cause of maternal mortality [5]. In 2009, abortion-related complications accounted for 42.7% of admissions to the gynecological ward at the teaching hospital in Kumasi, Ghana [6], despite the Ghana Health Service publishing guidelines to provide safe abortion services in all facilities in 2006 [7]. Beginning in 2000, when medication abortion was developed, and with ubiquitous access to the drugs, the proportion of abortions undertaken in a safe manner has increased, and morbidity and mortality related to abortion have improved [8]. In recent years, the World Health Organization has updated its guidance about what constitutes a safe abortion, most notably regarding the role of non-physician providers [9] and medication abortion [10]. There is emerging evidence that medication abortion is safe and effective, even when used by a woman not under the guidance of a healthcare provider [11,12]. When administered correctly, less than 0.2% of women experience serious complications from medication abortion [13]. With the wide availability of misoprostol, abortion-related complications might be fewer, and, when they do occur, less serious. The objective of this study is to describe trends in emergency admissions to one large teaching hospital due to complications from abortion from 2013 to 2017.
Methods
We undertook a retrospective, institution-based cross-sectional study in the emergency gynecology ward at the Komfo Anokye Teaching Hospital (KATH), in Kumasi, Ghana. Kumasi is the capital of the Ashanti Region, the most densely populated region of Ghana, with about 6 million inhabitants [14] (Ghana Administrative Records), 20% of the country’s total. A structured data extraction sheet was used to collect data from log books in the emergency gynecology ward. The study team trained the three data extractors who collected data on date of admission, age of patient and diagnosis from logbooks from June 1, 2013 to September 30, 2017, and entered them into an excel spreadsheet. Authors reviewed and coded all diagnoses, creating a variable for abortion. We restricted analysis to women within the reproductive age group (15-49 years of age), as we determined those are the women at risk of unsafe abortion. Dates were split into quarters, and the proportion of admissions due to abortion was calculated by dividing the total number of admissions each quarter by the number of abortion-related admissions in that quarter.
Logistic regression was used to test for association between age and abortion-related admission. Ethical clearance was obtained from the University of Michigan Institutional Review Board and the Komfo Anokye Teaching Hospital’s Committee on Human Research, Publications and Ethics.
Results
A total of 6,836 records that met the inclusion criteria (being between the ages of 15 and 49 years) are included in this analysis (out of 7,654 total admissions over the study period). For the youngest age group, abortion-related conditions accounted for 35.0% of admissions. This rose for those aged 20-24 (36.1%), and then declined for each subsequent age group (32.8% for ages 25-29 years; 32.2% for ages 30-39 years; 20.9% for ages 40-49 years) across the study timeframe. In logistic regression, age was associated with abortion-related admissions with the age group 20-24 being 1.2 times as likely as having an abortion-related admission (OR=1.19, 95% CI: 1.04- 1.37, p=.014), and those in the oldest age group being almost half as likely as having an abortion-related admission (OR=.557, 95% CI: .465-.668, p < .001).
At the beginning of our analysis, abortion-related admissions represented 39.6% of all emergency gynecology ward admissions for women in the reproductive age group, and this increased to 43.2% of all admissions in the second quarter of our analysis (June-August 2013). By the end of this analysis (September 2017), the proportion of admissions resulting from abortion had dropped to 21.4% (Figure 1). There was a fairly steady decline in abortion-related admissions to this ward over the 4 years of study. Due to a missing logbook, we do not have data from quarters 7 and 8.
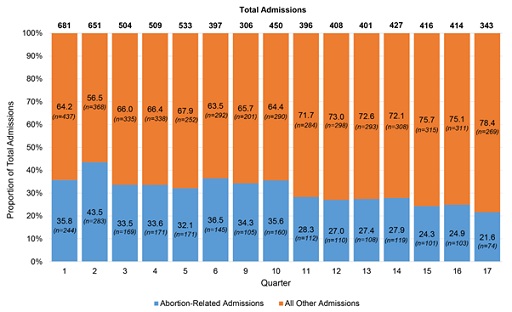 Figure 1: Proportion of admissions to the KATH emergency gynecology ward due to abortion.
Figure 1: Proportion of admissions to the KATH emergency gynecology ward due to abortion.
Discussion
In this study, we documented a dramatic reduction in abortion-related admissions to the emergency gynecology ward of a large teaching hospital in Kumasi, Ghana between March 2013 and September 2017. In Ghana, the majority of abortions are conducted by the woman herself [15]. It would appear from our analysis that there is potentially a shift from less safe to safer options for self-induction of abortion, given the relatively fewer admissions to the gynecology ward that are due to complications from unsafe abortion over the 4 years from 2013 to 2017.
Unfortunately, due to data limitations, we are not able to conduct more than descriptive analysis. However, this paper contributes to the literature by confirming the anecdotal reports of clinicians in this environment that post-abortion complications are reducing as a cause of admission to the emergency gynecology ward in this hospital. Although not directly observable due to data limitations, our findings bolster other work supporting the idea that women may be using medication abortion to self-manage abortions more safely [16]. Medication abortion has been documented in recent investigations as the most common means of abortion in urban Ghana [17,18], especially among young people [16]. Future work is necessary to determine if this reduction is due to the wide availability of misoprostol in this community or due to a reduction in unplanned pregnancies.
Even with the decreasing burden of admissions due to abortion, the fact that over one-fifth of admissions are related to post-abortion complications in a setting where safe abortion is ostensibly legally available in all public facilities, as well as by many private providers, is troubling. While progress has undoubtedly been made to improve access to safe abortion services, unsafe abortion is preventable, and until women have full access to safe methods, preventable hospitalizations and deaths will continue to occur.
Conflicts of Interest
The authors have no conflicts of interest.
References
- Ganatra B, Gerdts C, Rossier C, Johnson BR Jr, Tunçalp Ö, et al. (2017) Global, regional, and subregional classification of abortions by safety, 2010-14: Estimates from a Bayesian hierarchical model. Lancet 390: 2372-2381.
- Singh S (2006) Hospital admissions resulting from unsafe abortion: estimates from 13 developing countries. Lancet 368: 1887-1892.
- Calvert C, Owolabi OO, Yeung F, Pittrof R, Ganatra B, et al (2018) The magnitude and severity of abortion-related morbidity in settings with limited access to abortion services: A systematic review and meta-regression. BMJ global health (Vol-3).
- Aniteye P, Mayhew SH (2013) Shaping legal abortion provision in Ghana: Using policy theory to understand provider-related obstacles to policy implementation. Health Research Policy and Systems 11: 23.
- Asamoah BO, Moussa KM, Stafström M, Musinguzi G (2011) Distribution of causes of maternal mortality among different socio-demographic groups in Ghana; A descriptive study. BMC Public Health 11: 159.
- Konney TO, Danso KA, Odoi AT, Opare-Addo HS, Morhe ES (2009) Attitude of women with abortion-related complications toward provision of safe abortion services in Ghana. J Womens Health (Larchmt) 18: 1863-1866.
- Sedgh G (2010) Abortion in Ghana. Issues Brief (Alan Guttmacher Inst): 1-4.
- Singh S, Remez L, Sedgh G, Kwok L, Onda T (2018) Abortion worldwide 2017: Uneven progress and unequal access. Guttmacher Institute, USA.
- Ganatra B, Tunçalp Ö, Johnston HB, Johnson BR Jr, Gülmezoglu AM, et al. (2014) From concept to measurement: Operationalizing WHO's definition of unsafe abortion. Bull World Health Organ 92: 155.
- Harper CC, Blanchard K, Grossman D, Henderson JT, Darney PD (2007) Reducing maternal mortality due to elective abortion: Potential impact of misoprostol in low-resource settings. Int J Gynaecol Obstet 98: 66-69.
- Shannon C, Winikoff B (2008) How much supervision is necessary for women taking mifepristone and misoprostol for early medical abortion? Womens Health (Lond) 4: 107-111.
- Footman K, Keenan K, Reiss K, Reichwein B, Biswas P, et al. (2018) Medical Abortion Provision by Pharmacies and Drug Sellers in Low- and Middle-Income Countries: A Systematic Review. Stud Fam Plann 49: 57-70.
- WHO (2018) Newsroom. WHO, Geneva, Switzerland.
- Ghana Administrative Regions (2020).
- Ganle JK, Obeng B, Yeboah JY, Tagoe-Darko E, Mensah CM (2016) Disparities in abortion experience and access to safe abortion services in Ghana: Evidence from a retrospective survey. Afr J Reprod Health 20: 43-52.
- Moseson H, Herold S, Filippa S, Barr-Walker J, Baum SE, et al. (2020) Self-managed abortion: A systematic scoping review. Best Pract Res Clin Obstet Gynaecol 63: 87-110.
- Appiah-Agyekum NN, Sorkpor C, Ofori-Mensah S (2015) Determinants of abortion decisions among Ghanaian university students. Int J Adolesc Med Health 27: 79-84.
- Appiah-Agyekum NN (2018) Medical abortions among university students in Ghana: Implications for reproductive health education and management. Int J Womens Health 10: 515-522.
Citation: Compton SD, Ogu K, Dassah ET (2023) Abortion-Related Admissions to the Komfo Anokye Teaching Hospital in Kumasi, Ghana; A 4-Year Review. J Reprod Med Gynecol Obstet 8: 122.
Copyright: © 2023 Compton SD, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.