Acute Appendicitis Presenting as Urinary Retention in a Pediatric Patient
*Corresponding Author(s):
Rose AyoobDivision Of Nephrology, Department Of Pediatrics, West Virginia University, Charleston, WV, United States
Tel:+1 3043881565,
Email:rose.ayoob@hsc.wvu.edu
CASE
We present a unique case of a two-year-old male patient who presented to our Emergency Department (ED) multiple times with acute urinary retention. On his first ED visit, he had chief complaints of fever associated withvomiting, diarrhea and inability to urinate for one day. Patient was vitally stable on arrival and examination was within normal limits. Workup at that time was remarkable for leukocytosis of 21,000 and C Reactive Protein (CRP) of 38.9. Basic Metabolic Panel (BMP) was normal. Urinalysis (UA) showed 4 white cells but negative leucocyte esterase or nitrites. Patient was diagnosed with acute gastroenteritis. He received a normal saline bolus of 20 cc/kg, one dose of Ondansetron for vomiting and waslater discharged home.
Patient was seen in our outpatient pediatric clinic next day with chief complaint of inability to urinate. His vomiting, diarrhea and fevers improved overnight. On that visit, patient was vitally stable and examination was within normal limits except for palpable distended bladder. Workup showed down trending white cell count of 19,200 and CRP of 25.1. BMP was within normal limits. UA showed pyuria with 7 WBCs, 3 RBCs but negative leucocyte esterase and nitrites. Urine culture was obtained as well. Patient was catheterized in clinic where he produced approximately 140 ml of urine. On repeat examination, abdomen was soft and non-distended. He was discharged home with instructions to seek emergent care if it recurs.
Patient presented to ED again one day later, again with chief complaints of inability to urinate and intermittent low-grade fevers.Examination showed mild suprapubic tenderness and distended bladder. Initial workup showed leukocytosis of 20900, with CRP of 12.2 and negative procalcitonin of
Patient continued to spike high fevers. He was noticed to have frank abdominal distention next morning with rigidity and guarding. X-ray abdomen was repeated which showed worsening gaseous abdominal distention. Nasogastric (NG) tube was placed for decompression.
Urology and surgery teams were consulted and oxybutynin was stopped. CT abdomen and pelvis with PO/IV contrast was obtained (Figure 1) that showed “Acute, complicated appendicitis with abscess formation in the deep pelvis measuring 3.1 x 2.0 x 1.8 cm with additional fluid in the anterior pelvis as well as along the right paracolic gutter presumably representing reactive ascites vs extensive abscess formation. Also dilated small bowel in the upper abdomen with early small bowel obstruction.’’ Ceftriaxone was discontinued and Piperacillin-Tazobactam was added for coverage of gram-negativegut bacteria.
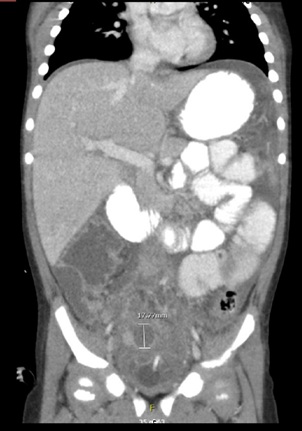 Figure 1: Patient CT of abdomen/pelvis with PO/IV contrast showing inflamed appendix and periappendiceal abscess formation.
Figure 1: Patient CT of abdomen/pelvis with PO/IV contrast showing inflamed appendix and periappendiceal abscess formation.
Patient was later taken to operation theatre for laparoscopic appendectomy and abdominal wash out by the surgery team. After return from surgery, he required a prolonged hospital stay for recovery. He was given bowel rest and total parental nutrition was initiated. Due to persistent fevers, metronidazole was then added for better anerobic coverage on post-operative day 2. He stayed on IV antibiotics for one additional week and overtime his fevers resolved, his white cell count and procalcitonin continued to downtrend. Patient’s bowel function started to recover slowly and oral feedings were reinitiated. His abdominal distention and rigidity resolved overtime.
DISCUSSION
Acute urinary retention is relatively rare in pediatric population [1]. The incidence gradually increases with age, with higher rates in those above 60 years of age.
The causes of urinary retention in pediatric population include neurologic causes, urinary tract infections and local neoplasms. Fecal impaction has also been described as a common cause for urinary retention in pediatrics. However, in adult male population, prostate related issues are the leading causes [2-4].
Our patient presented to ED with urinary retention on multiple occasions. He did not have any neurological problems, evidence of overt urinary tract infection or fecal impaction, all of which are considered common causes of acute urinary retention. Workup every time showed some leukocytosis and sterile pyuria. However, he later developed acute abdomen and was diagnosed with acute perforated appendicitis with peritonitis.Therefore, his early urinary retention was in fact a manifestation of atypical appendicitis.
Review of literature suggests that urinary retention can be a very rare presenting symptom of acute appendicitis in the pediatric population with only few published case reports on this topic [3]. Other urological manifestations that have been reported include dysuria and right renal colic which result from inflammation of adjacent urological structures from the appendicitis [5]. Compression of right ureter from inflamed appendix may also occur and lead to unilateral hydronephrosis in addition to symptoms of urinary obstruction, as in our patient [6]. Due to rarity of these presenting symptoms many times the diagnosis of appendicitis can be missed until perforation with peritonitis occurs.
It is a well-known fact that appendicitis often presents with vague, atypical symptoms, especially in children <3 years, making it a diagnostic challenge. Symptoms frequently overlap with various other diseases and diagnosis may be delayed, thereby resulting in increased disease morbidity and mortality [6,7].
When acute appendicitis is suspected, abdominal ultrasound is usually considered the modality of choice for establishing the diagnosis in children due to high sensitivity, less cost and less exposure to ionizing radiations. Computed Tomography scan (CT) of the abdomen may be better modality in cases with atypical presentations and those with suspected peritonitis due to better anatomical details provided [8].
Treatment of appendicitis usually involves appendectomy and antibiotics. Laparoscopic appendectomy is usually preferred due to decreased risk of post-operative complications [9]. Abdominal wash out is performed in cases of reactive ascites and pelvic abscess formation. Preferred antibiotic regimens usually include third generation cephalosporins with addition of metronidazole or single agent regimens including piperacillin tazobactam or a carbapenem [10].
In conclusion, health care providers need to have a broad list of differentials and have high index of suspicion for childrenpresenting with acute unexplained urinary retention and hydronephrosis especially in the set-up of fever, leukocytosis and multiple visits to emergency department. When common causes of acute urinary retention are excluded, unusual or less likely causes need to be explored thoroughly. Early intervention is crucial to prevent diseasecomplications, extended hospital course and health care costs.
REFERENCES
- Gardikis S, Touloupidis S, Dimitriadis G, Limas C, Antypas S, et al. (2002) Urological symptoms of acute appendicitis in childhood and early adolescence. Int Urol Nephrol 34: 189-192.
- Gatti JM, Perez-Brayfield M, Kirsch AJ, Smith EA, Massad HC, et al. (2001) Acute urinary retention in children. J Urol 165: 918-921.
- Humes DJ, Simpson J (2006) Acute appendicitis. BMJ 333: 530-534.
- Jacobsen SJ, Jacobson DJ, Girman CJ, Roberts RO, Rhodes T, et al. (1997) Natural history of prostatism: Risk factors for acute urinary retention. J Urol 158: 481-487.
- Nevo A, Mano R, Livne PM, Sivan B, Ben-Meir D (2014) Urinary retention in children. Urology 84: 1475-1479.
- Okur SK, Koca YS, Y?ld?z ?, Barut ? (2016) Right hydronephrosis as a complication of acute appendicitis. Case Rep Emerg Med 2016: 3231862.
- Preece JM (2001) Lesson of the month: Acute urinary retention: An unusual presentation of acute appendicitis in a 3 year old boy. Archives of Disease in Childhood 84: 269-269.
- Ruffolo C, Fiorot A, Pagura G, Antoniutti M, Massani M, et al. (2013) Acute appendicitis: What is the gold standard of treatment? World J Gastroenterol 19: 8799-8807.
- Shogilev D, Duus N, Odom S, Shapiro N (2014) Diagnosing appendicitis: Evidence-based review of the diagnostic approach in 2014. West J Emerg Med 15: 859-871.
- Talan DA, Saltzman DJ, DeUgarte DA, Moran GJ (2019) Methods of conservative antibiotic treatment of acute uncomplicated appendicitis. J Trauma Acute Care Surg 86: 722-736.
Citation: Rehman R, Bashir A, Mousattat Y, Ayoob R (2020) Acute Appendicitis Presenting as Urinary Retention in a Pediatric Patient. J Nephrol Renal Ther 6: 026.
Copyright: © 2020 Rahiya Rehman, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.