Advancement of the Cognitive Function on Laser Exposure after Tumor Removal in a Case with Brain Neoplasm
*Corresponding Author(s):
Shin-Tsu ChangDepartment Of Physical Medicine And Rehabilitation, Taichung Veterans General Hospital, Tri-Service General Hospital, School Of Medicine, National Defense Medical Center, Taichung, Taipei, Taiwan, Province Of China
Tel:+886 2935605578 , +886 423741350,
Fax:+886 945605523
Email:ccdivlaser1959@gmail.com
Abstract
Background: Brain cognitive function is very important in the activities of daily life. The thalamus plays a crucial role in cognitive functions, including executive function, decision-making, memory, emotion, and language. A brain tumor can lead to serious cognitive impairments. Surgical approach may both resolve the effects of the tumor to improve cognitive function or cause permanent disabilities resulting from damage to healthy functional brain tissue. Previous studies have focused on the surgical treatments on cognitive function, and without mention alternative for treating cognitive impairment.
Patient concern: A 43-year-old male experienced severe left hemiplegia after having undergone craniectomy for brain tumor removal. His cognitive function was obviously affected by the decreased perfusion of the thalamus observed from brain images. The intravascular laser irradiation of blood (ILIB) intervened later. After three ILIB courses, his cognitive ability, especially for the memory, has been improving, along with increased perfusion in the right thalamus viewed from the second images.
Discussion: We deduce that the increase of hypoperfusion of right thalamus was attributed to ILIB, which might improve the cognitive function simultaneously. This is the first case to describe the relationship between the thalamic perfusion and cognitive function in brain tumor under ILIB. We state that ILIB could be a novel way to treat people with brain tumor, and that the brain SPECT is a worthwhile instrument in the field of scintigraphic rehabilitation for displaying the neurologic retrieval.
Keywords
Brain tumor; Cognitive function; Intravascular laser irradiation of blood, Single photon emission computed tomography; Thalamus
INTRODUCTION
Cognition, the intellectual functions, is mental process of understanding through thought, experience, and the senses, and consists of attention, the formation of knowledge, memory and working memory, judgment and calculation, comprehension, problem solving and decision making [1]. Cognitive/mental disorders have been statistically measured as 15-20% of brain tumors, and can be the initial symptoms. The severity of cognitive deficits varies from attention to many conditions, for instance, delirium, dementia or amnesic syndrome. Cognitive disorders are strongly associated with several factors including the localization and nature of the tumor, peritumoral and remote alterations, and individual vulnerability [2]. Any brain tumor occurred in the exact or abutting area of cognition-related neural paths cause cognitive impairment. Cognitive deficits, especially memory, are the most common impairment after brain tumor [3].
There are many methods to treat brain tumor, such as surgical removal of tumor [4], chemotherapy [5], radiotherapy [6], rehabilitation [7] and others [8]. All of them tend to leave with cognitive deficits, especially people whose thalamus is impaired. Cognitive impairment, arising from tissue injury caused by the tumor itself, surgical resection and chemotherapy [9], is unsure and prevalent after operation for brain tumor [10].
Any novel method has been expecting to have a more fast recovery; therefore, the intravascular laser irradiation of blood (ILIB) comes with the tide of fashion. ILIB has been used in medical conditions, as its properties of increasing microcirculation and improving oxygen supply. It has been reported with efficacy in improving oxidative stress [11] and increased healing rate of wound [12].
We herein report a case with brain tumor with subsequent cognitive impairment, who was treated with ILIB and obtained better recovery of cognition.
CASE PRESENTATION
Patient, a 43-year-old male, was robust in the past until the end of 2015. He experienced left lower limb weakness initially, which progressively developed poor ability to stand up when he woke up. There was neither numbness nor paresthesia in the beginning. He then felt difficulty in walking and stepping up the stairs Due to his worse weakness, he was introduced to our hospitalby transfer from local clinic. The results of the brain magnetic resonance (MR) imaging of brain was performed and disclosed a tumor (2.74 X 2.65 cm) located in the right subcortical peri-ventricular region abutting thalamus (Figure 1).
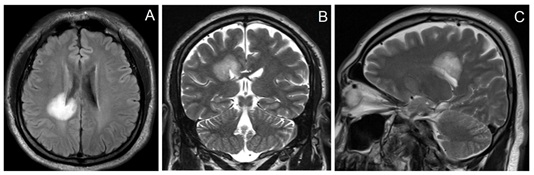
Figure 1: Brain MRI of our case before operation. This brain tumor shown as a high signal intensity on the area of the right peri-ventricular subcortical white matter in MRI T2 FLAIR image (A) which tumor abutting right thalamus. MRI T2 image, coronal view (B) MRI T2 image, sagittal view (C) MRI= magnetic resonance imaging.
He then underwent operation for craniectomy with tumor removal on January 28, 2016. According the description of Operative Note, after dissection of the skull by the neurosurgeon, the dura was opened to hinge on the edge of superior sagittal sinus and reflected medially, to avoid injury at the drainage vein originally directed to the superior sagittal sinus. The procedure of dissection of the arachnoid overlying the vein and freeing the vein from the underlying cortex provided added exposure. Application of self-retaining retractor pull the parieto-occipital lobe laterally, and the falx medially. The tumor as then removed delicately by tumor forces and micro-scissor under the microscopic maneuver. The dura was then closed and repaired. Patient was informed by the eminent surgeon as successful operation with nearly total (99.99%) removal of the entire tumor cells. The pathology confirmed it as diffuse astrocytoma (WHO grade II). Next day after operation, computer tomography (CT) of brain showed only post-operative edema around the operative area, and brain MRI checked 3 months later showed total absence of the brain tumor (Figure 2). Due to successful result of surgical resection of the brain tumor, the neurosurgeon did not endorse patient to receive chemotherapy and radiotherapy.
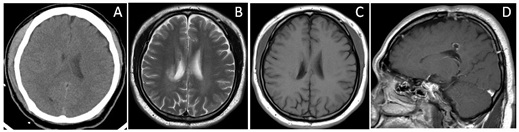
Figure 2: Radiographic films of brain after total removal of the brain tumor, one day (CT) and 3 months later (MRI). CT scan of brain one day after operation (A) MRI T2 image, axial view (B) MRI T2 FLAIR image, axial view (C) MRI T2 FLAIR image, sagittal view (D) CT = computed tomography, MRI= magnetic resonance imaging.
Right after the surgical operation, he cannot walk. According to the statement of the patient, his Left lower limb has no power but can drag his left lower limb to walk after ILIB. Though the numbness of the patient’s left side persists with hypesthesia, he still felt dramatic effect to move his left upper and lower limb with grade 3 muscles strength, which gradually improved from grade 1-2 to grade 3 after rehabilitation and ILIB. His left lower limb would tremor and be stiff when stretch and exertion, which usually happens on the patients who had impaired brain. He said, “I can walk with quad cane, but still cannot balance. The numbness on my face and left upper lower limb persists, but the sensation had improved a little bit not too obviously. I can feel the pain of injection while I could not feel the pain but numbness before.” At the last of conversation, the patient said that he has been under hot bath during the courses of ILIB, and he gets better effect.
After operation, episode of left side weakness with hypoesthesia and numbness, including left face, was noted, so intensive rehabilitation was provided. After discharge, he came to our REH OPD on November 27, 2016 for help, where poor posture, weakness with grade 1-2 muscle strength, balance and disability of walk were discovered. The ADL assessment showed impaired, and the Barthel index scores were as follows: eating (10), grooming (10), dressing(5), balance(5), bathing(0), bladder management (0), bowel management(10), stairs(0), hygiene(0), ambulation(15), urination(10). The patient’s Mini-Mental State Examination (MMSE) scores were 12 (Figure 3).
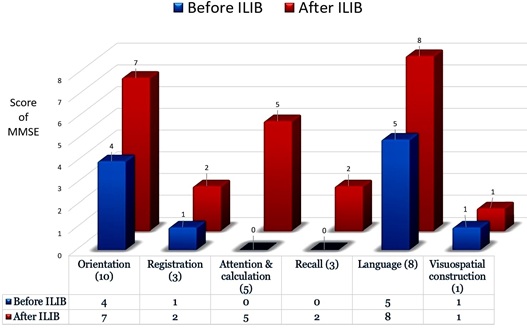
Figure 3: MMSE of the case. ILIB, intravascular laser irradiation of blood.
Initially, he reported pain of left shoulder, left wrist, and right ankle joints for many months, and dragging leg in the left side became obvious while walking. He came to our OPD on September 12, 2018 again for further treatment. The brain regional perfusion with single-photon emission computed tomography (SPECT), one year far away from the date of operation, was checked in the first time, and showed diminished uptake in the right thalamus Figure 4A.
We adopted the 632.8 nm wavelength helium-neon (HeNe) laser. The patient received three complete course of ILIB lasting an hour for 10 consecutive days. During the 3-course ILIB, patient reported no side effect, and felt his left upper lower limb range of motion improved. Although the numbness and burning-like sensation persisted, he could tolerate it without pain killers. He can now walk with quad cane with left anterior ankle-foot orthosis, even the gait pattern was still impaired with right foot vaulting and impaired balance. The patient’s memory was great before operation. After operation, his memory function decreased until the beginning of ILIB. The patient’s Mini-Mental State Examination (MMSE) scores were 29, better than 12 checked before Figure 3. Eight months later, the second brain SPECT showed improvement in some area as Figure 4B.
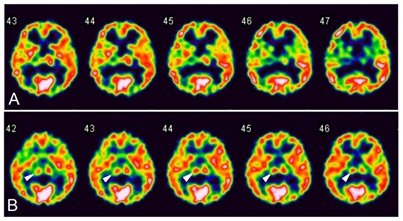
Figure 4: Regional perfusion SPECT before and after ILIB. The white to red area indicated better perfusion than the blue and green area. (A) This regional perfusion SPECT (conducted, after operation, before the patient underwent ILIB) shows the hypoperfusion on the right thalamus, where the color is blue and green. (B) The second regional perfusion SPECT (conducted after the patient underwent ILIB for 8 month, three ILIB courses) shows the improvement on the right thalamus, where the color turns red (arrowhead). SPECT, single-photon emission computed tomography. ILIB, intravascular laser irradiation of blood.
He has ever received 130 times of ILIB in our and other hospitals. Patient said that the amount of his white hair decreased, and the white-color hair was replaced with black hair, which makes him look younger after the courses of ILIB. The patient also stated that his metabolism has progressively improved due to ILIB. There were more times of urination than the time before using ILIB. In the past, he had few times of urination no matter how much water he drank. Thus, we took a look at his renal function examination report. Fortunately, although his eGFR decreased, his renal function did not show significant difference, as shown in Table 1.
Table 1: The table shows the patient’s renal function in 2016, 2017, and 2018.
|
Renal function |
24-Jan-16 |
15-Aug-17 |
13-Mar-18 |
|
BUN (mg/dL)(5-25) |
16 |
9 |
12 |
|
Creatinine (mg/dL)(M:0.7-1.4, F:0.5-0.9) |
0.8 |
0.83 |
0.99 |
|
eGFR (mL/min/1.73m2) |
113.23 |
107.99 |
87.69 |
|
(STAGE1:>=90; STAGE2: 60-89; STAGE3: 30-59.9; STAGE4:15-30; STAGE5:<15) |
The time interval of the whole clinical course, intervention, and associated evaluation was summarized in Figure 5.
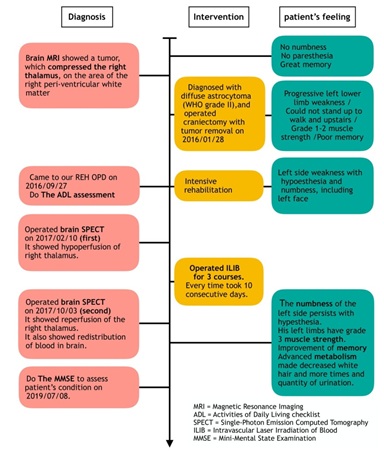
Figure 5: Time interval of the case and his self-feeling.
DISCUSSION
In our case, the decreased perfusion of the right thalamus observed from the first SPECT improved significantly when compared with the second SPECT after 3-course ILIB. The improvement of the right thalamus shown in the second SPECT correlated with advancing the function of the cognition.
Patients with brain tumors may suffer from cognitive deficits caused by the disease and/or its treatment. In a review article published in 2010, Gehring et al. [9] summarized the cognitive deficits in view of the broad domains of attention, language, memory, and executive functioning, and acclaimed potential causes for attribution as followed: 1) the tumor entity (location, size, progression and growth rate), 2) tumor-related neural complications and seizure, 3) radiation-related, early or late, with demyelination, leading to brain tissue inflammation/necrosis and impaired regeneration of hippocampal neurons; 4) antiepileptic drugs with subsequent endocrine/metabolic disturbances and psychological complication [9]. The cognitive impairment in our case should be highly related to tumor-related complication occurred in brain.
In a neuropsychological study of brain tumor, Desmond [13] found cognitive deficits highly correlate with either the location or total volume of the white matter lesions, and recognized a stronger association between cognitive deficits and those lesions in executive function, most likely due to the involvement of frontal-sub-cortical pathways [13]. The reported prevalence rates of changes in personality and/or behavior varied from 8%-67% in glioma patients [14], Our case having the brain tumor abutting the thalamus was just in the area of white matter and the fact is compatible with Desmond’s finding.
In order to address cognitive deficits in brain tumor survivors, some tailor-designing intervention programs including cognitive therapy and pharmacologic strategies, have found benefit [9]. On the other hand, we conducted ILIB for three courses, and patient appeared an obviously increased perfusion in the right thalamus, as well as the improved cognitive dysfunction, raising the realistic elucidation that improvement of thalamic perfusion and the cognition could be attributed to intervention of ILIB.
According to the literature to date, ILIB is widely used in clinical treatment to improve a lot of poor prognostic, chronic painful or stroke-causing disease, for instance, diabetes mellitus [15-17] cardiovascular disorders [18], hepatology [19], obstetrics [20], and rheumatology [21-25] and stroke [26-28] as its properties of increasing microcirculation and improving oxygen supply.
Cognitive impairment accounts for an important element of disability, and cognition has been demonstrated to be an independent predictor of survival in patients with cerebral neoplasms [29,30]. Our patient underwent 3 courses of ILIB, and his neural deficit including motor, sensation, memory and metabolism were gradually improved. A latest case report from our unit has approved that ILIB intervention can recuperate the cognitive impairment after stroke [27]. Cognition is strongly associated with function of thalamus, and in this case, the significant improvement of the patient’s right thalamus left with the better enhancement of the patient’s cognition, especially in his memory as he stated.
Our case felt that his memory got improved after using ILIB. Memory was probably related to the thalamus as the first cognitive function [31]. Thalamus is one of the crucial elements of the Papez circuit, which is an important neural structure for integrating cognitive function [32]. One article of ours confirmed that the intervention of ILIB leads to the reversibility of cognitive dysfunction in adult with stroke, indicating recovery of brain parenchymal lesions related to post-stroke cognitive impairment was attributed by the intact of Papez circuit [27]. This deduction can be fit in our case. We believe that the benefit of ILIB can contribute to the increase of right thalamus.
The fact of changing color of the patient’s hair from white to black is of interesting. ILIB is an alternative treatment for healing wound, relieving pain, promoting circulation and metabolism [15-17]. ILIB is able to induce a photobiological response inside the cells, activating the production of adenosine triphosphate (ATP), NO and reactive oxygen species, altering sodium-potassium pumps and calcium channels in cell membranes [33]. ILIB promote functional regeneration of mitochondria and pro-oxidant/ antioxidant equilibrium [11]. Furthermore, ILIB has been shown to alter ATP synthesis in white blood cells, as well as the deformation of red blood cells to pass through tiny blood vessels and amplify microcirculation [11], and to reduce low-density lipoprotein [11]. ILIB has been confirmed as biochemical modification of mitochondria and the activation of metabolic energy processes, which increases the production of ATP.
CONCLUSION
In conclusion, we deduce that the increase of hypoperfusion of right thalamus was attributed to ILIB, which might improve the cognitive function simultaneously. This is the first case to describe the relationship between the thalamic perfusion and cognitive function in brain tumor under ILIB. Based on the findings of SPECT and ensuing clinical presentation, we approve that the image is a very worthwhile instrument in the field of scintigraphic rehabilitation for the neurologic retrieval.
REFERENCES
- Stanovich KE (1990) Concepts in developmental theories of reading skill: Cognitive resources, automaticity, and modularity. Developmental Review 10: 72-100.
- Derouesné C (2015) Brain tumors, cognitive and mental disorders in adults. [Article in French] Geriatr Psychol Neuropsychiatr Vieil 13: 187-194.
- Gerstenecker A, Nabors LB, Meneses K, Fiveash JB, Marson DC, et al. (2014) Cognition in patients with newly diagnosed brain metastasis. profiles and implications. J Neurooncol 120: 179-185.
- Stummer W, Kamp MA (2009) The importance of surgical resection in malignant glioma. Curr Opin Neurol 22: 645-649.
- El-Habashy SE, Nazief AM, Adkins CE, Wen MM, El-Kamel AH, et al. (2014) Novel treatment strategies for brain tumors and metastases. Pharm Pat Anal 3: 279-296.
- Matsutani M (2004) Chemoradiotherapy for brain tumors: Current status and perspectives. Int J Clin Oncol 9: 471-474.
- Vargo M (2011) Brain tumor rehabilitation. Am J Phys Med Rehabil 90: 50-62.
- Ali FS, Hussain MR, Gutiérrez C, Demireva P, Ballester LY, et al. (2018) Cognitive disability in adult patients with brain tumors. Cancer Treat Rev 65: 33-40.
- Gehring K, Aaronson NK, Taphoorn MJ, Sitskoorn MM (2010) Interventions for cognitive deficits in patients with a brain tumor: An update. Expert Rev Anticancer Ther 10: 1779-1795.
- Perkins A, Liu G (2016) Primary brain tumors in adults: Diagnosis and treatment. Am Fam Physician 93: 211-217.
- Huang SF, Tsai YA, Wu SB, Wei YH, Tsai PY, et al. (2012) Effects of intravascular laser irradiation of blood in mitochondria dysfunction and oxidative stress in adults with chronic spinal cord injury. Photomed Laser Surg 30: 579-586.
- Mikhaylov VA (2015) The use of IntravenousLaser Blood Irradiation (ILBI) at 630-640 nm to prevent vascular diseases and to increase life expectancy. Laser Ther 24: 15-26.
- Desmond DW (2002) Cognition and white matter lesions. Cerebrovasc Dis 2: 53-57.
- Zwinkels H, Dirven L, Vissers T, Habets EJJ, Vos MJ, et al. (2016) Prevalence of changes in personality and behavior in adult glioma patients: a systematic review. Neurooncol Pract 3: 222-231.
- Kazemi Khoo N, Iravani A, Arjmand M, Vahabi F, Lajevardi M, et al. (2013) A metabolomic study on the effect of intravascular laser blood irradiation on type 2 diabetic patients. LasersMed Sci 28: 1527-1532.
- Kazemi Khoo N, Ansari F (2015) Blue or red: Which intravascularlaser light has more effects in diabetic patients? Lasers Med Sci. 30: 363-366.
- Kazemi Khoo N, Sarafnejad AF, Ansari F, Mehdipour P (2016) Modifying effect of intravenous laser therapy on the protein expression of arginase and epidermal growth factor receptor in type 2 diabetic patients. LasersMed Sci 31: 1537-1545.
- Derkacz A, Protasiewicz M, Rola P, Podgorska K, Szymczyszyn A, et al. (2014) Effects of intravascularlow-level laser therapy during coronary intervention on selected growth factors levels. Photomed Laser Surg 32: 582-587.
- Babaev AV, Gogolev DE, Reiner OV, Korochkin IM, Fandeev AV, et al. (2012) Effect of intravenouslow-intensity laser irradiation of the blood on clinical and laboratory parameters of hepatocellular insufficiency. Bull Exp Biol Med 153: 754-757.
- Mokmeli S, Khazemikho N, Niromanesh S, Vatankhah Z (2009) The application of low-level laser therapy after cesarean section does not compromise blood prolactin levels and lactation status. Photomed LaserSurg 27: 509-512.
- Timofeyev VT, Poryadin GV, Goloviznin MV (2001) Laserirradiation as a potential pathogenetic method for immune correction in rheumatoid arthritis. Pathophysiology 8: 35-40.
- Chiran DA, Litscher G, Weber M, Ailioaie LM, Ailioaie C, et al. (2013) Intravenous laser blood irradiationincreases efficacy of etanercept in selected subtypes of juvenile idiopathic arthritis: an innovative clinical research approach. Evid Based Complement Alternat Med 2013: 168134.
- Chiran DA, Weber M, Ailioaie LM, Moraru E, Ailioaie C, et al. (2014) Intravenouslaser blood irradiation and tocilizumab in a patient with juvenile arthritis. Case Rep Med 2014: 923496.
- Momenzadeh S, Abbasi M, Ebadifar A, Aryani M, Bayrami J, et al. (2015) The intravenouslaser blood irradiation in chronic pain and fibromyalgia. J Lasers Med Sci 6: 6-9.
- Liu EY, Chang ST (2019) Benefits of intravascular laser irradiation of blood on motor and sensory recovery viewing from brain function images: portrait of a case with chronic Sjögren's syndrome, transverse myelitis, and Guillain-Barré syndrome. Biomed J Sci & Tech Res 14.
- Yang WH, Lin SP, Chang ST (2017) Case report: Rapid improvement of crossed cerebellar diaschisis after intravascular laser irradiationof blood in a case of stroke. Medicine (Baltimore) 96: e5646.
- Chang JY, Liu CC, Liu IT, Chang ST (2019) Effects of intravascular laser irradiation of blood on cognitive function in a stroke survivor with hyperhomocysteinemia: dual recuperations in thalamus and serum homocysteine. Biomedical Journal of Scientific and Technical Research 16.
- Sung JH, Chang ST (2019) Reversal of impaired blood flow of the basal ganglion from the prior focal perfusion defect in a case of ischemic infarction: observation during the two stages of administration of Intravenous laser irradiation of blood. J Med Stud Res 2: 011.
- Kehayov II, Kitov BD, Zhelyazkov CB, Raykov SD, Davarski AN (2012) Neurocognitive impairments in brain tumor patients. Folia Med (Plovdiv) 54: 14-21.
- Lange M, Joly F, Vardy J, Ahles T, Dubois M, et al. (2019) Cancer-Related Cognitive Impairment: An update on state of the art, detection, and management strategies in cancer survivors. Ann Oncol pii: mdz410.
- Wolff M, Vann SD (2019) The Cognitive thalamus as a gateway to mental representations. J Neurosci 39: 3-14.
- Vann SD, Nelson AJD (2015) The mammillary bodies and memory: More than a hippocampal relay. Prog Brain Res 219: 163-185.
- Isabella APJ, Silva JTC, da Silva T, Rodrigues MFSD, Horliana ACRT, et al. (2019) Effect of irradiation with intravascular laser on the hemodynamic variables of hypertensive patients: Study protocol for prospective blinded randomized clinical trial. Medicine (Baltimore) 98: e15111.
Citation: Liu PY, Liu CC, Liu IT, He HC, Chang ST (2019) Advancement of the Cognitive Function on Laser Exposure after Tumor Removal in a Case with Brain Neoplasm. J Light Laser Curr Trends 2: 006.
Copyright: © 2019 Chuan-Ching Liu, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.