Analysis of the Ventilation Scan in the Evaluation of CTEPH
*Corresponding Author(s):
Geoffrey M CurrieSchool Of Dentistry And Health Sciences, Locked Bag 588, Charles Sturt University, Wagga Wagga 2678, Australia
Tel:+61 269332822,
Email:gcurrie@csu.edu.au
Abstract
Introduction: Early diagnosis of acute pulmonary embolism (PE) and a subsequent fast response in thrombolytics treatment is a key element in preventing progression to Chronic Thrombo-Embolic Pulmonary Hypertension (CTEPH). Lung ventilation and perfusion scintigraphy (V/Q) has been widely accepted as the preferred initial diagnostic imaging screening procedure for CTEPH. This study aimed to evaluate the performance of different ventilation methods in detecting CTEPH.
Methods: Data of completed V/Q studies and reports of 167 consecutive patients for further investigation of suspected CTEPH, were retrieved for analysis. All data was retrospectively analysed by two nuclear medicine physicians. The specificity, sensitivity, accuracy, positive predictive values (PPV), and negative predictive values (NPV), false positive rate and false negative rate of V/Q and CTPA were derived and calculated from these data.
Results: Of the 167 patients, 64 (38.3%) had a final diagnosis of CTEPH. While there were 64 positive cases for CTEPH, CTPA was positive for only 18 while the VQ was positive for all 64. Compared to DTPA aerosol, Technegas demonstrated superior positive predictive value, sensitivity and specificity with comparable negative predictive value and accuracy.
Conclusion: In suspected CTEPH, a high/intermediate V/Q report is consistent with a positive diagnosis. The use of Technegas for ventilation improves the positive predictive value and sensitivity over aerosol ventilation.
Keywords
Footline: Lung Ventilation in CTEPH; Lung scan; Perfusion; Pulmonary hypertension
INTRODUCTION
Chronic Thrombo-Embolic Pulmonary Hypertension (CTEPH) is a rare chronic condition of unresolved acute Pulmonary Embolism (PE) after more than three months of curative anticoagulation treatment [1]. Current guidelines recommend ventilation and perfusion scintigraphy (V/Q) as the first choice of imaging tool in suspected CTEPH to screen for the presence of thromboembolic disease [1]. V/Q is widely been accepted as being associated with a lower radiation dose to the patients and without possible complications from intravenous contrast injections [2]. The European Association of Nuclear Medicine (EANM) and the 2009 European Guidelines recommend V/Q to screen for CTEPH in cases where pulmonary hypertension is unexplained with a previous episode of PE [3]. Nonetheless, there are wide variations in the selection of imaging tests, including Computed Tomography Pulmonary Angiography (CTPA) in diagnosing CTEPH, and the choice of imaging modality often reverts to expertise and the availability, and thus preference.
The overall estimated incidence of CTEPH in Europe is between 3.3 (United Kingdom) to 5 (France) per 100,000 of population per year [4]. In the United States (US), there are 5.1 cases per 100,000 populations per year while Japan is 1.9 cases per 100,000 populations per year [4]. While the number of cases is reduced in Japan and generally across Asia compared to Europe and the US, an important observation is that the number of cases of CTEPH per case of PE reflects a more significant issue in Asia. Fir Europe and the US, 1 case of CTEPH emerges for every 20 cases of PE while in Japan (and other nations of South East Asia), there is 1 CTEPH case for every 4 PE cases [4-7].
Recent investigations of pooled data across multiple investigators [8] revealed 84% sensitivity and 94% specificity of CTPA for CTEPH compared to 94% sensitivity and 99% specificity of SPECT V/Q, and 85% sensitivity and 85% specificity for planar V/Q. The Area Under the Curve (AUC) for the Receiver Operator Characteristic (ROC) analysis was 0.96, 0.98 and 0.89 for CTPA, SPECT V/Q and planar V/Q respectively. Unfortunately, the ventilation data was contaminated by various procedural approaches including 99mTc-Technegas, 99mTc-DTPA aerosol, 81m-Krypton, 133-Xenon ventilation methods. In unpublished research by this group, the value of the ventilation study was in improving specificity (86% for perfusion only to 99% for V/Q), with no impact on sensitivity. The meta-analysis [8] may have underestimated the specificity of the planar V/Q scan with the SPECT V/Q data including only the Technegas approach. In a single site investigation [9] comparing CTPA and V/Q scan in 133 consecutive patients, sensitivity and specificity were 98% and 95% respectively for V/Q scan while CTPA reported 19% and 99% sensitivity and specificity for CTEPH. Ventilation scans were performed using a combination of 99mTc-DTPA aerosol and 99mTc-Technegas. It was noted that 99mTc-DTPA aerosols produced a higher proportion of indeterminant scans which produced more false negative studies. The objective of this study was to investigate the performance of V/Q in the diagnosis of CTEPH based on the method of ventilation.
METHODS
Completed V/Q images and reports, as well as the full clinical history of 7190 consecutive CTPA patients and 990 consecutive V/Q patients referred to the institution between 2005 and 2020 for further investigation of suspected CTEPH were retrieved for analysis. The study data consisted of planar V/Q studies carried out with either 99m-technetium (99mTc) Diethylenetriaminepentaacetic acid (DTPA) aerosol or 99mTc Technegas as the ventilating agent. Inclusion criteria comprised patients who are 18 years or older, patients whose nationalities are of Southeast Asian (SEA) origins, clinical suspicion of CTEPH as the basis of having undergone the V/Q scan, both ventilation and perfusion were performed, a corresponding computed tomography pulmonary angiogram (CTPA) study, and a diagnosis made at the completion of the scan.
Both CTPA and V/Q protocols and equipment remained consistent during the data collection period. In all CTPA acquisitions, the bolus tracking technique was applied, with the introduction of 40 millilitres (ml) of Omnipaque 350 at 3.5 to 4ml per second (s), and flushing with 30 mls of saline at the rate of 3 ml/s. The scan coverage was from the apex of the lungs to the base of the lungs, with the entire chest volume scanned in one acquisition in the caudocranial direction with 3mm slice reconstruction. All CTPA studies were performed on one of four scanners; Philips iCT 256 slice, Philips Brilliance 64 slice, GE Revolution 512 slice or Siemens Force 384 slice. V/Q studies were carried out with a two-day protocol using 500K counts planar imaging. All V/Q scans followed the same protocol on one of 3 gamma cameras; GE Optima, Siemens Symbia or Siemens ECam. From January 2005 to July 2015, ventilations were carried out with 99mTc-DTPA aerosol using the UltraVent nebulizer. Subsequent ventilations from August 2015 were carried out with 99mTc Technegas delivered from the Technegas generator.
The completed V/Q and CTPA images, reports, and relevant clinical history were consolidated and analysed. V/Q data were grouped according to high probability PE, intermediate probability PE, and low probability PE, and were analysed against their respective final CTEPH reports. The specificity, sensitivity, accuracy, Positive Predictive Values (PPV), and Negative Predictive Values (NPV), false positive rate and false negative rate of V/Q and CTPA were derived and calculated from these data. The study was approved by an institutional ethics committee.
RESULTS
Among more than 7000 patients included in the investigation, there were 167 patients with pulmonary hypertension that underwent both the V/Q and CTPA procedures and met the inclusion criteria. Of the 167 patients, 64 (38.3%) had a final diagnosis of CTEPH. While there were 64 positive cases for CTEPH, CTPA was positive for only 18 while the VQ was positive for all 64 (Table 1). Of the 81 patients who had Technegas ventilation, 39 (48.1%) had a final diagnosis of CTEPH and V/Q had a sensitivity and specificity of 97% and 95% respectively using high and intermediate probability outcomes as positive for CTEPH (Table 2). Of the 86 patients who had DTPA aerosol ventilation, 25 (29.1%) had a final diagnosis of CTEPH and V/Q had a sensitivity and specificity of 100% and 95% respectively using high and intermediate probability outcomes as positive for CTEPH (Table 3). When only a high probability outcome was used to determine CTEPH, increased specificity with decreasing sensitivity was noted. For Technegas ventilation the sensitivity for CTEPH was 69% and specificity 100% while for DTPA aerosol sensitivity was 44% and specificity 97%. This observation reflects the higher number of indeterminant ventilation scans associated with aerosols. Compared to DTPA aerosol, Technegas demonstrated superior positive predictive value, sensitivity and specificity with comparable negative predictive value and accuracy (Table 4).
|
|
CTPA (%) |
V/Q (Technegas plus Aerosol) |
|||
|
High probability |
High + Intermediate probability |
Low probability / normal |
Intermediate + low probability / normal |
||
|
True positive |
n = 18 (28.1%) |
38 (59.4%) |
64 (100%) |
- |
- |
|
False positive |
n = 4 (6.3%) |
2 (3.1%) |
4 (6.3%) |
- |
- |
|
True negative |
n = 99 (96.2%) |
- |
- |
82 (79.6%) |
85 (82.5%) |
|
False negative |
n = 46 (44.7%) |
- |
- |
1 (1.0%) |
26 (25.2%) |
|
Positive predictive value (PPV) |
81.8% |
95.0% |
94.1% |
- |
- |
|
Negative predictive value (NPV) |
68.3% |
76.6% |
98.8% |
- |
- |
|
Accuracy |
70.1% |
81.5% |
96.7% |
- |
- |
|
Sensitivity |
28.1% |
59.4% |
98.5% |
- |
- |
|
Specificity |
96.1% |
97.7% |
95.4% |
- |
- |
Table 1: Summary of performance characteristics of CTPA and V/Q in CTEPH for combined ventilation techniques.
|
|
V/Q |
|||
|
High probability |
High + Intermediate probability |
Low probability / normal |
Intermediate + low probability / normal |
|
|
True positive |
27 (69.2%) |
38 (97.4%) |
- |
- |
|
False positive |
0 (0%) |
2 (5.1%) |
- |
- |
|
True negative |
- |
- |
40 (95.2%) |
42 (100%) |
|
False negative |
- |
- |
1 (2.4%) |
12 (28.6%) |
|
Positive predictive value (PPV) |
100% |
95.0% |
- |
- |
|
Negative predictive value (NPV) |
77.8% |
97.6% |
- |
- |
|
Accuracy |
85.2% |
96.3% |
- |
- |
|
Sensitivity |
69.2% |
97.4% |
- |
- |
|
Specificity |
100% |
95.2% |
- |
- |
Table 2: Summary of performance characteristics of 99mTc-Technegas ventilation-based V/Q in CTEPH.
|
|
V/Q |
|||
|
High probability |
High + Intermediate probability |
Low probability / normal |
Intermediate + low probability / normal |
|
|
True positive |
11 (44.0%) |
25 (100%) |
- |
- |
|
False positive |
2 (8.0%) |
3 (12.0%) |
- |
- |
|
True negative |
- |
- |
58 (95.1%) |
59 (96.7%) |
|
False negative |
- |
- |
0 (0%) |
14 (22.9%) |
|
Positive predictive value (PPV) |
84.6% |
89.3% |
- |
- |
|
Negative predictive value (NPV) |
80.8% |
100% |
- |
- |
|
Accuracy |
81.4% |
96.5% |
- |
- |
|
Sensitivity |
44.0% |
100% |
- |
- |
|
Specificity |
96.7% |
95.1% |
- |
- |
Table 3: Summary of performance characteristics of 99mTc-DTPA aerosol ventilation-based V/Q in CTEPH.
|
|
Technegas |
DTPA |
||
|
High probability |
High + Intermediate probability |
High probability |
High + Intermediate probability |
|
|
Positive predictive value (PPV) |
100% |
95.0% |
84.6% |
89.3% |
|
Negative predictive value (NPV) |
77.8% |
97.6% |
80.8% |
100% |
|
Accuracy |
85.2% |
96.3% |
81.4% |
96.5% |
|
Sensitivity |
69.2% |
97.4% |
44.0% |
100% |
|
Specificity |
100% |
95.2% |
96.7% |
95.1% |
Table 4: Summary of performance characteristics of 99mTc-Technegas and 99mTc-DTPA aerosol ventilation-based V/Q in CTEPH.
DISCUSSION
Lung perfusion imaging in V/Q scintigraphy has the diagnostic ability in visualising small occlusive clots in small vessels and provides a clearer representation of haemodynamic significance, which are not easy to identify with CTPA [10]. Although technological advancements in CT have seen CTPA challenge V/Q as the primary mode of imaging investigation in the diagnosis of PE (Figure 1), there remains a significant disparity in performance in CTEPH. In this study, CTPA has shown to be markedly less sensitive than V/Q in the diagnosis of CTEPH with a comparable specificity. It should be noted that this study was undertaken using planar V/Q and that SPECT V/Q further enhances V/Q performance compared to CTPA [8].
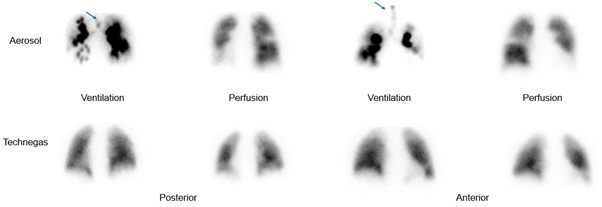 Figure 1: Representative images of the challenges associated with central (arrow) and large airways deposition of 99mTc-DTPA aerosol confounding perfusion interpretation (top). A more typical homogenous distribution using 99mTc-Technegas ventilation does not confound diagnosis of CTEPH on corresponding perfusion images (bottom).
Figure 1: Representative images of the challenges associated with central (arrow) and large airways deposition of 99mTc-DTPA aerosol confounding perfusion interpretation (top). A more typical homogenous distribution using 99mTc-Technegas ventilation does not confound diagnosis of CTEPH on corresponding perfusion images (bottom).
In the comparison between 99mTc Technegas and 99mTc-DTPA aerosol as ventilation agents, the performance of 99mTc-DTPA aerosol in terms of PPV (84.62% versus 100%), accuracy (81.40% versus 85.19%), sensitivity (44.00% versus 69.23%) and specificity (96.72% versus 100%) were markedly inferior to that of 99mTc Technegas when only high probability reports were included in the diagnosis of CTEPH. When both high and intermediate probability reports were included as CTEPH positive, the 99mTc-DTPA aerosol results were comparable to that of 99mTc Technegas.
Technegas is a ventilation system that delivers a dispersion of ultrafine 99mTc-labelled carbon particles to the lungs and overcomes the hot spot formation associated with droplet deposition and aggregation using aerosol techniques [11]. Indeed, the first head to head comparison of 99mTc-Technegas and 99mTc-DTPA aerosol for lung ventilation studies reported significantly higher central disposition in normal and obstructive airways for the aerosol with greater peripheral penetration and dispersion for Technegas [11]. The inclination for central deposition of aerosol-based ventilation agents is likely responsible for the decreased positive predictive value of 99mTc-DTPA aerosol compared to 99mTc-echnegas in this study. This central deposition will be compounded in SPECT reconstruction and, thus, the enhanced performance of Technegas noted in this planar investigation is likely to be more pronounced in SPECT data.
CONCLUSION
This investigation demonstrated that V/Q is a more valuable diagnostic imaging tool in detecting CTEPH than CTPA. In suspected CTEPH, a high/intermediate V/Q report is consistent with a positive diagnosis. The use of Technegas for ventilation improves the positive predictive value and sensitivity over aerosol ventilation. This is an important finding as CTEPH is a potentially treatable condition.
REFERENCES
- Kim NH, Delcroix M, Jenkins DP, Channick R, Dartvelle P, et al. (2013) Chronic Thromboembolic Pulmonary Hypertension. Journal of the American College of Cardiology 62: D92-95.
- Freeman JM (2007) Don’t bury the V/Q scan: It’s as good as multidetector CT angiograms with a lot less radiation exposures. Journal of Nuclear Medicine 49: 5-8.
- Bajc M, Neilly JB, Miniati M (2009) EANM guidelines for ventilation/perfusion scintigraphy: Part 1. Pulmonary imaging with ventilation/perfusion single photon emission tomography. European Journal of Nuclear Medicine Molecular Imaging 36:1356-1370.
- Bazmpani MA, Arvanitaki A, Toumpourleka M, Pitsiou G, Panagiotidou E, et al. (2017) Epidemiology and management of chronic thromboembolic pulmonary hypertension: experience from two expert centers. Hellenic Journal of Cardiology 59: 16-23.
- Park SY, Lee SM, Shin JW, Choi BW, Kim H, et al. (2016) Epidemiology of chronic thromboembolic pulmonary hypertension in Korea: results from the Korean registry. The Korean Journal of Internal Medicine, 31: 305-312.
- Baptista R, Meireles J, Agapito A, Castro G, da Silva AM, et al. (2013) Pulmonary hypertension in Portugal: first data from a nationwide registry. BioMed Research International 489-574.
- United Nations (2017) World Population Ageing 2017 - Highlights (ST/ESA/SER.A/397). Department of Economic and Social Affairs, Population Division (2017).
- Tong M, Wheat J, Currie G (2020) A review of medical imaging in the evaluation of PE and CTEPH. Pakistan Journal of Nuclear Medicine 10: 1-11.
- Tong M, Wheat J, Currie G (2020) Efficacy of ventilation perfusion lung scan (V/Q) and computed tomography pulmonary angiography (CTPA) for chronic thrombo-embolic pulmonary hypertension (CTEPH). Journal of Nuclear Medicine and Radiation Sciences 1: 2-6
- Hoey ETD, Gopalan D, Ganesh V (2009) Dual-energy CT pulmonary angiography: a novel technique for assessing acute and chronic pulmonary thromboembolism. Clinical Radiology 64: 414-419.
- Jogi J, Jonson B, Ekberg M, Bajc M (2010) Ventilation-perfusion SPECT with 99mTc-DTPA versus technegas: a head-to-head study in obstructive and nonobstructive disease. Journal of Nuclear Medicine 51: 735-741.
Citation: Tong M, Wheat J, Currie GM (2020) Analysis of the Ventilation Scan in the Evaluation of CTEPH. J Nucl Med Radiol Radiat Ther 5: 020.
Copyright: © 2020 Michael Tong, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.