Asparagus Induced Fixed-Food Eruption
*Corresponding Author(s):
Laura A AndrewsMedical University Of South Carolina College Of Medicine, Bee St. Apt 612, Charleston, SC 29401, United States
Tel:+1 8436013892,
Email:andrewla@musc.edu
Abstract
Fixed drug eruptions are localized, cutaneous type IV hypersensitivity reactions that are typically caused by exposure to new or intermittently-administered medications. However, if no pharmacological source is identified, a food or food additive may be considered as a causative agent. There are a limited number of documented fixed food eruptions in the literature, and those described differ in both appearance and timing of presentation. Management of these cutaneous eruptions includes avoidance of the causative agent, antihistamines as needed for pruritis, and treatment with topical steroids if necessary. We present the case of a fixed food eruption caused by asparagus ingestion.
Case Report
A 53-year-old male with a past medical history of asthma and hypertension presented to the dermatology clinic with multiple scaly well-demarcated circinate pink-red plaques on the bilateral lower extremities. The largest of these was 4 x 4 cm on the right distal lateral leg (Figure 1). He reported the lesions waxed and waned for approximately 10 years prior to this visit. Topical betamethasone dipropionate 0.05% ointment was prescribed. Two years later, the patient returned to the clinic and reported he continued to experience occasional flares of the lesions, notably after certain meals.
 Figure 1: Circinate pink-red plaques on right distal lateral leg.
Figure 1: Circinate pink-red plaques on right distal lateral leg.
Biopsy was obtained and revealed a basket-weave stratum corneum, interface dermatitis, polymorphous inflammatory infiltrate, papillary dermal fibrosis and melanophages surrounding the superficial vessels of the dermis, histologically consistent with a “fixed drug eruption” (Figures 2&3). Interestingly, the patient reported that the lesions flared within 24 hours of eating asparagus.
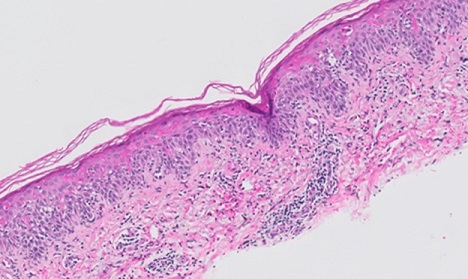 Figure 2: H&E x10 - Acute stratum corneum with vacuolar change along basilar layer and apoptosis of keratinocytes throughout all layers of the epidermis.
Figure 2: H&E x10 - Acute stratum corneum with vacuolar change along basilar layer and apoptosis of keratinocytes throughout all layers of the epidermis.
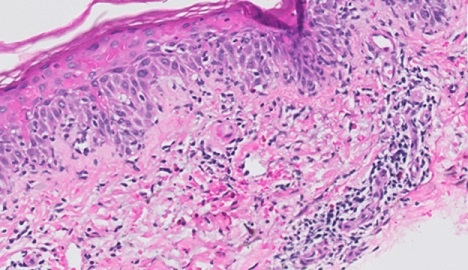 Figure 3: H&E x20 - Papillary dermal fibrosis and melanin pigment incontinence in a perivascular location and polymorphous infiltrate in dermis of lymphocytes and eosinophils.
Figure 3: H&E x20 - Papillary dermal fibrosis and melanin pigment incontinence in a perivascular location and polymorphous infiltrate in dermis of lymphocytes and eosinophils.
Discussion
A Fixed Drug Eruption (FDE) is a localized, cutaneous type IV hypersensitivity reaction occurring after ingestion of an offending agent. FDEs typically occur in the context of a new or intermittently-administered medication, the most common of which include: sulfonamides, non-steroidal inflammatory drugs, salicylates, barbiturates, and oral contraceptives [1]. However, if no pharmacological source is identified, a food or food additive may be implicated. This rare allergy was first defined in 1996 as a “Fixed Food Eruption (FFE)” [2]. There are few documented cases of these so called “fixed food eruptions (FFE)”, with only 15 available case reports in 2016. Tonic water (quinine), seafood, cashews, peanuts, lentils, bee pollen (propolis), strawberry, lactose, quinoline yellow dye and cheese crisps (+/- tartrazine) were the causative agents. TwoFFEs resulting from asparagus consumption have also been documented [3].
While fixed eruptions caused by both drugs and food tend to recur in the same location on the body - as indicated by the term “fixed” - they differ in some clinical characteristics. The few FFEs described in the literature are highly variable in their appearance as well as their timing; they range from hyperpigmented bullae to violaceous plaques that appear as early as 15 minutes to as late as a full week after ingestion. This heterogeneity of presentation among the FFEs suggests that they may differ in mechanism as well, although this has yet to be elucidated. In contrast, FDEs typically present with macular lesion(s) that develop hours after the drug exposure. FFEs also lack the residual hyperpigmentation characteristically present after fixed drug eruptions [4].
Of five known skin biopsies of active fixed food eruptions, three displayed a T-cell dependent pathway with induction of IFNy-producing CD8+ T cells in the dermis and epidermis, one exhibited a co-expression of neutrophils and eosinophils and the other had neutrophilic polymorphonuclear perivascular infiltration [5].
The differential diagnosis for an FDE presenting as a psoriasiform dermatitis includes conditions such as cutaneous T-Cell Lymphoma (CTCL), urticarial phase of bullous pemphigoid, and psoriasis. CTCL, which comprises a heterogenous group of non-Hodgkin lymphomas, was particularly important to rule out in this patient, whose age and gender fit the most common demographic for CTCL [6]. Histopathology made this distinction.
The management of a fixed drug or food eruption includes avoidance of the causative agent, antihistamines for pruritis, and treatment with topical steroids if necessary [1]. Our patient cleared his most recent episode with triamcinolone ointment twice daily for two weeks and avoidance of asparagus ingestion.
References
- Flowers H, Brodell R, Brents M, Wyatt J (2014) Fixed Drug Eruptions: Presentation, Diagnosis, and Management. South Med J 107: 724-727.
- Kelso JM (1996) Fixed food eruption. Journal of the American Academy of Dermatology 35: 638-639.
- Tattersall I, Reddy B (2016) Fixed Drug Eruption due to Achiote Dye. Case Reports in Dermatology, 8: 14-18.
- Parker A, Pinson M, Wohltmann W, Gomez R (2015) Fixed food eruption caused by peanut and cashew: A case report and review of the literature. J Allergy Clin Immunol Pract 3: 119-122.
- Sohn KH, Kim BK, Kim JY, Song WJ, Kang HR, et al. (2017). Fixed Food Eruption Caused by Actinidia arguta (Hardy Kiwi): A Case Report and Literature Review. Allergy, asthma & immunology research 9: 182-184.
- Wilcox R (2017) Cutaneous T-cell lymphoma: 2017 update on diagnosis, risk-stratification, and management. Am J Hematol 92: 1085-1102.
Citation: Andrews LA, Robinson I, Xu M, Winterfield L, Scribner J (2021) Asparagus Induced Fixed-Food Eruption. J Clin Dermatol Ther 7: 090.
Copyright: © 2021 Laura A Andrews, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.