Assessment of Patients Radiation Doses during Computed Tomography Chest Imaging Examination: Propose Diagnostic Reference Level
*Corresponding Author(s):
Ojike Peter EkwulugwoDepartment Of Radiology, Federal University Owerri Teaching Hospital, Imo State, Nigeria
Email:saintpeterlivy@gmail.com
Abstract
In medical imaging, Computed Tomography (CT) scan examination is a major source of ionizing radiation. All medical radiological exposures should be justified and optimized to meet up with the needed clinical outcome. Therefore, to avoid unnecessary radiation doses to patients, Diagnostic Reference Levels (DRLs) for CT examinations should be adhered to. The DRLs are used to identify radiation dose outliers during CT scan examinations, which does not contribute to good clinical diagnosis. DRLs have been successfully implemented in the UK, Australia, Japan, Canada and United States of America; and a few underdeveloped countries. The present study aimed at assessment of patients’ radiation dose during chest CT scan examination with a view to establishing local diagnostic levels in Rivers State, South-South, Nigeria. Sixty (60) adult patients comprising of 20 patients from center A, 20 patients from center B, and 20 patients from centre C were purposively sampled. The patients aged between 16-100 years and weighed 70±10 kg. The prospective data collection spans four months, and CTDIv and DLP were retrieved after each CT scan examination. SPSS version 25.0 was used to analyze data. Mean CTDIv and DLP values were calculated and their 75th percentile value was obtained as the DRL for anatomical region studied. DRLs proposed for chest CT examinations for Rivers state were: 10.6 mGy and 414.70 mGy.cm for CTDIv and DLP respectively. These values are lower than the European Commission DRLs and comparable to other international studies. Wide variation in mean doses are noted across the region. Therefore, the chest CT examination practice within the region is optimized.
Keywords
Computed Tomography; Dose Length Product; Diagnostic Reference Level; Optimization; Medical Imaging; Volumetric Computed Tomography Dose Index
Introduction
Computed Tomography (CT) is a valuable medical imaging examination for the diagnosis of wide range of chest diseases such as breast cancer, interstitial lung diseases, lung abscess [1,2] Sequel to development of Multi-Dictator Computed Tomography (MDCT) machines, new clinical applications are continuously evolving in medical procedures. It is estimated that in UK, computerized tomography examinations are the leading cause of 40% of annual collective dose resulting from medical exposure in 1999 compared to 20% in 1990 [3,4]. This increase in population radiation dose burden is of utmost concern to mankind due to the possibility of radiation induced malignant diseases like cancer [5,6] Therefore, sensible use of this imaging modality requires strict adherence to the principles of radiation protection: Justification, optimization and dose limitation, ensuring that the risk to patients does not outweigh the benefit gained from the procedure [7,8]. Doses are routinely estimated by using standard 16cm or 32 cm diameter Polymethylmethacrylate (PMMA) cylinder phantom representing “average” patients [9,10]. Although, the CT dose in chest imaging is high, tissue reactions are not expected because a specific threshold is required for it to occur, about 2000 mGy [11,12]. In CT chest imaging, the dose to skin is ranged between 20 mGy-40 mGy [13,14]. The International Commission on Radiological Protection (ICRP) recommended that Diagnostic Reference Levels (DRLs) should be used by regional, national and local authorized bodies like Nigeria Nuclear Regulatory Authority (NNRA), so as to minimized the patient doses from unnecessary exposure by keeping all patient exposures to as low as reasonably achievable (ALARA Concept) [15,16]. In CT examinations, the volume Computed Tomography Dose Index (CTDIv) and Dose Length Product (DLP) are the parameters used to estimate the dose to the standard phantom representing average patients [17,18]. The CTDIv represents the average dose to a cross section of a phantom (measured in mGy) [6,7]. Dose length Product (DLP) is the product of the CTDIv and the scan Length (L) for a group of scans along x-axis (measured in mGy.cm) [19,20]. Currently, these two dosimetric variables are displayed on CT dose reports page after each scan series. The aim of this study was to estimate the radiation dose to adult patient during chest computed tomography imaging examination in Rivers state, Nigeria, and to establish local diagnostic reference levels.
Materials And Methods
Materials
The materials required for the conduct of this research were Computed Tomography Scanner Machines which is domiciled at the study centre, IAEA recommended data collection sheet, SPSS version 25 software for data analysis and Ethical clearance obtained from the participating centers.
Study Area: The study area was located in Port Harcourt Rivers State. The three study centres were all located in the Port Harcourt City.
- Methods
This study adopted a prospective and quantitative research design to estimate the absorbed radiation dose to patient undergoing CT scan of the chest. A quantitative design was appropriate because the study involved the use of numerical data.
Study Population: The study involved all adult patients that attended for chest CT scan examinations in the studied centers.
Ethical Consideration: In line with Helsinki declaration 1964 on research involving human subjects, ethical approval and consent was granted by studied centers and patients’ confidentiality was maintained by obtaining an informed consent before participating in the research.
Data Collection: The data was collected with the assistance of a CT radiographer who was trained on how to collect the data.
Sample Size: A sample size of sixty (60) qualified patients were recruited for chest CT in the study. This was obtained through selection of twenty (20) participants from centre A, (20) from B, and (20) from C respectively.
Inclusion Criteria
- Only ambulant adult patients weighing 70±10 kg was included in the study [21,22].
- Only adult patients that presented for chest CT scan examinations were considered.
- Data was acquired on a CT scanner routinely calibrated by the Nigeria Nuclear Regulatory Authority (NNRA).
Exclusion Criteria: Generally, all the patients that do not fall within the inclusion criteria were excluded from the study.
- Data Analysis
CT dose index (CTDI (mGy)), which is the measure of the dose from single-slice irradiation is defined as the integral along a line parallel to the axis of rotation (z) of the dose profile, D(z), divided by the nominal slice thickness, T as shown in Equation 1 [23].
 The weighted CT air kerma index, CTDIw (mGy), used to combine values of CTDI measured at the centre (c) and periphery (p) of a standard CT dosimetry phantom as shown in Equation 2 [23]
The weighted CT air kerma index, CTDIw (mGy), used to combine values of CTDI measured at the centre (c) and periphery (p) of a standard CT dosimetry phantom as shown in Equation 2 [23]
 Volumetric computed tomography dose index (CTDIv) is expressed as the average dose delivered to the scan volume for specific examination. It is derived from the CTDI. For a single slice scanner, CTDIv is defined by Equation 3 as:
Volumetric computed tomography dose index (CTDIv) is expressed as the average dose delivered to the scan volume for specific examination. It is derived from the CTDI. For a single slice scanner, CTDIv is defined by Equation 3 as:
 Where N is the number of scans, T is the nominal scan width (mm) and L is the distance between scans (mm) [23].
Where N is the number of scans, T is the nominal scan width (mm) and L is the distance between scans (mm) [23].
For MSCT system, NXT is the total nominal scan width, and I correspond to the patient table movement during one gantry rotation. According to the work of [24] the Multiple Scan Average Dose (MSAD) for spiral scans can be expressed in Equation 4 as:
 Comparing Equation 3 and 4, we have Equation 5;
Comparing Equation 3 and 4, we have Equation 5;

Results
To compute the result for the chest CT dose examination for adult patient in Rivers State radio-diagnostic centers in Nigeria, CT scanner type, model, number of slices, year of manufacture and year of installation were obtained, recorded and presented in (Table 1). Also, the patients’ average age (years) and weight (kg) were measured and the patients’ gender characteristics were all shown in (Table 2). Lastly, the CT scan parameters (anthropo-technical features) like kV, mA, Scan length, pitch, FOV, CTDIv and DLP were calculated and presented in (Table 3).
|
Centre |
Manufacturer |
Model Detector |
Configuration |
Manufactured Year |
Installed Year |
|
A |
Siemens |
Somatom |
16-Slice |
2019 |
2019 |
|
B |
General Electric (GE) |
Brivo |
8-Slice |
2015 |
2015 |
|
C |
General Electric (GE) |
Bright Speed |
4-Slice |
2006 |
2015 |
Table 1: Details of Facility CT Scan Machines.
|
Centre |
Examination Type |
Age ± SD (years) |
Sex |
Total |
Mean Weight ± SD (kg) |
|
|
M |
F |
|||||
|
A |
Chest |
60.17±16.59 |
12 |
8 |
20 |
74.09±8.44 |
|
B |
Chest |
59.40±13.66 |
9 |
11 |
20 |
74.95±5.56 |
|
C |
Chest |
54.71±6.82 |
9 |
11 |
20 |
71.55±7.22 |
Table 2: Demographic distribution and patient’s Chest characteristics of the study population.
|
Centre |
Examination |
kV |
mA |
Scan Length |
Pitch |
FOV |
|
A |
Chest |
110 |
125.22 |
5.12 |
1.09 |
30.17 |
|
B |
Chest |
110 |
57.950 |
30.60 |
0.83 |
30.00 |
|
C |
Chest |
120 |
185.30 |
37.35 |
0.98 |
36.20 |
Table 3: Scan parameters for all the studied centers.
- Result Analysis
In order to analyze the obtained results, bar charts were plotted and comparison was made with international recommendations, and some Nigeria authors’ local and regional values.
Discussion
In this study we investigated the patient’s radiation dose during chest CT scan examination and based on that propose diagnostic reference level for that anatomical body region for South-South, Nigeria. Both male and female patients were involved in the study with the percentage of males = 30 (50%), and females = 30 (50%) for the population. The radiological centers studied were selected because they met the inclusion criteria for the study having a functional and accredited CT scan machine.
(Table 1) shows details of different CT scan machines available in the three studied centers, manufacturers, model, detector configurations, year of manufacture and installation.
Demographic distribution and patient chest dose characteristics of the studied population was detailed in (Table 2). The centers A, B and C patients’ mean age (in years), with their standard deviation were, respectively 60.17±16.59, 59.40±13.66 and 54.71±6.82.
Sixty (60) males and females’ patients with twenty (20) in center A, twenty (20) in B and twenty (20) in C were recruited. The patient’s respective mean weights were (in kg), 74.09 ± 5.49, 74.95±5.01 and 71.55±7.22 for centres A, B and C respectively. The scan parameters of the studied centers were shown in (Table 3) and (Figure 1). The Centre Mean Dose in terms of CTDIv (mGy) and DLP (mGy.cm) and standard deviation for CT of chest in the studied region were shown on (Table 4) and (Figure 2). The mean CTDIv were 9.72±1.73 mGy, 5.60±1.75 mGy and 11.15±4.02 mGy for centres A, B and C respectively. While, the mean DLP were 322.03 ± 33.87 mGy.cm, 241.95±53.78 mGy.cm and 485.10±51.36 mGy.cm for centers A, B and C respectively. Observable CT dose patient variation exist among the studied centers. This is due to different CT scan parameters kVp, scan range, time, pitch, time and mAs among the centers.
|
Centre |
Body Region |
CTDIv (mGy) |
DLP (mGy.cm) |
|
A |
Chest |
9.72±1.73 |
322.03±33.87 |
|
B |
Chest |
5.60±1.75 |
241.95±53.78 |
|
C |
Chest |
11.15±4.02 |
485.10±51.36 |
Table 4: Centre Mean Dose in Terms of CTDIv (mGy) and DLP (mGy.cm).
 Figure 1: Bar Charts Showing Comparison of Scan Parameters of the Study Centres.
Figure 1: Bar Charts Showing Comparison of Scan Parameters of the Study Centres.
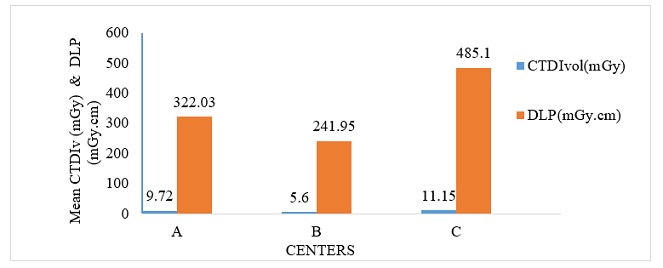 Figure 2: Comparison of Center Mean CTDIv (mGy) and DLP (mGy.cm) with their respective values.
Figure 2: Comparison of Center Mean CTDIv (mGy) and DLP (mGy.cm) with their respective values.
(Table 5) and (Figure 2) shows the combined mean of CTDIv as 8.82±2.54 mGy and DLP as 349.70±65.82 mGy.cm. The proposed local diagnostic reference level for chest CT examination of the region was 10.63 mGy and 414.70 mGy.cm with respect to CTDIv and DLP. Comparison of our DRL with that of international DRLs values was shown in (Table 6) and (Figure 3) respectively. European Commission [14] (10mGy) and Australia [15] had same values with our study in terms of CTDIvol (mGy). Our DRL value of 10.6 mGy in terms CTDIvol was comparable with the works of UK [16] (8.5mGy) and Japan [17] (13 mGy).
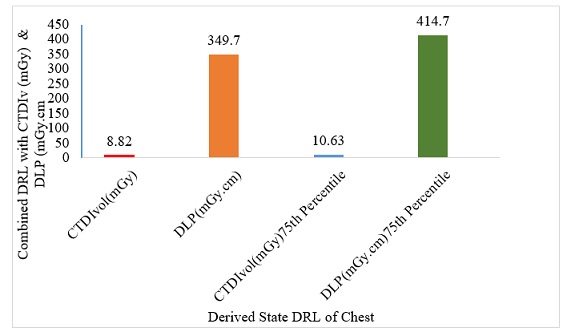 Figure 3: Comparison of Combined CTDIv (mGy) and DLP (mGy.cm) with their Derived State DRL.
Figure 3: Comparison of Combined CTDIv (mGy) and DLP (mGy.cm) with their Derived State DRL.
|
DRL |
Body Region |
Mean |
75th Percentile |
|
CTDIv (mGy) |
Chest |
8.82±2.54 |
10.63 |
|
DLP (mGy.cm) |
Chest |
349.70±65.82 |
414.7 |
Table 5: Combined Mean of CTDIv (mGy) and DLP (mGy.cm) with Derived State DRLs.
|
Body Region |
Authors |
Year |
CTDIv (mGy) |
|
Chest |
Present Study |
2023 |
10.6 |
|
Chest |
European Commission |
2014 |
10 |
|
Chest |
Australia |
2020 |
10 |
|
Chest |
Japan |
2020 |
13 |
|
Chest |
UK |
2019 |
8.5 |
Table 6: Comparison of Established DRLs in Terms of CTDIv (mGy) with International Values.
(Table 7) and (Figure 4), shows the table and comparison of our DRL in terms of DLP. (414.7 mGy.cm) being lower than the European Commission [14] (600 mGy.cm), and Japan [17] (510 mGy.cm), but comparable with Australia [15] (390 mGy.cm), and higher than UK [16] (290 mGy.cm). These lower doses obtained in our study is likely due to adherence to patient radiation protection principle of optimization in all the three diagnostic centers (Figure 5).
|
Body Region |
Authors |
Year |
CTDIv (mGy) |
|
Chest |
Present Study |
2023 |
414.7 |
|
Chest |
European Commission |
2014 |
600 |
|
Chest |
Australia |
2020 |
390 |
|
Chest |
Japan |
2020 |
510 |
|
Chest |
UK |
2019 |
290 |
Table 7: Comparison of Established DRLs in Terms of DLP (mGy.cm) with International Values.
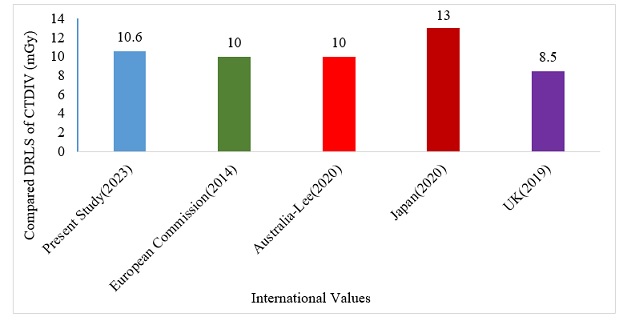 Figure 4: Comparison of our DRL in Terms of CTDIv with International Values.
Figure 4: Comparison of our DRL in Terms of CTDIv with International Values.
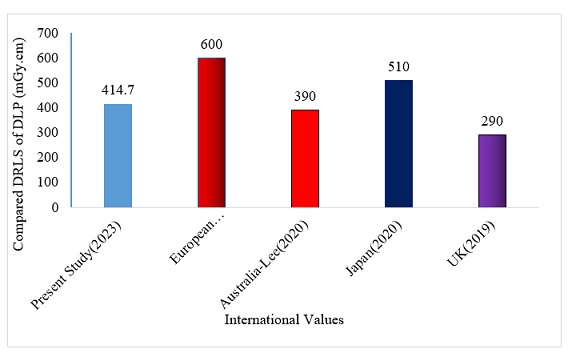 Figure 5: Comparison of our DRL in terms of DLP with International Values.
Figure 5: Comparison of our DRL in terms of DLP with International Values.
In Nigeria, some authors have established DRLs both locally as per state, and regionally as per geographical zones (Tables 8,9 and Figures 6,7). The results of our study were compared with the works of Buhari [18] from Northwest with CTDIv and DLP (17.25mGy/735mGy.cm) and percentage variation with our work as 21.7% and 21.4% respectively. In a similar study, in Northcentral, Rilwan et al., [19] obtained 10.9 mGy/432.8mGy.cm for CTDIv and DLP and variation with our work shows 13.7% and 12.6% respectively. In the same vein, Ogbole and Obed [20] in Southwest obtained 22.7 mGy/1189 mGy.cm with percentage variation of 28.6% and 34.7%. Also, Joseph et al., [21] carried out a similar study in Northeast with CTDIv and DLP values as 18 mGy/659 mGy.cm, and variation of 22.7% and 19.2% existed. Therefore, our established DRLs for chest examination in South-South region of Nigeria, was comparable with the work in North-Central Nigeria (Figure 6), but lower than the values obtained in North west, Southwest, and Northeast respectively (Figure 6). The third quartile value is chosen as an appropriate investigation level, on the grounds that if 75% of the CT centers can operate satisfactorily below this dose value, then the remaining 25% should be made aware of their considerably higher dose values and optimization should be initiated.
|
Body Region |
Authors |
Year |
Location |
CTDIv (mGy) |
|
Chest |
Ogbole & Obed |
2014 |
South-West, Nigeria |
22.7 |
|
Chest |
Joseph et al. |
2018 |
North-East, Nigeria |
18 |
|
Chest |
Buhari & Buhari |
2021 |
North-West, Nigeria |
17.25 |
|
Chest |
Rilwan et al. |
2020 |
North-Central, Nigeria |
10.9 |
|
Chest |
Present Study |
2023 |
South-South, Nigeria |
10.6 |
Table 8: Comparison of Established DRLs in terms of CTDIv (mGy) with Other Part of Nigeria Values.
|
Body Region |
Authors |
Year |
Location |
DLP (mGy.cm) |
|
Chest |
Ogbole & Obed |
2014 |
South-West, Nigeria |
1189 |
|
Chest |
Buhari & Buhari |
2021 |
North-West, Nigeria |
735 |
|
Chest |
Joseph et al. |
2018 |
North-East, Nigeria |
659 |
|
Chest |
Rilwan et al. |
2020 |
North-Central, Nigeria |
432.8 |
|
Chest |
Present Study |
2023 |
South-South, Nigeria |
414.7 |
Table 9: Comparison of Established DRLs in terms of DLP (mGy.cm) with Other Part of Nigeria values.
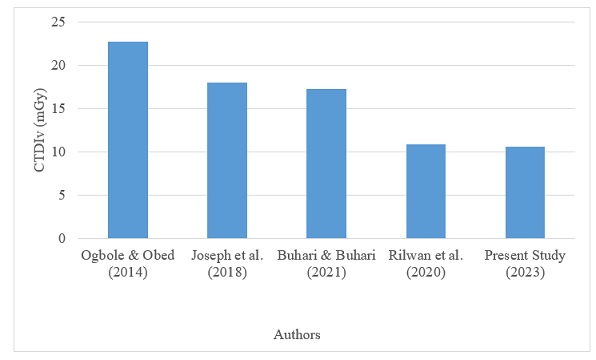 Figure 6: Comparison of our DRL in Terms of CTDIv (mGy) with Other Part Nigeria values.
Figure 6: Comparison of our DRL in Terms of CTDIv (mGy) with Other Part Nigeria values.
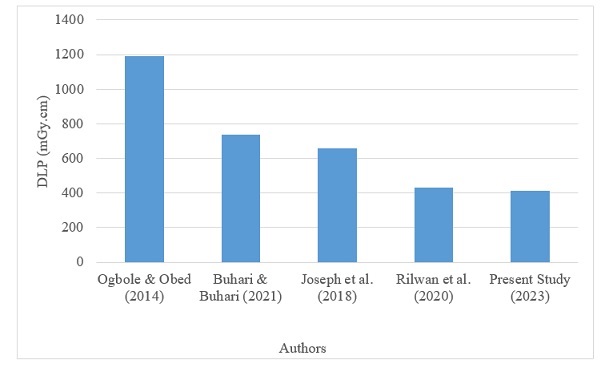 Figure 7: Comparison of our DRL in Terms of DLP with Other Part of Nigeria values.
Figure 7: Comparison of our DRL in Terms of DLP with Other Part of Nigeria values.
Conclusion
Local DRLs for chest CT examinations was proposed for Rivers State, South-South, Nigeria. The proposed LDRL were analogous or below other international works and Europeans Commission reports. Therefore, there is good patient dose optimization for chest CT examinations in the region studied.
Although the CTDIv obtained in this study is relatively similar to the internationally, locally and regionally reported data in the literature, and the DLP values is comparably lower than the European Commission reported value, but higher than data reported by some countries. Our result is intended for Preliminary Regional Diagnostic Reference Levels (PDRLs) for State studied. Also, variation between CT scan centers was observed. It is therefore recommended that the tube current and tube current time product be investigated and reduced, where possible so as to reduce the radiation absorbed dose. Also, the CT scan protocol for chest examination should be harmonized across all CT centers in Nigeria. Further recommendation is that an audit should be conducted in three (3) or (5) years’ time to establish revised LDRL that will be equal to or lower than the internationally established DRLs. There is also a need to determine the effective dose for patients undergoing chest CT examinations in the locality.
References
- Furlow B (2010) Radiation Dose in Computed Tomography. Radiologic Technology 22: 437-450.
- Brenner DJ, Hall EJ (2007) Computed Tomography an Increasing Source of Radiation Exposure. New England Journal of Medicine 357: 2277-2284.
- Vetter R (2008) ICRP Publication 103. The Recommendations of the International Commission on Radiological Protection. Health Physics 95: 445-446.
- Tanoue L (2009) Computed Tomography -An Increasing Source of Radiation Exposure. Year Book of Pulmonary Disease 34: 154-155.
- Brink J, Miller D (2015) US. National Diagnostic Reference Levels. Closing the Gap Radiology 277.
- Wallac AB (2010) The Implementation of Diagnostic Reference Levels to Australian Radiology Practice. J Med Imaging Radiat Oncol 54: 465-471.
- Huda W (2007) Radiation Doses and Risks in Chest Computed Tomography Examination. Proceedings of the American Thoracic Society 4: 316-320.
- ICRP (1991) Publication 60: 1990 Recommendations of the International Commission on Radiological Protection. Ann ICRP 21: 1-201.
- European Commission (2019) Guidelines on Quality Criteria for Diagnostic Radiographic Images European Commission EUR 16261 EN. European Commission, Europe.
- Goldman LW (2007) Principles of CT Radiation Dose and Image Quality. J Nucl Med Technol 35: 213-225.
- Karthikeyan D, Chegu D (2005) Step by Step CT Scan (A Practical Guide for Residents and Technologist). Jaypee Brothers Medical Publisher, New Delhi, India.
- Morin RL, Gerber TE, McCollough CH (2003) Radiation Dose in Computed Tomography of the Heart. Circulation 33: 917-922.
- European Commission (2014) Diagnostic Reference Levels (DRLS) in Thirty-Six European Countries. Radiation protection, European Commission, Europe.
- Lee KC, Beveridge T, Sanagou M, Thomas P (2020) Updated Australian diagnostic reference level for adult CT. J Med Radiat Sci 67: 5-15.
- UK Health Security Agency-RCE (2019) Doses from Computed Tomography (CT) Exams in the UK Review, UKHSA, England.
- Japan Medical Imaging and Radiological Systems Industries Association (2020) National Institutes for Quatum and Radiological Science and Technology. National Diagnostic Reference Levels in Japan 1-22.
- Buhari M, Buhari S (2021) Review of Diagnostic Reference Levels for Adult Patients Undergoing Chest and Abdomen Computed Tomography Scan in Northern Nigeria. African Journal of Environment and Natural Research 4: 83-90.
- Rilwan U, Sabiu LK, Umar I, Yusuf SD, Ugwu EI (2021) Assessment of Radiation Dose in Computed Tomography Examination of Adult Patient in Abuja and Keffi, Hospitals in Nigeria. Journal of Nuclear Medicine and Radiation Research 12: 1-7.
- Ogbole GI, Obed RI (2014) Radiation Doses in Computed Tomography: Need for Optimization and Application of Dose Reference Levels in Nigeria. West African Journal of Radiology 21: 1-6.
- Joseph DZ, Nzotta CC, Skam JD (2017) Diagnostic Reference Levels for Computed Tomography Examinations in North-Eastern, Nigeria. Pakistan Journal of Radiology 27: 364-369.
- Rilwan U, Onuchukwu GC, Sabiu LK, Abdullahi HA, Umar I (2020) Abdominal CT Dose Examination for Adult Patient in Abuja and Keffi, Hospitals in Nigerian. Asian Journal of Advanced Research and Reports 8: 36-44.
- Rilwan U, Onuchukwu GC, Umar I, Sabiu LK, Abdullahi HA (2020) Chest CT Dose Examination for Adult Patient in Abuja and Keffi, Hospitals in Nigerian. Asian Journal of Advanced Research and Reports 8: 1-9.
- Rilwan U, Onuchukwu GC, Abdullahi HA, Umar I, Sabiu LK (2020) Head CT Dose Examination for Adult Patient in Abuja and Keffi, Hospitals in Nigerian. Asian Journal of Advanced Research and Reports 9: 8-13.
- Abdullahi AH, Umar I, Taofeeq AI, Joseph DZ, Bello AA, et al. (2020) Assessment of Dose to Patients Undergoing Computed Tomography Procedures at Selected Diagnostic Centers in Kano, Nigeria. African Journal of Medical Physics 3: 23-28.
Citation: Ekwulugwo OP, Emenike OC, Bierechi OK, Ada MC, Usman R (2023) Assessment of Patients Radiation Doses during Computed Tomography Chest Imaging Examination: Propose Diagnostic Reference Level. J Nucl Med Radiol Radiat Ther. 7: 031.
Copyright: © 2023 Ojike Peter Ekwulugwo, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.