Auricular Myiasis in Children: Case report of Unexpected Foreign Bodie
*Corresponding Author(s):
Chaouki ADepartment Of Ent, University Hospital Centre IBN ROCHD, Central African Republic
Email:anasschaouki.ac@gmail.com
Abstract
Myiasis is the invasion and feeding on living tissues of humans or animals by fly larvae; The aural myiasisis not a common infestation, rare in adults but frequent in children with neglected chronic suppurative otorrhea and poor personal hygiene.
The most common pathological symptoms of aural myiasis are otalgia and otorrhea, the diagnosis is usually through physical examination, and rarely through diagnostic images. There are no published guidelines for diagnosis or treatment of this disease.
We report a case of a child with aural myiasis, living in a rural area in Casablanca morocco, with a maggot at the right ear; in treatment a combination of maggot extraction, Saline irrigation, concomitant suction and 3 mg of ivermectine were administrated with an encouraging results.
Keywords
INTRODUCTION
Auricular myiasis presents a rare and a unique clinical entity, it is rare in adults but frequent on among children; only a small number of case series have been reported [2]. Humans represent only a target of opportunity; it is frequent in rural and slum areas where unhygienic conditions are prevalent. Therefore, there is a Lack of available evidence to guide management of this disease [3]. We report a rare case of auricular myiasis on a child with immune deficiency history.
CASE REPORT
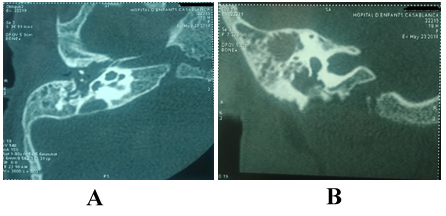
The girl has been referred to our ENT department for a complementary care management. The girl was admitted with the complaint of chronic otorrhea, otalgia and itching in the external auditory canal. The mother reported the extraction of maggots from the external auditory canal. CT scan showed a filling of the external auditory canal, middle ear and the mastoid cells without any bone lysis (Figure 1).
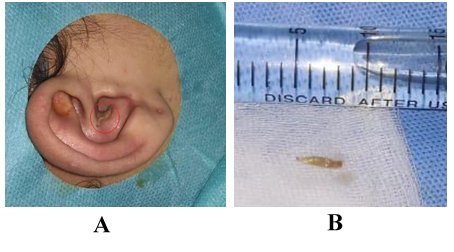
Upon examination with a general anesthesia, maggots showed at the middle ear after the aspiration of the draining right ear, with a large perforation. The maggots were extracted with clamp (Figure 2).
Saline irrigation and concomitant suction were performed. Combination antibiotic/steroid preparations were given pre- and post-micro toilet evacuation of the maggots, 3mg of ivermectine was administrated after extraction in one dose.
Maggot have been addressed in physiological saline at the parasitology laboratory and mycology, the myiasis was confirmed but fly species was not determined due to poor transport conditions, and the manipulated maggot. After 3 weeks follow up, the girl remained free of symptoms, and endoscopic examination showed the beginning of perforation closing (Figure 3).
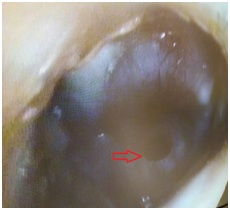 Figure 3: Clean extern auditory canal, with beginning of closing perforation.
Figure 3: Clean extern auditory canal, with beginning of closing perforation.DISCUSSION
Neglected chronic suppurative otorrhea was the most suspicious cause in our case. The clinical presentation is wide from maggots in the ear to otalgia, ear drainage, Perforation of drum, itching roaring sound, tinnitus, bleeding. Otalgia is the most common pathological symptom of aural myiasis, otorrhea may be the second frequent symptom. Severe infestation may lead to deafness and meningitis. The surrounding tissue of the ear canal including bones may be damaged by the larval attack [3,5]. The examination of auditory function before and after treatment will be necessary if the patient repot hearing loss.
In our case the symptoms were the otorrhea and maggots in the ear; auditory function was not examined by audiogram. Taxonomic division establishes several families derived from the order Diptera: Oestridae, Calliphoridae and Sarcophagidae are the most important. The species Wohlfahrtia magnifica, which belongs to the latter family, is a must-type larva, meaning that it requires living in a host tissue to complete its development. This species is the predominant etiologic agent worldwide [4,6].
In our population (morocco) sarcophagidae is the most frequent family [7], in our case fly species was not determined due to poor transport conditions. Singh and Rana (1989) reported that the identification of the species of maggot prior to the recommendation of treatment is important because not all types of myiasis are benign [5]; however in our case despite the lack of identification the outcomes were satisfactory.
After having diagnosed myiasis through physical examination and, in some cases, through diagnostic images, the treatment must begin as soon as possible, including removal of maggots and cleaning lesion with 70% ethanol, 10% chloroform, oil drops, iodine saline or normal saline. Prophylactic antibiotic therapy may prevent secondary infections. The treatment is simple in early stage [4,5].
According to literature, maggot’ sex traction, normal saline irrigation with concomitant suction and antibiotics were performed in our case. The ultimate goal of any treatment regimen is complete maggot removal and the easiest approach would likely be microscopic removal of all maggots with subsequent use of otic antibiotic drops [8]. Different studies have reported the occurrence of aural myiasis in humans [3], hence the interest of watchful waiting.
ETHICAL APPROVAL
REFERENCES
- Singh A, Singh Z (2015) Incidence of myiasis among humans-a review. Parasitology Research 114: 3183-3199.
- Jervis Bardy J, Fitzpatrick N, Masood A, Crossland G, Patel H (2014) Myiasis of the ear. Annals of Otology, Rhinology & Laryngology 124: 345-350.
- Maturo S, Captain U, Michaelson PG, Brennan J (2007) Auricular myiasis. Otolaryngology-Head and Neck Surgery 136: 668-669.
- Rodríguez Ruiz M, Acosta AM, Cifuentes Cardozo E, Chirveches M, Rosselli D (2018) Otomyiasis: systematic review. International Archives of Otorhinolaryngology 23: 104-109.
- Yuca K, Çaksen H, Sakin YF, Yuca SA, Kiri? M, et al. (2005) Aural myiasis in children and literature review. The Tohoku Journal of Experimental Medicine 206: 125-130.
- Jervis-Bardy J, Fitzpatrick N, Masood A, Crossland G, Patel H (2015) Myiasis of the ear: A review with entomological aspects for the otolaryngologist. Ann Otol Rhinol Laryngol 124: 345-350.
- Tligui H, Bouazzaoui A, Agoumi A, Otomyiases (2006) Humaines dues à Wohlfahrtia magnifica (Diptera : Sarcophagidae): A propos de trois observations au Maroc.
- Steve Maturo, et al. (2007) Auricular myiasis; Otolaryngology-Head and Neck Surgery.
Citation: Ballage A, Chaouki A, Beghdad M, Mkhatri A, Abada R, et al. (2019) Auricular Myiasis in Children: Case report of Unexpected foreign Bodie. J Otolaryng Head Neck Surg 5: 34
Copyright: © 2019 Ballage A, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.