Case Report of an Atypical Evolution of Urine Obstruction, is this Acute on Chronic Kidney Disease?
*Corresponding Author(s):
Rizo Topete LFellow Of The Internal Medicine Department, Hospital Christus Muguerza Alta Especialidad, UDEM, Monterrey, Nuevo León, Mexico
Tel:+52 1 81 8029 7718,
Email:marili18@hotmail.com
Abstract
Acute kidney injury (AKI), previously known as acute kidney failure, is defined as an abrupt (within hours) reduction of renal function in which both structural damage and loss of function are encompassed. Classification of AKI includes pre-renal, intrinsic kidney diseases (renal) and post-renal [1]. The term ‘acute-on-chronic renal failure’ has been used when AKI occurs in the background of pre-existing chronic kidney disease [2].
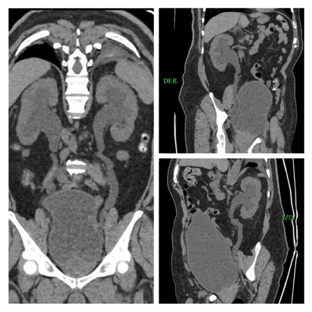
Post-renal AKI occurs after acute obstruction of the urinary flow, which increases intra-tubular pressure and thus decreases glomerular filtration rate. In addition, this acute obstruction generates an inflammatory process that contributes to the reduction of glomerular filtration. It can occur after an obstruction at any level of the urinary system (from the renal tubule to the urethra). The obstruction of the urinary tract is a common problem but a rare cause of AKI, currently there is no epidemiological data on its incidence, however it is more common in men and increases with age mainly due to prostate disease, pelvic cancer and urolithiasis [3,4]. The timing of the reversal of the obstructive cause is crucial because if not done in time can lead to permanent kidney damage. It is clear that complete or prolonged partial urinary tract obstruction can lead to tubular atrophy, interstitial fibrosis and, eventually irreversible renal injury [5]. Also is important to notice that obstruction of urinary tract may occur in the setting of preexisting Chronic Kidney Disease (CKD).
We present an atypical case (time of evolution) of a urinary obstruction with extremely high levels of plasmatic creatinine.
Keywords
CASE REPORT
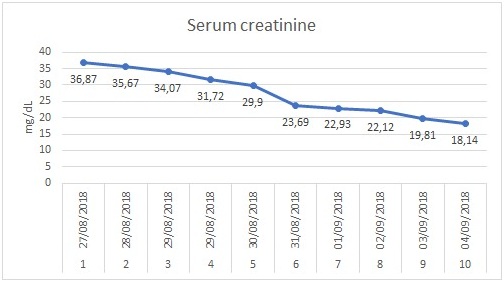
The patient’s obstruction was resolved on the first day of hospitalization with a urinary catheter but electrolyte abnormalities (hyperkalemia) persisted and hemodialysis was started.
DISCUSSION
There are no absolute criteria for when to initiate dialysis in these patients, but it is recommended to initiate before complications occur [6,9]. It is important to remember that the serum creatinine level does not correlate with Glomerular Filtration Rate (GFR) in a patient with AKI, so the clinical manifestations will govern the decision of renal replacement therapy. It is for this reason that in the beginning this treatment was not initiated in our patient, in spite of having a potassium greater than 6.5 mEq/L and urea greater than 30mEq/L because it did not cause significant electrocardiographic changes and was not accompanied with alterations in the mental status or symptoms of severe uremic encephalopathy however despite bladder catheterization, the hyperkalemia persisted and renal replacement therapy was decided to start.
CONCLUSION
REFERENCES
- Makris K, Spanou L (2016) Acute Kidney Injury: Definition, Pathophysiology and Clinical Phenotypes. Clin Biochem Rev 37: 85-89.
- Madala N (2007) Acute Renal Failure in Patients with Chronic Kidney Disease. African jornalOnline 25: 395-398.
- Bhandari S, Johnston P, Fowler RC, Joyce A, Turney JHN (1995) Non dilated bilateral ureteric obstruction. Nephrol Dial Transplant 10: 2337-2339.
- Chapman ME, Reid JH (1991) Use of percutanrousnehrostomy in malignan ureteric obstruction. Br J Radiol 64: 318-20.
- Blantz RC (1998) Pathophysiology of pre-renal azotemia. Kidney Int 53: 512-523.
- Lameire N, Van Biesen W, Vanholder R (2005) Acute renal failure. The Lancet 365: 417-430.
- Frokiaer J, Zeidel M (2011) Urinary tract obstruction. Brenner and Rector’s The Kidney 9. Elsevier. New York.
- Green J, Vardy Y, Minichor M, Better OS (1986) Extreme unilateral hydronephrosis with normal glomerular filtration rate: physiological studies in a case of obstructive uropathy. J Urol 136: 361-365.
- Better OS, Arieff AI, Massry SG, Kleeman CR, Mawell MH (1973) Studies on renal function after relief of complete unilateral ureteral obstruction of three month’s duration in man. Am J Med 54: 234-240.
Citation: De la Vega Méndez, Villarreal A, González P, Jímenez M, Topete R (2019) Case Report of an Atypical Evolution of Urine Obstruction, is this Acute on Chronic Kidney Disease?. J Nephrol Renal Ther 4: 022.
Copyright: © 2019 De la Vega Méndez FM, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.