Celiac Crisis in an Adult Patient: Case Report and Review of the Literature
*Corresponding Author(s):
Dimitrios Katsifis-Nezis1st Department Of Internal Medicine And Diabetes Center, Tzaneio General Hospital Of Piraeus, Piraeus, Greece
Tel:+30 6941405376,
Email:dimitris.katsifis@yahoo.com
Abstract
We report a case of celiac crisis in a previously healthy 51-year-old female presenting with a month’s history of diarrhea, cachexia and an abnormal metabolic panel.The patient’s diarrhea resolved after initiation of a gluten free diet and she gained 4 kilograms during hospitalization.
Celiac crisis is a very rare presentation of celiac disease in adults but nonetheless should be considered in patients with marked metabolic derangements in the setting of osmotic diarrhea.
Keywords
Celiac crisis; Celiac disease; Gluten free diet; Hypokalemia; Tissue transglutaminase
Introduction
Celiac Disease (CD) is an immune mediated inflammation of the small intestine caused by sensitivity to gluten and related proteins. Its prevalence ranges between 1:100 to 1:300 in most countries and manifests with a heterogeneous symptomatology [1]. Typical symptoms include chronic diarrhea and signs of malabsorption [2]. Celiac crisis is a fulminant manifestation of CD that presents with acute symptoms that often require hospitalization. It mainly affects pediatric patients under 2 years of age [3]. Due to its rarity in the adult population, with approximately 40 reported cases in the medical literature, clinicians need a high level of suspicion to recognize this clinical entity.
Case Presentation
A 51 years old woman was presented in the emergency department with a history of one month of diarrhea, accompanied by weight loss of 10 kilograms. The patient reported a frequency of 20 episodes of watery diarrhea per day with the absence of blood, mucus or steatorrhea. There was no history of fever, abdominal pain or recent travel abroad. She, also, denied any episode of night sweats or chills. She did not suffer from chronic illness or used any regular or illicit medication. Her family history was unremarkable.
At the objective examination she appeared cachectic and fatigued, but with normal awareness. Her skin turgor and jugular venous pressure were decreased and her mucous membranes dry. Auscultation of the lungs and heart was normal with respiratory frequency 15 breaths per minute. Blood pressure was found to be 85/75 mmHg, saturation of oxygen98% and heart rate 105 beats per minute. The rest of the examination was unremarkable.
Initial investigations revealed severe hypokalemia (K+: 1,8meq/L) and normal anion gap metabolic acidosis (PH: 7,30), consistent with the history of chronic diarrhea. Moreover, her serum sodium was 129 meq/L with urine sodium <5 mmol/L (hypovolemic hyponatraemia). The patient was treated with isotonic fluids and potassium intravenously and was admitted in the internal medicine department for further examination.
Additional laboratory examination indicated hypoalbuminemia (2.7 gr/dl), coagulopathy (INR: 4.4; APTT:55.9 sec) and positive tissue transgtlutaminase IgA antibodies (177U/ml). Stool examination did not suggest infectious etiology; neuroendocrine tumor work-up was negative while Computed Tomography (CT) of the upper and lower abdomen was free of pathological findings. Upper and lower endoscopies were performed and four biopsies were taken (stomach, duodenum and post bulbar duodenum). Histopathological exam describes increased intraepithelial lymphocytes, crypt hyperplasia and villous atrophy (Figure 1).
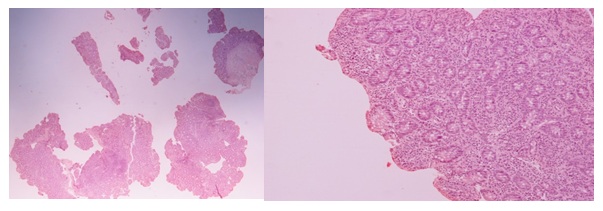 Figure 1: Increased intraepithelial lymphocytes, crypt hyperplasia and villous atrophy (H&E).
Figure 1: Increased intraepithelial lymphocytes, crypt hyperplasia and villous atrophy (H&E).
The biopsy results together with the positive serological marker of CD are consistent with the diagnosis of CD.
The patient was started on low calorie gluten free diet (500 kcal/day) and received vitamin B complex in order to prevent refeeding syndrome. She showed clinical and laboratory improvement with the episodes of diarrhea limited to 1-2 daily and gained 4 kilograms in 15 days. The patient got referred to the CD clinic of the same hospital.
Discussion
Celiac crisis is a rare and life-threatening form of CD fist described by Di Sant ‘Agnese in 1953 [4]. In 2010, Jamma and colleagues defined a celiac crisis as an acute presentation or rapid progression of gastrointestinal symptomatology, in CD patients, that requires medical attention [5]. Additionally, at least two of the following criteria have to be met.
- • Weight loss > 5 kg
- • Neurological symptoms
- • Increased creatinine > 2g/dl
- • Hypoalbuminemia <3.0 g/dl
- • Severe dehydration or shock
- • Metabolic acidosis (PH <7,35)
- • Electrolyte abnormalities
A recent review of the 42 reported cases described that, as CD, celiac crisis has a female predominance of 2:1. Furthermore, most of the patients (37/42) reported no past history of CD and their mean age of presentation was 50 years of age. Electrolyte imbalances, hypoproteinemia, metabolic acidosis and anemia were the most common abnormalities and the majority of patients indicated positive CD serology and advanced disease specific histopathological lesions (Marsh 3C stage) [6].
The present casefulfils five of the proposed criteria; weight loss of 10 kilograms, dehydration, severe hypokalemia/hyponatraemia, metabolic acidosis and hypoalbuminemia. Furthermore, it parallels the reported epidemiology of the disease as our patient was an otherwise healthy female of 51 years.
Moreover, although, not a part of the diagnostic criteria, bleeding diathesis has been identified in celiac crisis patients [6-7]. We, too, found an abnormal coagulation panel, most probably due to vitamin K malabsorption. This assumption is strengthened with the normalization of the laboratory values after the start of gluten free feeding.
Lastly, some reports suggest that celiac crisis is triggered by a preceding stimulus, such as surgery or infection [6,8]. In our case none was identified.
Celiac crisis is an easy to treat but severe presentation of CD. Due to its rarity it often is low or non-existent in the differential diagnosis of diarrhea in adult patients. We suggest that all patients, fulfilling some of the criteria proposed by Jamma and colleagues or having increased levels of CD-related antibodies, should be placed on gluten free diet and undergo to endoscopic examination of the small bowel.
References
- Gujral N, Freeman HJ, Thomson AB (2021) Celiac disease: prevalence, diagnosis, pathogenesis and treatment. World J Gastroenterol 18: 6036-6059.
- Rubio-Tapia A, Hill ID, Kelly CP, Calderwood AH, Murray JA (2013) ACG clinical guidelines: diagnosis and management of celiac disease. Am J Gastroenterol 108: 656-676.
- Babar MI, Ahmad I, Rao MS, Iqbal R, Asghar S, et al. (2011) Celiac disease and celiac crisis in children. J Coll Physicians Surg Pak 21: 487-490.
- Andersen DH, Di Sant'agnese PA (1953) Idiopathic celiac disease. I. Mode of onset and diagnosis. Pediatrics 11: 207-223.
- Jamma S, Rubio-Tapia A, Kelly CP, Murray J, Najarian R, et al. (2010) Celiac crisis is a rare but serious complication of celiac disease in adults. Clin Gastroenterol Hepatol 8: 587-590.
- Balaban DV, Dima A, Jurcut C, Popp A, Jinga M (2019) Celiac crisis, a rare occurrence in adult celiac disease: A systematic review. World J Clin Cases 7: 311-319.
- MagroR, Pullicino E (2012) Coeliac crisis with severe hypokalemia in an adult. Malta Medical Journal 24: 36-39.
- Hammami S, Aref HL, Khalfa M, Kochtalli I, Hammami M (2018) Refeeding syndrome in adults with celiac crisis: a case report. J Med Case Rep 12: 22.
Citation: Katsifis-Nezis D, Papazafiropoulou A, Vrakas S, Kampourogiani D, Kourkoulis P, et al. (2021) Celiac Crisis in an Adult Patient: Case Report and Review of the Literature. J Clin Stud Med Case Rep 8: 0116.
Copyright: © 2021 Dimitrios Katsifis-Nezis, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.