Clinical, Radiological and Evolutionary Aspects of Higher Grade of Injury of Subaxial Spine
*Corresponding Author(s):
Mualaba CélèbreDepartment Of Neurosurgery, Fann Teaching Hospital, Cheikh Anta Diop University, Dakar, Senegal
Tel:+221 1781310732,
Email:mualabcl01@gmail.com / mlbcelebre1@gmail.com
Abstract
Introduction: Higher grade of injury of the subaxial spine is any osteo-disco-ligamentary injury clinically classified as ASIA A and B, very often involving the functional and vital prognosis of the patient. In African literature, few works have attempted to focus on this problem. The objective of this study is to evaluate the prognosis of patients with high grade of cervical spine trauma.
Patients and methods: Over a 10-year period from 2009 to 2019, we retrospectively studied 48 records of patients followed in the neurosurgery department of the Fann University Hospital with higher grade of injury to the subaxial spine.
Results: Higher grade forms of subaxial spine injuries were frequent and represented 32% of subaxial spine injuries. The average age was 35 years with extremes of 16 to 60 years. We found predominance of males, with a sex ratio of 15, and falls were common cause. All patients presented a severe neurological, i.e. 81% classified as ASIA A. Associated injuries such as head trauma were observed in 6.25%. Surgical treatment was performed in 44%, by anterior approach in the majority. Mortality was high, at 79%. Only one patient had a complete recovery among the 10 survivorsafter 12 months of follow-up.
Conclusion: The improvement of the technical platform in the pre-hospital and hospital management of higher grade of injury of the subaxial spine and the creation of secondary neurosurgical care centers can improve the functional and vital prognosis. However, prevention remains the basis and constitutes the best treatment, while at the same time raising the awareness of the population.
Keywords
High grade; Subaxial spine; Trauma
Introduction
Trauma to the subaxial spine (ICS) represents all osteo-disco-ligamentary injuries involving the spine between the C2-C3 and C7-T1 discs.
"Highly mobile and poorly protected, the cervical spine is particularly vulnerable to trauma [1]. We speak of higher grade spinal injuries when the vital and functional prognosis is engaged. In our context, they concern patients classified as ASIA A or B and are mostly male and young [2,3]. Because they are more exposed to traffic accidents, which represent about half of the aetiologies, followed by falls and sports injuries [4].
Injuries to the subaxial spine are caused by multiple traumatic vectors. The diagnosis and management of spinal injuries must be early in order to limit the extension of the injuries. The African literature in general and Senegalese in particular, reports few works devoted specifically to the trauma of the subaxial spine with particular emphasis on their clinical, radiological and evolutionary fate. The objective of this work is to determine the epidemiological-clinical-radiological-evolutionary aspects of the so-called higher grade injury of the subaxial spine.
Patient and Methods
Over a period of 10 years, i.e. from 1 May 2009 to 1 May 2019, we retrospectively studied 48 files of patients followed in the neurosurgery department of the Fann University Hospital who had complained about trauma to the subaxial spine. We only included in this study patients who had suffered about higher grade trauma to the subaxial spine, i.e. patients classified as ASIA A and B. The study parameters were: frequency, age, sex, circumstances of the injury, time of admission, clinical (ASIA classification), imaging findings, type of treatment and outcome at 12 months based on the ASIA score and radiological findings. Data were analysed using SPSS version 20 software.
Results
During the study period, we recorded 150 cases of traumatic injury to the subaxial spine, of which 48 cases were classified as higher grade subaxial spine injuries, i.e. a frequency of 32%. The average age of the patients was 35±15 years, with extremes of 16 and 60 years. The age group most affected was between 26 and 45 years and represented 56%. The predominant sex was male, with a sex ratio of 15. Only 2 trauma patients were referred directly to the emergency department in our study setting, while 46 patients were referred from another health facility to our study setting. The conditions of collection and management at the trauma site were not specified. The admission time was greater than 10 hours in 85% of cases after the trauma. Among the 48 patients, 23 were victims of a fall (fall from a tree, fall from a height, fall from a car and fall from the second floor), 18 of road accidents and 7 of other types of accidents (3 patients were received after a wrestling match, 2 who had received a millet bag on the head, one diving accident and one patient had hit a wall (Table 1).
|
Circumstances of the Injury |
Number |
Percentage |
|
Falls |
23 |
48% |
|
Accidents on public roads |
18 |
38% |
|
Other causes |
7 |
14 |
|
Total |
48 |
100% |
Table 1: Distribution of patients according to the circumstances of the trauma.
According to the ASIA classification, ASIA A was predominant in 81.25% of cases, compared to 19% of ASIA B cases. Tetraplegia was the most frequent clinical presentation in the series in 39 cases (81.25%). Neurovegetative disorders were present in 9 cases, i.e. 18.75% of our patients, dominated by priapism in 5 cases and respiratory disorders in 4 cases.
Sphincter disorders accounted for 12 cases, 10 of which had constipation and 2 of which had sphincter disorders such as urinary retention or incontinence. Trophic disorders such as pressure sores were observed in 3 of our patients (6.25% of cases). Associated injuries and symptoms were present in 18.75% of cases. They were dominated by head trauma and skin wounds, respectively 6.2%. The 93.7% of patients in our series had vertebro-medullary lesions. Of these, 28 patients had disco-ligamentary lesions, i.e. 58.3% of cases, 15 patients had bone lesions, i.e. 31.2% of cases, 2 patients had mixed lesions and i.e. 4.2% of cases, and 3 patients had pure spinal cord lesions. The most common lesion levels were C4-C5 and C5-C6 with 24.4% and 37.8% respectively (Table 2).
|
Lesion Level |
Number |
Percentage |
|
C3-C4 |
6 |
13,3% |
|
C4-C5 |
11 |
24,4% |
|
C5-C6 |
17 |
37,8% |
|
C6-C7 |
6 |
13,3% |
|
C7-D1 |
5 |
11,1% |
|
Total |
45 |
100% |
Table 2: Distribution of patients according to lesion level.
Among the lesions, the most common were fracture-luxation followed by simple fracture with frequencies of 43.75% and 31.25% of cases respectively.
Spinal cord injuries represented 19 cases, i.e. 39.6% of the cases. Among these lesions, 16 were vertebro-medullary, i.e. 33.3%, compared with 03 pure spinal cord lesions of the contusion type, i.e. 6.25% of cases (Figure 1).
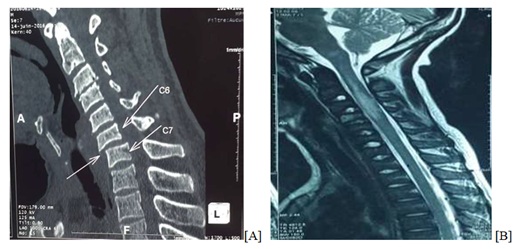 Figure 1: [A]: CT scan of the cervical spine showing C6-C7 subluxation with C6 anterolisthesis and C3-C4 disc pinch; [B]: Sagittal reconstruction of a cervical MRI showing a T2 sequence of spinal cord contusion (edematous) extending from C2 to C4.
Figure 1: [A]: CT scan of the cervical spine showing C6-C7 subluxation with C6 anterolisthesis and C3-C4 disc pinch; [B]: Sagittal reconstruction of a cervical MRI showing a T2 sequence of spinal cord contusion (edematous) extending from C2 to C4.
Pre-hospital care (pick-up, transfer conditions) was not specified. However, secondary transport was carried out by the health facility's ambulance. Surgery was the most common treatment in 21 cases (44%). Only one case had benefited from a posterior approach as opposed to almost all of the anterior approach and thus osteosynthesis by screwed plate. All patients received functional, bladder and bowel rehabilitation except for the patients who died early. The post-therapy evaluation of our series of 48 patients at 12 months’ follow-up found 10 patients who survived, i.e. 20.8%. These patients were re-evaluated neurologically using the ASIA score as (Table 3).
|
Post-Treatment Outcome at 12 Months Follow-Up |
Number |
Percentage |
|
ASIA A to ASIA B |
1 |
10 % |
|
ASIA A to ASIA C |
4 |
40% |
|
ASIA B to ASIA C |
1 |
10% |
|
ASIA B to ASIA D |
3 |
30% |
|
ASIA B to ASIA E |
1 |
10% |
|
Total |
10 |
100% |
Table 3: Distribution of patients according to post-treatment outcome.
Only one patient in the series made a full recovery, a 32-year-old who received a millet bag on the head causing a trauma to the cervical spine classified clinically as ASIA B on entry and whose CT scan of the cervical spine showed a vertebro-discal ligament injury of the fracture-luxation type; he underwent anterior surgery followed by a few sessions of motor physiotherapy which led to a full recovery after one year.
The average follow-up time was 12 months. The mortality of subaxial spine injuries in our setting was 79% of which 50% or 24 cases of deaths were ASIA A initially unoperated and 14 cases died postoperatively and the cause of death was related to neurovegetative disorders and decubitus complications. Thirty-four cases of death were initially classified as ASIA A with neurovegetative disorders at the beginning, the subjects aged over 60 years were practically all dead and death is considered as early if it occurs before one month of evolution, medium between one month and 6 months and late after 6 months. 35 cases were noted in our series to have died early, i.e. 72%.
Discussion
In Africa, there are few epidemiological studies that give an exact idea of the frequency of cervical spine injuries. During our study period, subaxial spine injuries represented 3% of all pathologies recorded in the department. The work carried out by [5], found a frequency of 2 to 3%, similar to ours, which suggests that cervical spine trauma remains an unexploited field in orthopaedic traumatology. The literature reports 35 years as the average age of occurrence of the trauma. The fact that young adults are the active segment of our society and therefore the most exposed, and the fact that they practice violent sports explains the occurrence of spinal injuries in our context [6-9].
By far the most common cause of cervical spine injuries in general is road traffic accidents as reported in the international literature [10-14]. The most frequent etiology is falls, which is why most of our patients were farmers with an increased risk of falling from a tree. But also the types of risky work like masonry without any form of protection. The delay between the occurrence of the trauma in the case of higher grade of spine trauma and the first treatment plays an important role in the outcome of the trauma patient. In our context, this long delay was explained by a failure of the emergency management system and the defective state of the roads in our environment. But also the inexistence of peripheral centers for neurosurgical care and management of cervical spine injuries in some regions of Senegal [15,16].
The ASIA (American spinal injury association) score remains the most widely used means of evaluating spinal trauma. The predominance of grade A explains the severity of spinal injuries in falls, which is the most frequent etiology in our study. Higher grade injury to the spine is associated with a severe neurological picture including genito-phincter disorders. Imaging in the context of spinal trauma is currently guided by certain decision trees such as those reported by some Canadian studies (NEXUS, CCR) [17], identifying the type of imaging to be requested.
Disco-ligamentary lesions are always the most frequent in cervical spine trauma; they are due to the fact that the slightest damage to the spinal cord during spinal trauma can be caused by a compressive bone fragment. Secondary injuries can also be observed, such as secondary spinal cord injuries defined by a cascade of events that affects the spinal cord originally spared by the impact and carries out a post-traumatic spinal cord self-destruction [18,19]. The limitation of these secondary injuries is at the origin of multiple studies in search of pharmacological agents capable of stopping this cascade of events [20,21].
The management of spinal trauma begins at the scene of the accident, with a one-piece pick-up, respecting the straightness of the head-neck-trunk axis, and installation in a shell. Medical transport by a team trained in emergency care remains the basis for preventing secondary traumatic injuries and charity fractures. In our environment, more than half of our patients have undergone a secondary transfer, i.e. 98% of the cases, because this transport is first carried out by the fire brigade towards the peripheral health structures which then refer them to the neurosurgical centers due to the lack of services capable of dealing with spinal injuries.
The type of injury guides the management of spinal trauma, which may be orthopaedic or surgical. The aim is to optimize the chances of neurological recovery by achieving decompression of neurological structures and to fix unstable injuries.
The subaxial spine can be approached by an anterior approach (the most used in our series), by a posterior approach or by a double or combined approach. The posterior approach was used for a long time, developed by ROY Camille [22]. Today, the anterior approach is the preferred method for the surgical treatment of cervical spine disorders, whether degenerative, traumatic, tumoral or vascular. It provides easy access to the injured disc/corporal region.
In our series, 42% of the patients operated on were approached from anterior versus 2% from posterior, and the mixed approach was not used. These results are comparable to those reported in the literature (Table 4) [23-25].
|
Authors |
Anterior approach |
Posterior approach |
Mixed approach |
|
E Kpelao5 |
18,8% |
65,7% |
- |
|
H Romulus13 |
85,9% |
12,8% |
1,3% |
|
P M Loembe9 |
72,2% |
23,5% |
4,3% |
|
M Batarbouch24 |
50,5% |
24,8% |
24,77% |
|
R Camille22 |
11% |
89% |
- |
|
B J Ordonez25 |
90% |
10% |
- |
|
Our series |
42% |
2% |
- |
Table 4: Distribution of patients according to the type of approach performed.
Historically, the popular treatment in France, following the work of R. Roy-Camille [22], is posterior plate osteosynthesis, aimed at stabilizing the injured underlying disc. If radiological control does not show satisfactory release of the canal, an anterior approach with excision-graft is used. Orthopaedic treatment consisted of reduction by traction followed by compression by a rigid cervical collar. Routine administration of corticosteroids in acute spinal injuries is not indicated according to studies conducted by the NASCI-II group [24].
The evolution of cervical spine trauma in general and the subaxial spine in particular is closely related to the initial neurological state; complete spinal cord injuries grade A have a very poor neurological improvement while incomplete injuries grade B have a better chance of recovery. But also the level of injury, as the case of neurological damage above C4 is accompanied by a very high number of deaths. This is because above C4 there is damage to the respiratory centers and the main breathing muscle (diaphragm) responsible for acute respiratory failure. Post-therapy follow-up of patients is still important.
At 12 months, of the 10 surviving patients, or 21% of cases, one patient had recovered completely. The remaining nine had made a partial recovery with one patient remaining ASIA B, five of the patients had progressed to grade C and three to grade D, all due to early functional rehabilitation. This functional rehabilitation is essential for a good professional reintegration and a maximum of personal independence, provided it is well conducted; however, it remains limited by the lack of financial means of the patients, the often very spaced out appointments do not allow an intensified rehabilitation with the aim of having a better chance of recovery of mobility. Another challenge is the non-availability of appropriate rehabilitation facilities in certain localities, which can compensate for this eventuality, and this remains a subject of reflection in the management of neurological disorders in Africa.
With all these problems linked to the lack of financial and material resources for the treatment of cervical spine injuries, Africa in general and Senegal in particular is obliged to promote the prevention of these injuries by optimizing awareness campaigns on public road accidents through the respect of the highway code and the education of the paediatric population on the risk of falls by climbing trees. As for workers, wearing appropriate safety equipment on construction sites remains the only way to limit the risk of spinal injuries.
Conclusion
The improvement of the technical platform in the pre-hospital and hospital management of serious trauma of the lower cervical spine and the creation of secondary neurosurgical care centers can improve the functional and vital prognosis to some extent. However, prevention remains the basis and constitutes the best treatment, while at the same time raising the awareness of the population.
References
- Olsen WL, Chakeres DW, Berry I, Richaud J (1992) Spine and Spinal Cord Trauma. In: Imaging of the spine and spinal cord. Raven Press, New York, USA.
- Amar AP, Levy ML (1999) Surgical reversals in the management of spinal cord injury. J Am Coll Surg 188: 550-566.
- Donald JW, Sadowsky C (2002) Spinal cord injury. Lancet 359: 417-425.
- Panjabi MM, White AA (1980) Basic biomechanics of the spine. Neurosurgy 7: 76-93.
- Kpelao E, Diop A, Beketi K, Tine I, Thioub M, et al. (2013) Challenge of the management of severe trauma of cervical spine in sub-developed country. Neurochirurgie 59: 111-114.
- Ziani I (2015) Current management of cervical spine trauma experience of the neurosurgery department of the hospital of specialties about 102 cases. Med thesis, Rabat.
- Mouhamed B (2019) Management of cervical spine trauma about 50 cases. Med thesis, Morocco.
- Fomba M (2008) Epidemiological and radiological aspects of cervical spine trauma in the orthopaedic and traumatological surgery department of the Gabriel Touré University Hospital. Med thesis, Bamako.
- Loembe P (1998) Fractures and dislocations of the lower cervical spine-therapeutic attitudes in Gabon. 45: 628-632.
- Karim K (2008) Trauma of the cervical spine in the orthopaedic and traumatological surgery department of the Gabrielle Touré University Hospital, about 45 cases. Thesis Med, Mali.
- Ntungwanayo S (2020) Severe trauma of the lower cervical spine in 126 cases. Dissertation for the residency in orthopaedics and traumatology, Dakar.
- Sow CM (1990) Recent trauma of the spine in 496 cases and 30 necropsies. MedThesis, Dakar.
- Houdenou R (2010) Trauma of the cervical spine in 136 cases. Med thesis, Fez.
- Sénégas J (1987) Trauma of the cervical spine. Encycl Med Chir, Appareil locomoteur.
- Robert O, Valla C, Lenfant F, Seltzer S, Coudert M, et al. (2002) Interest of standard radiographs of the cervical spine in the unconscious trauma patient. Ann Fr Anesth Réanim 21: 347-353.
- Habbab A (2016) Management of cervical spine trauma in the surgical intensive care unit: A case report. Med Thesis, Morocco.
- Saragiotto BT, Maher CG, Lin CWC, Verhagen AP, Goergen S, et al. (2018) Canadian C-spine rule and the National Emergency X-Radiography Utilization Study (NEXUS) for detecting clinically important cervical spine injury following blunt trauma. Cochrane Database of Sys Rev 4: CD012989.
- Dosch JC, Dieteman JL (2000) Spinal cord injury. Imagerie des urgences. Paris, France.
- Dusart I, Schwab ME (1994) Secondary cell death and the inflammatory reaction after dorsal hemisection of the rat spinal cord. Eur J Neurosci 6: 712-724.
- Ducker TB, Saleman M, Perot PL, Balentine JD (1978) Experimental spinal cord trauma, I: Correlation of blood flow, tissue oxygen and neurologic status in the dog. Surg Neurol 10: 60-63.
- Camille R, Saillant G, Laville C, Benazet JP (1992) Treatment of lesions of the lower cervical spine C3 to C7. Spine 10: 442-446.
- Fuentes JM, Benezech J, Lussiez B, Vlahovitch B (1986) Fracture-separation of the articular process of the lower cervical spine. Its relation to fracture-dislocation in hyperextension. Rev Chir Orthop Reparatrice Appar Mot 72: 435-440.
- Evaniew N, Noonan VK, Fallah N, Kwon BK, Rivers CS, et al. (2015) Methylprednisolone for the treatment of patients with acute spinal cord injuries: A propensity score-matched cohort study from a Canadian multi-center spinal cord injury registry. J Neurotrauma 32: 1674-1683.
- Batarbouch M (2004) Traumatisms of the lower cervical spine experience of the neurosurgery department of the IbnSina hospital between 1994 and 2002. Mouhamed V University, Faculty of Medicine and Pharmacy, Rabat.
- Ordonez BJ, Benzel EC, Naderi S, Waller SJ (2000) Cervical facet dislocation: Techniques for ventral reduction and stabilization. J Neurosurg 92: 18-23.
Citation: Ndiaye Sy EHC, Célèbre M, Ndour MM, Faye M, Sarr C, et al. (2021) Gastrointestinal Surgery in Tertiary Care Center during Pandemic: Single Surgeon, Single Center Experience. Archiv Surg S Educ 3: 028.
Copyright: © 2021 El hadji Cheikh Ndiaye Sy, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.