Comparison of Two Self-Myofascial Release Tools for Increasing Ankle Dorsiflexion Range of Motion
*Corresponding Author(s):
Justin M StanekSchool Of Kinesiology & Recreation, Illinois State University, United States
Tel:+1 3094385862,
Fax:+1 3094385559
Email:jmstane@ilstu.edu
Abstract
Background/Aim: Lack of Ankle Dorsiflexion (DF) mobility is common in both the athletic and general populations and is associated with a variety of lower extremity pathologies. Numerous techniques exist to improve range of motion (ROM) with often the goal of addressing soft-tissue tightness within the triceps surae. Self-myofascial release using instruments such as foam rollers, massage sticks and other hand-held rollers are common in health care and athletic settings. The purpose of this study was to compare the effectiveness of two self-myofascial release tools on improving ankle DF-ROM.
Methods: Thirty-eight participants (n=70 limbs) volunteered to participate and were randomly allocated to either the control (n=24), The Stick™ (n=23), or R8 Roller™ (n=23) group. Participants closed-chain DF ROM (standing and kneeling) were assessed at baseline and immediately post-treatment. Participants in the intervention groups performed 5 sets of 30 seconds of self-myofascial release while the control group participants sat quietly for 5 minutes.
Findings: Results showed both self-myofascial release tools significantly increased DF-ROM when compared to the control group, however, the R8 Roller™ demonstrated slightly higher gains.
Conclusion: A single-session of self-myofascial release is effective for improving both standing and kneeling DF-ROM. Clinicians and athletes should consider adding these instruments into their self-care.
Keywords
Flexibility; Manual therapy; Mobility; Rehabilitation
Introduction
Ankle Dorsiflexion (DF) Range of Motion (ROM) plays an important role in gait mechanics. Proper heel strike cannot occur if certain degrees of motion do not exist with dorsiflexion. Proper DF results in correct foot strike and contributes to injury prevention. Willems et al., suggested limited DF range of motion may put the foot in a position of greater plantarflexion, increasing the likelihood of injury because the joint is in a loose-packed position [1]. Poor DF also reduces the ability to utilize and apply power from the posterior chain muscles [2,3]. Previous research has suggested needing at least 10° of DF during the stance phase of walking gait [4] while closer to 30° of DF is reported while running in standard shoes [5]. An individual who lacks these degrees of motion increase the odds of injury to their ankles, lower legs, and knees [1,6-8]. Specifically, having less than 20-30° of closed chain ankle DF has shown to hinder normal gait and may cause compensatory gait patterns, leading to pathologic conditions [9]. Pathologies that have been associated with decreased DF ROM include genu recurvatum, excessive subtalar joint pronation, ankle sprains, medial tibial stress syndrome, Achilles tendinopathy, gastrocnemius strains, and anterior cruciate ligament injuries [9].
Loss of ankle mobility can be due to soft tissue tightness, joint tightness, and/or muscle weakness. Joint mobilizations can help increase joint mobility and muscle strengthening with select exercises targeting the muscles of the lower leg can reduce muscle weakness. Soft tissue tightness can be reduced through forms of stretching and/or self-myofascial release. Although there are many forms of stretching, multiple studies have shown that static stretching provides the best acute improvements in ankle dorsiflexion [10-13]. Similar studies have looked at the comparison of static stretching to self-myofascial release utilizing tools such as foam rollers, massage sticks, and other hand-held rollers [13-16].
Self-Myofascial Release (SMR) is a technique in which pressure is applied to the fascia by the individual using various tools such as balls, rods, foam rollers of various densities and massagers [15]. SMR is a popular technique utilized by healthcare professionals and active individuals due to the ease of use and effectiveness in ROM improvements. A systematic review by Cheatham et al. looked at the effects on the tissue with handheld massage sticks compared to high density foam rollers pre- and post-exercise [14]. They found that both foam rolling and roller massagers help improve joint ROM and pre and post exercise muscle performance [14]. A 2015 literature review found that both foam rolling and roller massage help in pre-exercise, muscle maintenance, and aid in recovery following exercise [17]. The study also found that roller massage is a valuable tool for individuals because it allows them to self-treat at any time and frequency that is convenient for them [17]. Popular roller massagers are The Stickä and, more recently, the R8 Rollerä. Most of the studies used in the systematic review and literature review reference The Stickä. There is limited to no research out there on the effects on ROM or performance using the R8 Rollerä. Therefore, the purpose of this study was to compare the acute effects of The Stick™ and R8 Rollerä, on DF ROM in physically active individuals. We hypothesized that the R8 Roller™ would show greater increases in ankle DF ROM than both The Stick™ and the control groups.
Methods
- Design
A randomized control, cross-sectional study design was used to examine the effects of self-myofascial release on improving DF ROM using the R8 Roller™ compared to The Stick™. The participants were required to visit the athletic training facility for one session. Participants were randomized into one of three groups using block randomization in order to keep groups balanced with block sizes of 3 (1, 2, 3, 1, 2, 3, etc.). Both limbs of the volunteers were screened for inclusion and in instances when the participant’s dominant and non-dominant limbs qualified, they were both allocated to the same group. Limb dominance was self-reported by each participant as the preferred kicking limb.
- Participants
Based on a power analysis with power=0.80 and α level =0.05, the estimated sample size for the study was 15 participants per group. Following the initial screening 38 participants (17 male, 21 female, age 23.78±3.5 years, height 172.9±9.26 cm, mass 74.38±16.06 kg) had at least one ankle qualify for the study. Inclusion criteria required participants to meet the minimum ACSM guidelines [18] for physical activity and to have a dorsiflexion measure of less than 34° on one or both ankles during the modified Weight Bearing Lunge Test (WBLT) [19,20]. Participants were excluded if they had a recent lower extremity injury (within the past 6 months), previous lower extremity surgeries, current treatment being done on the triceps surae, and prior use of the R8 Roller™ and/or The Stick™. All participants signed an informed consent form prior to participation, and the university’s institutional review board approved the study. Demographic data for the participants is presented in table 1.
|
Group |
n (limbs) |
Age (years) |
Height (cm) |
Weight (kg) |
|
|
|
|
Mean ± SD |
|
|
Control |
24 |
23.85 ± 3.87 |
173.1 ± 7.39 |
77 ± 15.34 |
|
Stick |
23 |
23.33 ± 3.39 |
170.18 ± 9.87 |
72.97 ± 18.5 |
|
Roller |
23 |
24.07 ± 3.82 |
175.44 ± 9.71 |
71.12 ± 14.01 |
|
All Participants |
70 |
23.78 ± 3.5 |
172.9 ± 9.26 |
74.38 ± 16.06 |
Table 1: Demographic Data by Group.
- Measurements
To determine study eligibility, the investigators measured closed chain DF ROM using a digital inclinometer (SmartTool Pro 3600; Swiss Precision Instruments, Inc, Garden Grove, CA) with the participant’s knee straight and knee flexed to 90° at the starting position. Previous research has shown this to be a reliable and valid method for assessing ankle ROM [21-24]. The rater aligned the digital inclinometer along the anterior crest of the tibia so that the proximal end was immediately distal to the tibial tuberosity and the distal end aligned along the tibial crest (Figures 1&2). The individual in this manuscript has given written informed consent to publish these photos. The angle of the tibia relative to the horizontal was measured and readings were recorded in degrees. The inter-rater reliability for the standing measurement was high with an inter-class correlation coefficient (ICC) of 0.96 (95% CI = 0.93, 0.98). The ICC for the kneeling measurement was 0.95 (95% CI = 0.92, 0.97).
To assess standing DF, each participant removed their shoes and positioned themselves with both hands on the wall in front of them. The participant placed the dominant foot on a tape line so that the second toe and center of the heel were directly over the tape. This was done to reduce subtalar joint pronation which has been shown to affect ankle DF [22]. The participant then leaned forward while maintaining full knee extension and heel contact with the ground (Figure 1). The non-dominant limb remained in a position to maintain balance and not restrict dorsiflexion of the dominant limb. The participant was instructed to lean forward until they first felt a stretch in their calf and/or when they felt their heel begin to rise. This measurement technique was used based on the resistance 1 (R1) principle of joint mobilizations. R1 is described as the first point of resistance felt by the examiner and occurs near the end of a joint’s ROM [20]. Next, three test trials were performed by the participant, returning to neutral between each measurement. The mean value of the three measurements was documented and used for data analysis. Measurements were then repeated on the non-dominant limb.
For the kneeling measurement, the participant was instructed to kneel on the opposite leg being tested with the test leg visually placed in 90° of hip and knee flexion. The participant placed their front foot on the tape line as stated above. The participant was then instructed to lunge forward while keeping their heel in contact with the ground and their foot in line with the tape. The participant was instructed to lunge forward until they first felt a stretch in their distal calf and/or the heel began to rise. The measurement was taken three times as stated above.
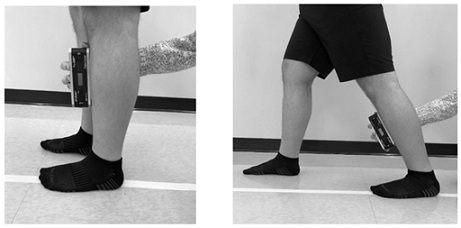 Figure 1: Standing weight bearing DF ROM start and end positions.
Figure 1: Standing weight bearing DF ROM start and end positions.
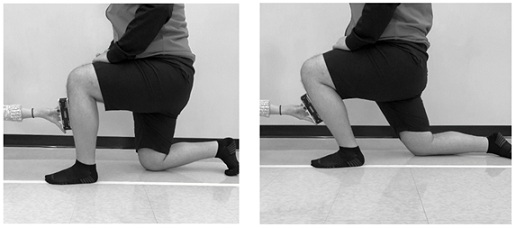 Figure 2: Kneeling weight bearing DF ROM start and end positions.
Figure 2: Kneeling weight bearing DF ROM start and end positions.
- Procedures
Participants met with the investigators to complete preparticipation questionnaires prior to beginning their first session. All procedures occurred at a single session for each participant. First, baseline ROM were performed as previously described to determine enrollment status. Qualifying limbs were randomly allocated to 1 of 3 groups: control, R8 Roller™, or The Stick™, using block randomization.
Upon reporting to the facility for their session, all participants were instructed to ride a stationary bike (moderate resistance) for 5 minutes in order to warm up the triceps surae. The clinician then educated patients on how to use the R8 Roller™ on the triceps surae based on the videos provided by the company [25]. R8 Roller™ participants then completed 5 sets of 30 seconds of rolling with 30 seconds rest between each set. During the first set, the participant used the roller on the medial and lateral aspect of the upper calf. The next set was over the medial and lateral aspect of the lower calf. The third set was over the posterior Achilles tendon. The fourth and fifth sets were over the posterior-medial and posterior-lateral aspects of the calf respectively. The Stick™ participants repeated the exact same procedures as the R8 Roller™, except they used The Stick™ instead of the R8 Roller™. Participants in the control group had their baseline measurements for DF ROM assessed. Upon allocation to the control group, these participants did the same stationary bike warm up for 5 minutes, sat quietly for approximately 5 minutes, and completed post-measurements. Following the assigned intervention, all participants had their ankle mobility re-assessed in both the standing and kneeling positions.
- Statistical analysis
To compare the effects of the interventions on DF ROM, change scores were calculated by subtracting the baseline measurement from the post-treatment measurement in the standing and kneeling conditions. Two, one-way ANOVAs were used to compare change scores across the 3 interventions for the standing and kneeling conditions. Differences identified by the ANOVA were assessed using Tukey post hoc tests. Effect sizes were calculated using the Cohen d and categorized as trivial (£0.20), small (0.21-0.49), moderate (0.50-0.79), or large (³0.80) [26]. The α level was set a priori at p < 0.05. All statistical analyses were performed using SPSS (version 22; IBM Corp, Armonk, NY).
Results
Preliminary testing was completed and revealed no difference between groups at baseline for the standing (p=0.23) or kneeling position (p=0.40). The means and standard deviations for all variables are reported in table 2. All limbs that were allocated to a group received the intended intervention and were analyzed post-treatment. Significant differences among groups were found in the standing (F2,31 = 7.18, p < 0.001) and the kneeling (F2,31 = 9.313, p = 0.001) positions. Post hoc analyses revealed significant differences between the R8 Roller™ and control (p=0.01, effect size=.94 95% CI: 0.34-1.54) and between The Stick™ and control (p = 0.02, effect size=.94 95% CI: 0.34-1.54) in the standing position. In the kneeling position, the R8 Roller™ had significant differences between the control (p = 0.001, effect size=1.19, 95% CI: 0.57-1.81) and The Stick™ had significant differences between control (p=0.03, effect size = .93 95% CI: 0.33-1.53). No significant differences were found between the R8 Roller™ and The Stick™ in either the standing or kneeling positions. No adverse reactions or unintended effects were reported by any participants.
|
|
|
|
Standing DF ROM |
|
|
|
|
Group |
n |
Baseline (°) |
Post-treatment (°) |
Change (°) |
P-value |
Effect size (95% CI) |
|
Control |
24 |
29.57 ± 5.16 |
29.64 ± 6.26 |
0.07 ± 3.79 |
n/a |
n/a |
|
Stick |
23 |
25.28 ± 6.27 |
28.51 ± 6.33 |
3.22 ± 2.82* |
0.02 |
0.94 (0.34-1.54) |
|
Roller |
23 |
24.93 ± 5.91 |
28.80 ± 6.23 |
3.87 ± 4.29* |
0.01 |
0.94 (0.34-1.54) |
|
|
|
|
Kneeling DF ROM |
|
|
|
|
Group |
n |
Baseline (°) |
Post-treatment (°) |
Change (°) |
P-value |
Effect size (95% CI) |
|
Control |
24 |
34.19 ± 4.64 |
37.33 ± 5.39 |
-0.42 ± 3.76 |
n/a |
n/a |
|
Stick |
23 |
35.84 ± 4.36 |
38.38 ± 3.81 |
2.54 ± 2.42* |
0.03 |
0.93 (0.33-1.53) |
|
Roller |
23 |
34.19 ± 4.64 |
38.54 ± 3.83 |
4.35 ± 4.26* |
0.001 |
1.19 (0.57-1.81) |
Table 2: Means and Standard Deviation by Group.
*indicates significant difference compared to control (P < 0.05).
Discussion
The purpose of this study was to examine the acute differences that may exist between two handheld SMR tools, the R8 Roller™ and The Stick™, on closed chain DF ROM. Based on our findings, the hypothesis was partially supported. The R8 Roller™ did not generate a significant increase in DF ROM compared to The Stick™ but did when compared to the control. Both devices appear to be equally effective at improving both standing and kneeling DF ROM. Applying both the R8 Roller™ and The Stick™ to the upper calf is relatively easy and likely comfortable for the participants. This could explain why no differences were found between the two devices in the standing position. The R8 Roller™ had slightly greater gains in ROM than The Stick™ in the kneeling position which could be attributed to the amount of pressure each device applied along the Achilles tendon. This is a sensitive area to roll over and The Stick™ requires people to apply the pressure. This subjective pressure could be limited due to sensitivity, whereas the R8 Roller™ has designed inserts to allow optimal comfort while providing a consistent spring-loaded roll over the intended area. The Stick™ is also only applying one point of contact against the Achille’s whereas the R8 can wrap around either side of the Achilles and allows two points of contact at any given time. To our knowledge, this is the first study examining the effectiveness of the R8 Roller on improving ROM.
Previous studies have found that roller massagers and foam rollers are effective tools for SMR to improve ROM [13,14,16,17,27,28]. There are thoughts that these tools have mechanical effects on fascia via its thixotropic properties, where the pressure on the fascia from rolling may allow it to become soft and lengthen, gaining more ROM [29-31]. Twomey and Taylor demonstrated that long-term mechanical stress application was required to induce a gel-like state [32]. Previous research has calculated that mechanical stress application forces of 24-115kg was high enough to cause such changes [33]. Using a handheld dynamometer and estimating a calf size with a circumference of approximately 40cm, we determined the springs alone on the R8 Roller provided approximately 11kg of force. It is unclear how much force participants in our study applied when using either the R8 Roller™ or The Stick™, however, it is possible the mechanical stress was sufficient to create change. Ge et al. found that IASTM not only has a mechanical effect, but also a neurological outcome as well. It alters the neural activities of mechanoreceptors with larger axons increasing 2-point discrimination [34]. Since IASTM has similar contact on soft tissue as roller massagers, it can be speculated that the roller massagers effect the mechanoreceptors in a similar manner. Schleip suggests immediate changes with the soft tissue are due to a neurological response, causing relaxation of the smooth or striated muscle fibers, which may also affect the metabolic ground substance within the immediate area [35].
Research has indicated the minimal detectable change (MDC) for closed-chain DF ROM ranges from 1.5-6.4° [23,36,37] and one study reported a specific MDC value of 3.8° [23]. Based on our data and using the formula for calculating MDC, (MDC = standard error of measurement x 1.96 x √2) our MDC values ranged from 1.32-1.41°. Conservatively, using the previously reported value of 3.8°, the R8 Roller™ achieved this change in both the standing and kneeling positions, however, The Stick™ did not. Further inspection of our data using the MDC of 3.8°, 11 (48%) ankles in the R8 Roller™ group exceeded the MDC, while 12 (52%) and 3 (12.5%) achieved this in The Stick™ and control groups respectively, for the standing position. Similar findings were also found in kneeling with 11 (48%) ankles in the R8 Roller™ group exceeding the MDC, whereas 9 (39%) and 3 (12.5%) achieved this in The Stick™ and control groups respectively.
We chose to have the cut off for ROM at 34°based off previous research which found having less than 30° [1] or 34° [38] is predictive of injury. The higher end of the range was our cutoff to avoid negatively affecting the number of potential participants that would qualify while still trying to prevent a ceiling effect. Previous research on DF ROM has stated a limitation with their study was using healthy participants that did not possess a DF ROM deficit, potentially limiting the amount of change [39].
Myofascial Release (MFR) has been used to treat soft tissue adhesions, alleviate pain, and reduce tissue tenderness, edema, and inflammation while improving muscle recovery [17,40]. Myofascial release demonstrated positive outcomes for increasing ROM and treating pain in a recent systematic review [41]. SMR is a technique similar to MFR where individuals use their own body weight on a foam roller or their upper body strength on a roller massager to exert pressures on the soft tissue. SMR eliminates the need for a clinician to provide MFR [17,42]. Smith et al., found that foam rolling and static stretching, combined, were more effective than static stretching alone and that foam rolling is more effective than static stretching on improving DF ROM [13].Similar research also found that foam rolling and static stretching combined had a 9.1% increase in DF ROM [16]. In a study done by de Souza et al., it was found that the use of a roller massagers on the calf provided an approximate 11% increase in DF ROM [28]. A similar study found that the use of a roller massager increased ankle ROM by about 4% compared to static stretching [43]. Our results found that the R8 Roller™ provided 15.5% change in standing and 12.7% in kneeling DF ROM. The Stick™ showed 12.7% and 7% changes while the control group showed 0.2% and 0.1% changes in standing and kneeling respectively. In busy health care settings, SMR has proven to be effective and time saving for clinicians, but it relies on the patient to perform the techniques correctly. Based on of our results, the R8 Roller™ and The Stick™ have the potential to provide similar ROM gains as hands-on, clinician intensive treatments.
- Limitations
As with any research investigation, this study had limitations. First, the participants were instructed to stop at the first point of tissue stretch and/or when they felt like their heel was going to lift off the ground during the ROM measurements. This point of limitation is subjective and can be interpreted differently amongst participants. However, the same instructions were repeated to the participant during each measurement session for consistency. Second, the pressure each participant applied while using The Stick™ could not be determined. Each participant was shown how to use The Stick™ and instructed to apply the maximum amount of pressure without eliciting pain. Since pain is subjective, the amount of pressure is subjective and may not match the pressure applied by the R8 Roller™. This could explain the slight differences found between the two. Finally, since the post-treatment measurements were taken right after each treatment, it is uncertain how long the increase in DF ROM may last. Our results are limited to acute responses in soft tissue from the treatment of both the R8 Roller™ and The Stick™.
Conclusion
The R8 Roller™ and The Stick™ both demonstrated immediate and significant increases in ankle DF ROM after one treatment in a population with deficits in DF. Based off the findings from this study, considerations should be made to utilize the R8 Roller™ or The Stick™ when aiming to improve DF ROM. Further research needs to be done to determine the long-term effects when comparing the R8 Roller™ to The Stick™ and/or the effects of multiple treatments while using the R8 Roller™ or The Stick™.
Funding
Authors received no funding for this work.
References
- Willems TM, Witvrouw E, Delbaere K, Mahieu N, Bourdeaudhuij ID, et al. (2005) Intrinsic risk factors for inversion ankle sprains in male subjects: a prospective study. Am J Sports Med 33: 415-23.
- Fong DT-P, Hong Y, Chan L-K, Yung PS-H, Chan K-M (2007) A systematic review on ankle injury and ankle sprain in sports. Sports Med Auckl NZ 37: 73-94.
- Nagano K, Uoya S, Nagano Y (2019) Effects of antagonistic muscle contraction exercises on ankle joint range of motion. J Phys Ther Sci 31: 526-529.
- Perry J, Burnfield J (2021) Gait Analysis: Normal and Pathological Function. J Sports Sci Med 9: 353.
- Sobhani S, Heuvel ER, Dekker R, Postema K, Kluitenberg B, et al. (2017) Biomechanics of running with rocker shoes. J Sci Med Sport 20: 38-44.
- Neely F (1998) Biomechanical risk factors for exercise-related lower limb injuries. Sports Med 26: 395-413.
- Wang HK, Chen CH, Shiang TY, Jan MH, Lin KH (2006) Risk-factor analysis of high school basketball-player ankle injuries: A prospective controlled cohort study evaluating postural sway, ankle strength, and flexibility. Arch Phys Med Rehabil 87: 821-825.
- You JY, Lee HM, Luo HJ, Lee CC, Cheng PG, et al. (2009) Gastrocnemius tightness on joint angle and work of lower extremity during gait. Clin Biomech 24: 744-750.
- Stanek JM, Pieczynski AE (2020) Effectiveness of clinician- and patient-applied mobilisation with movement technique to increase ankle dorsiflexion range of motion. Int J Ther Rehabil 27: 1-11.
- Jeon I, Kwon O, Yi C-H, Cynn H-S, Hwang U (2015) Ankle-Dorsiflexion Range of Motion After Ankle Self-Stretching Using a Strap. J Athl Train 50: 1226-1232.
- Behm DG, Blazevich AJ, Kay AD, McHugh M (2016) Acute effects of muscle stretching on physical performance, range of motion, and injury incidence in healthy active individuals: a systematic review. Appl Physiol Nutr Metab Physiol Appl Nutr Metab 41: 1-11.
- Medeiros DM, Martini TF (2018) Chronic effect of different types of stretching on ankle dorsiflexion range of motion: Systematic review and meta-analysis. The Foot 34: 28-35.
- Smith JC, Washell BR, Aini MF, Brown S, Hall MC (2019) Effects of Static Stretching and Foam Rolling on Ankle Dorsiflexion Range of Motion. Med Sci Sports Exerc 51: 1752-1758.
- Cheatham SW, Kolber MJ, Cain M, Lee M (2015) The effects of self-myofascial release using a foam roll or roller massager on joint range of motion, muscle recovery, and performance: A systematic review. Int J Sports Phys Ther 10: 827-838.
- Markovic G (2015) Acute effects of instrument assisted soft tissue mobilization vs. foam rolling on knee and hip range of motion in soccer players. J Bodyw Mov Ther 19: 690-696.
- Škarabot J, Beardsley C, Štirn I (2015) Comparing the effects of self-myofascial release with static stretching on ankle range-of-motion in adolescent athletes. Int J Sports Phys Ther 10: 203-212.
- Schroeder AN, Best TM (2015) Is self myofascial release an effective preexercise and recovery strategy? A literature review. Curr Sports Med Rep 14: 200-208.
- ACSM's National Center (2017) ACSM Guidelines for Exercise Testing and Prescription. Lippincott Williams & Wilkins, USA.
- Powden CJ, Hoch JM, Hoch MC (2015) Reliability and minimal detectable change of the weight-bearing lunge test: A systematic review. Man Ther 20: 524-532.
- Stanek J, Sullivan T, Davis S (2018) Comparison of Compressive Myofascial Release and the Graston Technique for Improving Ankle-Dorsiflexion Range of Motion. J Athl Train 53: 160-167.
- Munteanu SE, Strawhorn AB, Landorf KB, Bird AR, Murley GS (2009) A weightbearing technique for the measurement of ankle joint dorsiflexion with the knee extended is reliable. J Sci Med Sport 12: 54-59.
- Chisholm MD, Birmingham TB, Brown J, MacDermid J, Chesworth BM (2012) Reliability and Validity of a Weight-Bearing Measure of Ankle Dorsiflexion Range of Motion. Physiother Can 64: 347-355.
- Konor MM, Morton S, Eckerson JM, Grindstaff TL (2012) Reliability of three measures of ankle dorsiflexion range of motion. Int J Sports Phys Ther 7: 279-287.
- Hall EA, Docherty CL (2017) Validity of clinical outcome measures to evaluate ankle range of motion during the weight-bearing lunge test. J Sci Med Sport 20: 618-621.
- Roll Recovery (2021) R8 How to Calves. Education. Roll Recovery, USA.
- Cohen J (1988) Statistical power analysis for the behavioral sciences. Erlbaum Associates, USA.
- Curran PF, Fiore RD, Crisco JJ (2008) A comparison of the pressure exerted on soft tissue by 2 myofascial rollers. J Sport Rehabil 17: 432-442.
- Souza A, Sanchotene CG, Lopes CMS, Beck JA, Silva ACK, et al. (2019) Acute Effect of 2 Self-Myofascial Release Protocols on Hip and Ankle Range of Motion. J Sport Rehabil 28: 159-164.
- Barnes MF (1997) The basic science of myofascial release: morphologic change in connective tissue. J Bodyw Mov Ther 1: 231-238.
- Stemmans C, Sefton J (2004) Myofascial Release for Athletic Trainers, Part I: Theory and Session Guidelines. Athl Ther Today 9: 48-49.
- Sullivan KM, Silvey DBJ, Button DC, Behm DG (2013) Roller-massager application to the hamstrings increases sit-and-reach range of motion within five to ten seconds without performance impairments. Int J Sports Phys Ther 8: 228-236.
- Twomey L, Taylor J (1982) Flexion creep deformation and hysteresis in the lumbar vertebral column. Spine 7: 116-122.
- Threlkeld AJ (1992) The effects of manual therapy on connective tissue. Phys Ther 72: 893-902.
- Ge W, Roth E, Sansone A (2017) A quasi-experimental study on the effects of instrument assisted soft tissue mobilization on mechanosensitive neurons. J Phys Ther Sci 29: 654-657.
- Schleip R (2003) Fascial plasticity-A new neurobiological explanation, Part 1. J Bodyw Mov Ther 7: 11-19.
- Denegar C, Hertel J, Fonseca J (2002) The effect of lateral ankle sprain on dorsiflexion range of motion, posterior talar glide, and joint laxity. J Orthop Sports Phys Ther 32: 166-173.
- Cosby NL, Hertel J (2011) Relationships between measures of posterior talar glide and ankle dorsiflexion range of motion. Athl Train Sports Health Care 3: 76-85.
- Pope R, Herbert R, Kirwan J (1998) Effects of ankle dorsiflexion range and pre-exercise calf muscle stretching on injury risk in Army recruits. Aust J Physiother 44: 165-172.
- Rowlett CA, Hanney WJ, Pabian PS, McArthur JH, Rothschild CE, et al. (2019) Efficacy of instrument-assisted soft tissue mobilization in comparison to gastrocnemius-soleus stretching for dorsiflexion range of motion: A randomized controlled trial. J Bodyw Mov Ther 23: 233-240.
- Paolini J (2009) Review of Myofascial Release as an Effective Massage Therapy Technique. Hubbard T, editor. Athl Ther Today 14: 30-34.
- AJimsha MS, Al-Mudahka NR, Al-Madzhar JA (2015) Effectiveness of myofascial release: Systematic review of randomized controlled trials. J Bodyw Mov Ther 19: 102-112.
- MacDonald GZ, Penney MDH, Mullaley ME, Cuconato AL, Drake CDJ, et al. (2013) An acute bout of self-myofascial release increases range of motion without a subsequent decrease in muscle activation or force. J Strength Cond Res 27: 812-821.
- Halperin I, Aboodarda SJ, Button DC, Andersen LL, Behm DG (2014) Roller massager improves range of motion of plantar flexor muscles without subsequent decreases in force parameters. Int J Sports Phys Ther 9: 92-102.
Citation: Porter W, Anderson B, Stanek JM (2023) Comparison of Two Self-Myofascial Release Tools for Increasing Ankle Dorsiflexion Range of Motion. J Altern Complement Integr Med 9: 434.
Copyright: © 2023 Whitney Porter, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.