Correlation between Vitamin D Concentrations and Physical Activity in U.S. Children and Young Adults between Ages 5-15 Years
*Corresponding Author(s):
Rohitha GoonatilakeDepartment Of Mathematics And Physics, Texas A&M International University, Texas, United States
Email:harag@tamiu.edu
Abstract
The aspects of human health, behaviors and cognitive functions develop at the early stages of our life. This paper analyzes the correlation between vitamin D and physical activity in children and young adults (ages 5-15 years). A significant health association suggested that physical activity led to higher serum levels of 25-hydroxyvitamin D, (25(OH)D) in the human body. The relationship between self-reported physical activity and vitamin D as it correlates to the development of children and young adults among the U.S. population is extensively examined. The analysis is based on the data from participants in the Centers for Disease Control and Prevention (CDC) and U.S National Health and Nutrition Examination Survey (NHANES, 2013-2014). This paper also provides the existence of factors that influence the different levels of vitamin D in the human body and their relation to the population at large. This research is comprised of the collection of data from the CDC for public use, statistical analyses and findings using SAS statistical software.
Keywords
Calcium; Physical activity; Vitamin D; 25-hydroxyvitamin D (25(OH)D)
ABBREVIATIONS AND SAS IDENTIFIERS
- • 25(OH)D2+25(OH)D3 is aggregate of vitamin D occurs in 2 forms vitamin D2 (25(OH)D2 which is ergocalciferol) and vitamin D3 ( 25(OH)D3 which is cholecalciferol), and simply referred to as vitamin D2 and vitamin D3.
- • LBXVIDMS is 25OHD2+25OHD3 (nmol/L) (these two substances combine give out the levels of vitamin D levels in a body).
- • MINVIDEOGAME is minutes spent in videogames per week.
- • PAQ722 is any physical activities performed in the past 7 days (Yes/No).
INTRODUCTION
Vitamin D and calcium work together to protect bones and achieve ultimate results; perhaps against cancer, diabetes and high blood pressure [1]. Calcium is known to be a vital nutrient for our body, as bone mass depends on the levels of calcium present in our bodies. As intake of calcium increases, so does our bone mass. Thus, reduction of calcium in the human body is strongly correlated to loss of bone mass. Unlike many other vitamins, our bodies cannot store any surplus of calcium; the human body has as much as needed depending on calcium levels.
Furthermore, the bone mass loss is a strong determinant for the risk of osteoporosis [2]. For many years, research has been conducted to focus on how to decrease the bone loss that occurs as years pass by in one’s life [3]. When a balance is reached and proper bone mass is maintained under normal conditions, bone formation is coordinated through multiple levels of coupling mechanisms [4]. Bone minerals have also been important to recognize bone strength [5]. As stated in calcium in human health, “bone is the body calcium reserve” and exercise is directly related to bone mass during growth and for maintaining it during maturity [1]. As defined in calcium in human health, “physical activity is defined as any form of muscular activity that results in an increase in energy expenditure” [1]. Exercise is planned physical activity with the goal of maintaining a fit lifestyle, however, physical activity has also been found to increment the growth stimulation of bone [6]. An increase in muscle mass requires for one’s bones to adapt. However, even if one is taking enough calcium, if there is a deficiency in vitamin D, all calcium accumulated could go to waste. The human body needs vitamin D to effectively absorb calcium. The way to determine an individual’s vitamin D levels is through the measure of serum 25-hydroxyvitamin D concentrations (abbreviated as 25(OH)D) [2]. Although vitamin D does not decrease mortality risk, there are several studies that analyze how exercise in certain individuals produces higher levels of vitamin D [7]. While sunlight is the main source of vitamin D for many people, there are other ways to obtain vitamin D such as a nutritious diet and vitamin D supplements, thus providing the optimal levels of reviews associated with the study.
Vitamin D in the body
Vitamin D and calcium are critical for optimal development of children and young adults. Known as the sunshine vitamin, vitamin D is produced by the body most commonly by Ultraviolet (UV) light that the human body gets from exposure to the sun [8]. As a fundamental micronutrient, vitamin D is extremely essential for strong bones because it is the substance that helps the body use calcium that is received from diet. The best sources of vitamin D can be found in few foods such as fish, vegetables, eggs, dairy and some grain products [9]. As stated in a dietary reference, “the dietary sources of vitamin D include food and dietary supplements; therefore, total vitamin D intake reflects the combined dietary contribution from foods and supplements”. Pharmacology, vitamin D comprises a group of fat-soluble secosteroids accountable for a variety of biological effects. The two major groups are vitamin D2, which is a vitamin produced by the human body and the vitamin that is found in foods, and vitamin D3, which is found synthesized in the skin and is also consumed in animal-based foods [10]. Both vitamins, D2 and D3, can be found as dietary supplements and in foods. As previously highlighted, vitamin D is incorporated into the skin from exposure of ultraviolet radiation. The human body converts UV radiation and produces vitamin D, specifically vitamin D3 [11].
Vitamin D’s most prevalent function in the human body is calcium and a phosphate combination leading to mineralization of the bone [1]. Low levels of vitamin D are commonly found in elderly and show that poor muscle strength and weakness may be associated with the deficiency. As people get older, it is harder for the human body to allow skin to absorb 25-hydroxyvitamin D, 25(OH)D [12]. The impact of vitamin D depends on the stage of life that the individuals are at. In infancy, infants require adequate levels of vitamin D, as a deficiency could lead to skeletal deformities. It is recommended that infants that are fully breast-fed receive vitamin D supplements because breast milk has a low concentration of the vitamin. In contrast, commercial infant formula contains vitamin D [10]. While at the stage of childhood and adolescence it is important to maintain high levels of vitamin D as it is a stage that is characterized by bone accretion. During this stage, almost 50 percent of adult bone mass will be accumulated [6]. The levels that are considered normal for vitamin D in the human body are 20 ng/ml; anything lower than that is considered vitamin D deficiency [13]. For children, pediatricians use less than 25 nmol/L to define vitamin D deficiency in their patients, and considered that anything greater than 50 nmol/L is beneficial for children [14]. As mentioned before, 25(0H)D levels are important in the body because the hormones promote calcium absorption and lead to induction of synthesis of calcium transport and to regulate either indirectly or directly bone mineralization [15].
There are certain factors to take into consideration when looking at the numbers of synthetization of vitamin D, such as season of the year, skin pigmentation, and household income [16]. First off, there is a clear difference in sunlight exposure levels during the winter months and that of the summer months, leading to a variation in the amount of vitamin D absorbed. During summer months, children and adolescents are known to spend more time in recreational activities and/or taking advantage of enjoying a day out. This affects the body by obtaining higher exposure to UV light. However, during the wintertime, the weather usually is an impediment to 1) enjoying outdoor recreational activities and 2) whenever one can engage in outdoor activities, thus UV light is not as strong as in the summer. Next, the effect this has on vitamin D is that the rate of production is lower. When it comes to skin pigmentation, there is a relationship between the skin pigmentation and the capacity to produce vitamin D [17]. It is believed that higher skin pigmentation prevents UV exposure in contrast to individuals that have lighter pigmentation where UV light penetration is more commonly found. NHANES survey found that serum levels are highest in whites, lowest in non-Hispanic blacks and intermediate in Hispanic groups. Then, socio-economic status is also taken into consideration when looking at vitamin D levels, mainly because of the differences in individual’s diets. A low socio-economic status may prevent families from having a good and balanced diet that may not include the common food groups containing the vitamins [18]. Low-income families could also face some difficulty in obtaining vitamin D supplements when other needs are deemed more important. The probability that someone from middle-upper class is able to have a balanced diet and can afford supplements is much higher.
Physical activity and vitamin D
As stated by Jennifer White, “low levels of physical activity are particularly detrimental to bone density in children” [19]. The increment of physical activity helps to prevent loss of bone mineral density. Physical activity not only increases bone size but also bone strength [20]. It is well recognized that physical activity has a positive effect on health. It is believed that 20 to 30 minutes of physical activity outdoors can increase vitamin D levels and that two to three times of sun exposure in a week is enough to achieve healthy vitamin D levels in the summer [21]. Physical activity helps control body fat percentages, and, in turn, aids in vitamin D absorption [19]. It has been showed that there is an association between vitamin D levels and difficult health outcomes, which is why it is believed there is an association between physical activity and vitamin D levels [22]. Obese children and youth are less active than leaner peers and therefore this can negatively affect their levels of vitamin D because of two reasons. Firstly, a child that is obese most likely does not have a balanced diet that provides adequate nutrients and therefore is not able to obtain vitamin D levels from food [23]. Secondly, as previously mentioned, vitamin D levels are obtained primarily from sunlight exposure. The higher the body fat concentration in children, the harder it is for UV light to penetrate the skin [24]. This can lead to vitamin D deficiency among the population. However, a mixture of physical activity and a well-balanced diet can reduce body fat percentage. It is also important to take into consideration the effects that exercise has on skeletal health. As acknowledged therein, vitamin D levels help to absorb calcium effectively. Research conducted by Bar-Or highlighted that “cross-sectional comparisons have shown that young athletes in weight-bearing sport” [25]. Thus such as gymnastics, soccer and volleyball have a higher Body Mass Density (BMD) than do non-athletesis leads to the conclusion that when higher physical activity rates are achieved, the higher it is for children and young adults to obtain bone build up and bone mass. Young vitamin D-deficient individuals may not be able to healthily develop bones. The same study suggested that all adolescents should perform some form of physical activity either daily or nearly every day as there is a possible association between adult health and health behavior in previous years [25].
METHODOLOGY AND ANALYSIS
Information obtained from the U.S. National Health and Nutrition Examination Survey includes the data from individuals from ages 1-79 years of age, from Mexican American, Hispanic, Non-White Hispanic and Non-Hispanic Black origins [17]. A group of 9,813 females and males from NHANES survey were examined. NHANES reflected a continuous and standardized data collection based on a representative sample of the U.S. population and provides critical diet and health measures for federal program planning and policy making. NHANES is unique because it collects and tracks health measures from a national sample of Americans and provides an important aspect of the nation’s health monitoring system. This questionnaire breaks down into self-reported physical activity and includes the individual activity questions which included details about the type of physical activity respondents engaged in. Furthermore, individual activities were categorized as "indoor" and "outdoor" based on a discussion with experts that are familiar with the physical activity habits in the U.S. In this analysis, variables that were considered were gender, age, race, socio-economic status, Body Mass Index (BMI) and gender was categorized as male and female and their ages ranged from 5 to 15 years. Race was categorized as Mexican American, other Hispanic, Non-White Hispanic, and Non-Hispanic Black, and other. Socioeconomic status was categorized by ranges of annual household incomes. Season of when the questionnaire conducted was also taken into consideration as a six-month period during November-April 2013 and May-October 2014 [17]. BMI was categorized as normal if BMI < 25 kg/m2, overweight if 25 kg/m2 ≤ BMI ≤ 30 kg/m2, and obese if BMI ≥ 30 kg/m2 [26].
The analysis of the research was carried out through the basis of correlation, regression analysis, t-test, Chi-square test and ANOVA model using statistical programming SAS®. SAS® is a software suite developed by SAS Institute for advanced analytics, multivariate analyses, business intelligence, data management and predictive analytics. A linear regression was used to model the association between physical activity and vitamin D levels in children and young adults between the ages of 5-15 years. Self-reported physical activity times were reported in minutes per day in different categories such as indoors and outdoors [17]. Time spent in a 30-day period was also examined. Time that children and young adults spent watching TV and playing video games was considered. Additionally, tables and figures are provided denoting the sample size and the respective vitamin D concentration among the subjects of the study and statistical analyses is carried out.
The data presented in table 1, shows that the sample size of children between the ages of 5-15 years that participated in the questionnaire was 1,788 among a total of 9,813 surveyed. Of which 52% were male and 48% were female. When looking at the race of participants provided in table 2, it is shown that 25% were Mexican American origin, 10% other Hispanics, 26% Non-Hispanic White, 25% Non-Hispanic Black and 14% were from another race. The six-month period was examined to see any deficiencies between months when the questionnaire was taken. Table 3 depicts the breakdown between November 1, 2013 through April 31, 2014 when the children and young adults took the questionnaire. There were 857 participants from May, 2014 through October 30, 2014. The annual household income provided in table 4, presents that approximately 779 children and young adults live in a household where the annual household income is below the U.S. median household income level, $25,000-$34,999. Next, from BMI between individuals between the ages 5-15 years, 62 were underweight, 1,045 were normal, 327 were overweight and 354 obese. When looking at the correlation between total vitamin D levels and physical activity, the activities were selected based on the physical activities that are practiced while in exposure to the sunlight. It is known that 25 (OH) vitamin D total, (25 (OH) D2 + 25 (OH) D3) is the best measure of the stores and status of vitamin D [27]. Parameters for the linear regression model show that LBXVIDMS 25(OH)D2+25(OH)D3 (of course, measured in nmol/L) can be a linear function depending on the amount of hours using the computer or being outside of school over a 30-day timespan per day. Any physical activity in the last 7 days, participation in school sports, physical activities during school days, hours watched TV or videos over a 30-day timespan per day are provided in table 5. It can be observed in table 6 that there exists a correlation for 25(OH)D2+25(OH)D3 from hours of watching TV or video games, to any physical activity during the last 7 days, or participating in school sports. A correlation analysis for 25(OH)D2+25(OH)D3 between the six-month period, vitamin D intake, BMI and annual household income in table 7 shows that the assumptions were correct in determining factors that influence levels of vitamin D. The Chi-square test was performed for minutes spent in video games per week and vitamin D levels, the null hypothesis was that MINVIDEOGAME and LBXVIDMS are independent. From the results in table 8, the null hypothesis was rejected to conclude that minutes spent playing video games and vitamin D levels are dependent from each other. However, 100% of the cells have an expected count less than 5. In this instance, the Chi-square may not be a valid test. Additionally, the Chi-square test provides a special consideration in the deliberations because of its robustness. Any statistical test that works even after the stipulated assumptions are violated is considered a robust test. Research shows that the “rule of 5 or more expected frequencies” is too stringent or restrictive for inference purposes, even though practically a set of data can be collected to meet these requirements [28]. Figure 1 shows the differences between physical activity and 25(OH)D2+25(OH)D3, the distribution of LBXVIDMS - PAQ722 is symmetric, or at least exhibiting symmetry. The paired samples, 25(OH)D2+ 25(OH)D3 and physical activity, assuming the characteristics about data 1) the two groups are paired, and 2) there are no significant outliers in the difference between the two related groups. Finally, the normality, the difference of pair follows a normal distribution, thus making an ideal situation for the paired sample t-test to be administered. Figure 2, helps us observe that there is a statistical significance between vitamin D concentrations of individuals that performed any physical activity. The output from ANOVA analysis conducted for LBXVIDMS with PAQ722 as shown in table 9. LBXVIDMS is related to 25(OH)D2+25(OH)D3 and PAQ722 for any physical activity in the last 7 days. From ANOVA overall analysis, it can be observed that there is a statistically significant difference between the groups means of 25(OH)D2+25(OH)D3 and physical activity. Figure 3 provides the vitamin D concentration measured against minutes per week of rigorous recreational activity. The correlation analysis was applied in several outdoor activities to see if they had a correlation with vitamin D levels. It can be observed that physical activities such as walking, bike riding, running and track & field have a positive correlation with levels of 25(OH)D2+25(OH)D3 as provided in table 10.
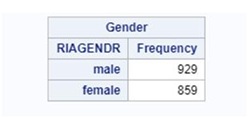 Table 1: RIAGENDR is assigned to gender.
Table 1: RIAGENDR is assigned to gender.
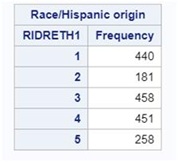 Table 2: Variable RIDRETH1 is assigned To Race/Hispanic origin (1 is for Mexican American, 2 Other Hispanic, 3 Non-Hispanic White, 4 Non-Hispanic Black, 5 Other Race).
Table 2: Variable RIDRETH1 is assigned To Race/Hispanic origin (1 is for Mexican American, 2 Other Hispanic, 3 Non-Hispanic White, 4 Non-Hispanic Black, 5 Other Race).
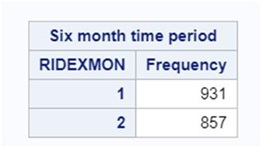 Table 3: RIDEXMON is assigned six-month time period (1 is for November-April 2013, 2 May-October 2014).
Table 3: RIDEXMON is assigned six-month time period (1 is for November-April 2013, 2 May-October 2014).
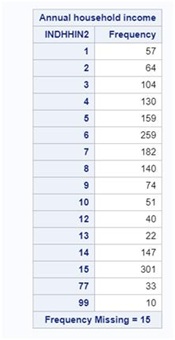 Table 4: Variable INDHHIN2 is assigned to annual household income (1 for $0-$4,999, 2 for $5,000-$9,999, 3 for $10,000-$14,999, 4 for $15,000-$19,999, 5 for $20,000-$24,999, 6 for $25,000-$34,999, 7 for $35,000-$44,999, 8 for $45,000-$54,999, 9 for $55,000-$64,999, 10 for $65,000-$74,999, 12 for $20,000 and over, 13 for under $20,000, 14 for $75,000-$99,999,15 for $100,000 and over, 77 for refused to answer, 99 for stated don’t know).
Table 4: Variable INDHHIN2 is assigned to annual household income (1 for $0-$4,999, 2 for $5,000-$9,999, 3 for $10,000-$14,999, 4 for $15,000-$19,999, 5 for $20,000-$24,999, 6 for $25,000-$34,999, 7 for $35,000-$44,999, 8 for $45,000-$54,999, 9 for $55,000-$64,999, 10 for $65,000-$74,999, 12 for $20,000 and over, 13 for under $20,000, 14 for $75,000-$99,999,15 for $100,000 and over, 77 for refused to answer, 99 for stated don’t know).
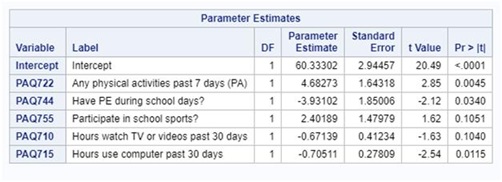 Table 5: Parameters for the linear regression model for LBXVIDMS vs. PAQ722, PAQ744, PAQ755, PAQ710, PAQ715.
Table 5: Parameters for the linear regression model for LBXVIDMS vs. PAQ722, PAQ744, PAQ755, PAQ710, PAQ715.
LBXVIDMS is for 25(OH)D2+25(OH)D3, PAQ722 for any physical activity in the past 7 days, PAQ744 for have physical activity during school days, PAQ755 for participation in school sports, PAQ710 for hours spent watching TV or videogames in the last 30 days, PAQ715 for hours spent using the computer in the last 30 days.
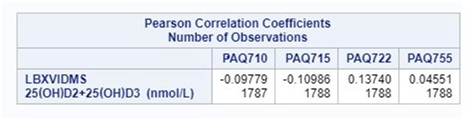 Table 6: Correlation analysis for 25(OH)D2+25(OH)D3 includes hours watching TV or playing videogames using the computer outside of school, any physical activity during the last 7 days, and participating in school sports.
Table 6: Correlation analysis for 25(OH)D2+25(OH)D3 includes hours watching TV or playing videogames using the computer outside of school, any physical activity during the last 7 days, and participating in school sports.
LBXVIDMS is for 25(OH)D2+25(OH)D3, PAQ710 for hours spent watching TV or videogames in the last 30 days, PAQ715 for hours spent using the computer in the last 30 days, PAQ722 for any physical activity in the past 7 days, and PAQ755 for participation in school sports.
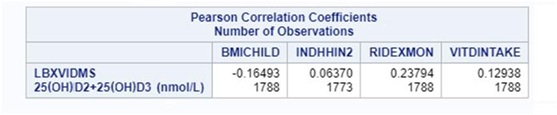 Table 7: Correlation Analysis for 25(OH)D2+25(OH)D3 with, six-month period, vitamin D intake, BMI and annual household income.
Table 7: Correlation Analysis for 25(OH)D2+25(OH)D3 with, six-month period, vitamin D intake, BMI and annual household income.
LBXVIDMS is for 25(OH)D2+25(OH)D3, BMICHOLD for levels of BMI in each individual, INDHHIN2 for annual household income of family for each children, RIDEXMON for six month period (November-April 2013 and May-October 2014.), VITDINTAKE for total vitamin D intake.
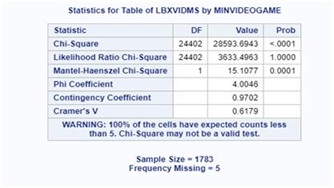 Table 8: Chi-square test for minutes spent playing video games per week against vitamin D levels.
Table 8: Chi-square test for minutes spent playing video games per week against vitamin D levels.
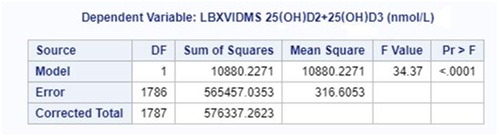 Table 9: ANOVA analysis for LBXVIDMS with PAQ722.
Table 9: ANOVA analysis for LBXVIDMS with PAQ722.
LBXVIDMS is for 25(OH)D2+25(OH)D3 and PAQ722 for any physical activity in the last 7 days.
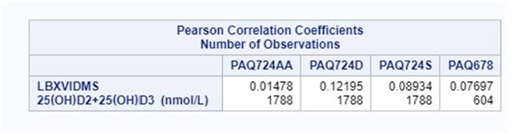 Table 10: Correlation for specific outdoor sports.
Table 10: Correlation for specific outdoor sports.
PAQ724AA for walking, PAQ724D for bike riding, PAQ72AS for running and PAQ678 for track and field.
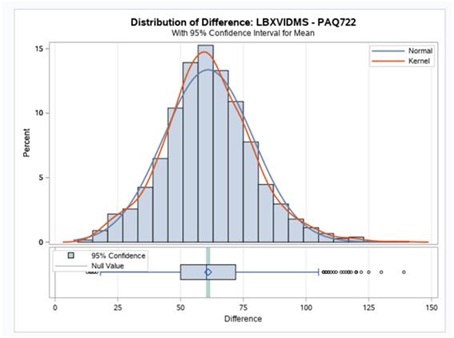 Figure 1: Distribution of difference between 25(OH)D2+25(OH)D3 and any physical activity (LBXVIDMS is for 25(OH)D2+25(OH)D3 levels and PAQ722 for any physical activity in the last 7 days).
Figure 1: Distribution of difference between 25(OH)D2+25(OH)D3 and any physical activity (LBXVIDMS is for 25(OH)D2+25(OH)D3 levels and PAQ722 for any physical activity in the last 7 days).
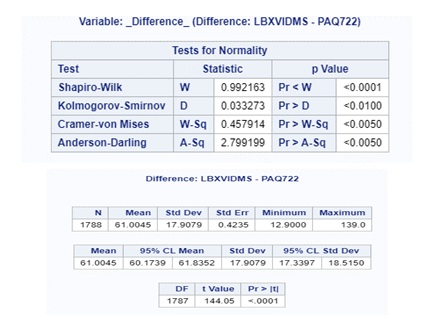 Figure 2: Paired sample t-test results for 25(OH)D2+25(OH)D3 vs. physical activity.
Figure 2: Paired sample t-test results for 25(OH)D2+25(OH)D3 vs. physical activity.
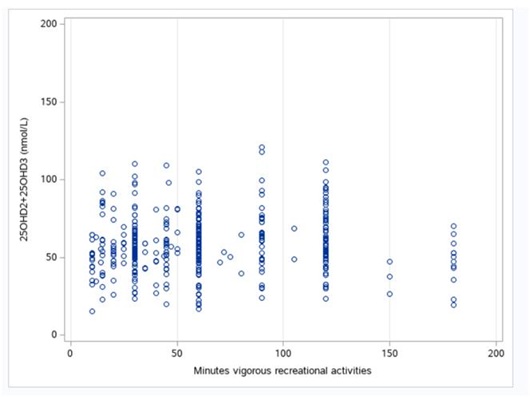 Figure 3: Vitamin D concentrations according to minutes per week of rigorous recreational activity.
Figure 3: Vitamin D concentrations according to minutes per week of rigorous recreational activity.
CONCLUSION
At the outset, it is emphasized that this study is primarily focused on outdoor activities that are significantly correlated with the levels of vitamin D. As a vitamin that “acts like a hormone,” vitamin D plays a long-recognized role in calcium targeting bone. It protects against multiple sclerosis rheumatic disorders, diabetes, high blood pressure, and cardiovascular diseases [9,29]. Vitamin D can be obtained in a well-balanced diet or can be synthesized in the skin from exposure to ultraviolet sunlight (UV light). Several factors influencing the levels of vitamin D are found in the human body, such as skin pigmentation, race, age, season and socioeconomic status. Because of these factors, vitamin D deficiency has been observed in children and young adults. The results show that the positive association between physical activity and vitamin D levels was strong enough to believe that physical activity leads to higher serum levels of 25-hydroxyvitamin D in the human body thus, to be able to conclude that the physical activity is positively correlated with higher levels of vitamin D and its metabolites. From the linear regression model obtained earlier, that there is a greater impact for vitamin D2 and vitamin D3 when individuals participate in school sports rather than spend hours watching TV or video games. Among all physical activities considered in the study, the participants who had significantly greater levels of vitamin D were those who participated in outdoor sports. This is explained through the correlation of bodily exposure to sunlight and vitamin D. The Chi-square test shows that the longer children spend playing video games the lower their vitamin D levels are. Further research could be conducted to explore correlation between physical activity and vitamin D levels in adults who self-reported physical activity in early stages of their lives. As observed during the six-month period, BMI and annual household income play a role in the levels of vitamin D among children and young adults. Though, in another attempt, using the three ranges for the time spent on video games per week with Low: 0-75 minutes, Moderate: 80-360 minutes, and High: 420-3,360 minutes against levels of vitamin D2 and vitamin D3 divided into Low: 13.90-35.30 nmol/L, Moderate: 35.50-67.00 nmol/L, and High: 67.20-140.00 nmol/L, the Chi-square test provides a statistically significant association between time spent playing on video games and levels of vitamin D2 and vitamin D3 as supported by table 11.
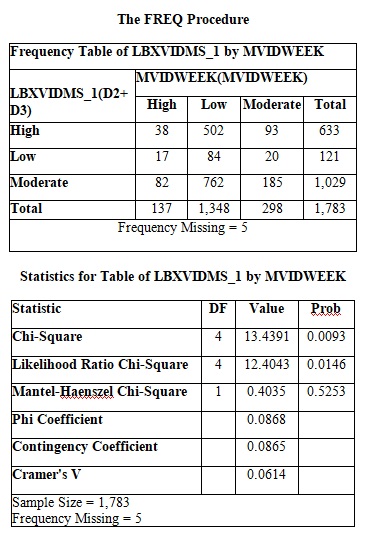 Table 11: Chi-square test for minutes spent playing video games per week and vitamin D levels using categories: low, moderate, and high.
Table 11: Chi-square test for minutes spent playing video games per week and vitamin D levels using categories: low, moderate, and high.
ACKNOWLEDGEMENTS
The first author would like to thank Dr. Carlos H. Orces M.D., M.P.H., F.A.C.P for helping throughout this project, guiding along and providing the support. Would also like to thank Dr. Rohitha Goonatilake for mentoring and guiding with the manuscript. More importantly, it is an immense opportunity being able to collaborate with Dr. Carlos H. Orces to make this research project possible for a publication. Additionally, Ms. Sofia C. Maldonado and Ms. Karina N. Flores assisted us in the many revisions of the draft for us to bring this manuscript to the current form, and they are greatly appreciated for their support.
REFERENCES
- Weaver CM, Heaney RP (2006) Calcium in human health. Humana Press, USA.
- Holick MF (2008) Deficiency of sunlight and vitamin D. Bmj 336: 1318-1319.
- Bunout D, Barrera G, Leiva L, Gattas V, Maza MPDL, et al. (2006) Effects of vitamin D supplementation and exercise training on physical performance in Chilean vitamin D deficient elderly subjects. Exp Gerontol 41: 746-752.
- Zhang L, Chen X, Wu J, Yuan Y, Guo J, et al. (2016) The effects of different intensities of exercise and active vitamin D on mouse bone mass and bone strength. J Bone Miner Metab 35: 265-277.
- Lerner V, Miodownik C (2012) Vitamin D deficiency. Nova Science, Hauppauge, USA.
- Carter CW, Micheli LJ (2012) Beyond Weight Control: The Benefits of Physical Activity for Children. Pediatr Ann 41: 493-493.
- Bolland MJ, Grey A, Reid IR (2014) Vitamin D supplements do not reduce mortality risk. BMJ 348: 2860.
- Cheetham CH, Freaney R, Mckenna MJ, Nashef L, Lamb E, et al. (1999) Vitamin D deficiency. BMJ 318: 1284-1284.
- Constantini NW, Hackney AC (2013) Endocrinology of physical activity and sport. Humana Press, New York, USA.
- Institute of Medicine (US) Committee to Review Dietary Reference Intakes for Vitamin D and Calcium (2011) Dietary Reference Intakes for Calcium and Vitamin D. National Academies Press, Washington DC, USA.
- Mead MN (2008) Benefits of Sunlight: A Bright Spot for Human Health. Environ Health Perspect 116: 160-167.
- Venning G (2005) Recent developments in vitamin D deficiency and muscle weakness among elderly people. BMJ 330: 524-526.
- Coney P, Demers LM, Dodson WC, Kunselman AR, Ladson G, et al. (2012) Determination of vitamin D in relation to body mass index and race in a defined population of black and white women. Int J Gynaecol Obstet 119: 21-25.
- Thurston A, Bowring C, Shaw N, Arundel P (2015) Vitamin D and bone health: A practical clinical guideline for management in children and young people in the UK. Bone Abstracts. 4: 88.
- Schoenmakers I, Pettifor JM, Peña-Rosas JP, Lamberg-Allardt C, Shaw N, et al. (2016) Prevention and consequences of vitamin D deficiency in pregnant and lactating women and children: A symposium to prioritise vitamin D on the global agenda. J Steroid Biochem Mol Biol 164: 156-160.
- Pearce SH, Cheetham TD (2010) Diagnosis and management of vitamin D deficiency. BMJ 340: 5664.
- Centers for Disease Control and Prevention (CDC) (2014) NHANES 2013-2014. CDC, USA.
- Feldman D, Pike JW, Adams JS (2011) Vitamin D Two-Volume Set. Academic Press, Pg No: 2144.
- White J, Flohr JA, Winter SS, Vener J, Feinauer LR, et al. (2005) Potential benefits of physical activity for children with acute lymphoblastic leukemia. Pediatr Rehabil 8: 53-58.
- Fausto-Sterling A (2008) The Bare Bones of Race. Soc Stud Sci 38: 657-694.
- Lanteri P, Lombardi G, Colombini A, Banfi G (2013) Vitamin D in exercise: Physiologic and analytical concerns. Clin Chim Acta 415: 45-53.
- Wanner M, Richard A, Martin B, Linseisen J, Rohrmann S (2015) Associations between objective and self-reported physical activity and vitamin D serum levels in the US population. Cancer Causes Control 26: 881-891.
- Uusi-Rasi K, Patil R, Karinkanta S, Kannus P, Tokola K, et al. (2017) A 2-Year Follow-Up after a 2-Year RCT with Vitamin D and Exercise: Effects on Falls, Injurious Falls and Physical Functioning Among Older Women. J Gerontol A Biol Sci Med Sci 72: 1239-1245.
- Patil R, Karinkanta S, Tokola K, Kannus P, Sievänen H, et al. (2015) Effects of Vitamin D and Exercise on the Wellbeing of Older Community-Dwelling Women: A Randomized Controlled Trial. Gerontology 62: 401-408.
- Bar-Or O (1995) Health Benefits of Physical Activity during Childhood and Adolescence. PsycEXTRA Dataset.
- Bislev LS, Rødbro LL, Rolighed L, Sikjaer T, Rejnmark L (2018) Effects of Vitamin D3 Supplementation on Muscle Strength, Mass, and Physical Performance in Women with Vitamin D Insufficiency: A Randomized Placebo-Controlled Trial. Calcified Tissue International 103: 483-493.
- Nasim B, Al Sughaiyer HM, Abdul Rahman SM, Inamdar B, Chakaki R, et al. (2019) Efficacy of Vitamin D3 versus Vitamin D2 in deficient and insufficient patients: An open-label, randomized controlled trial. Ibnosina J Med Biomed Sci 11: 57-61.
- Cochran WG (1954) Some methods of strengthening the common χ^2-tests. Biometrics 10: 417-451.
- Wang H, Chen W, Li D, Yin X, Zhang X, et al. (2017) Vitamin D and Chronic Diseases. Aging and disease 8: 346-353.
Citation: Espinoza LP, Orces CH, Goonatilake R (2020) Correlation between Vitamin D Concentrations and Physical Activity in U.S. Children and Young Adults between Ages 5-15 Years. J Med Stud Res 3: 018.
Copyright: © 2020 Lorna P Espinoza, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.