Cross-Cultural Adaptation, Validation, and Reliability of the Michigan Hand Outcomes Questionnaire: Arabic Version
*Corresponding Author(s):
Aliaa F KhajaDepartment Of Trauma And Orthopedics, Al Razi Orthopedic Hospital, Kuwait City, Kuwait
Tel:+965 66135777,
Email:aliaa.khaja@gmail.com
Abstract
Background: Michigan Hand Outcomes Questionnaire (MHOQ) is a patient-reported hand-specific questionnaire representing outcomes.
Objectives: The purpose of this study was to translate the MHSQ into Arabic and investigate its psychometric properties by testing the internal consistency, reliability, validity, and floor/ceiling effects.
Materials & Methods: 57 patients participated in this survey. The internal consistency tests were performed using Cronbach’s alpha. Spearman’s Correlation was calculated to estimate construct validity in comparison to DASH. Also, the Bland-Altman Plot was used to investigate the proportional bias between DASH and Arabic MHSQ.
Results: Arabic MHS had a Cronbach’s alpha of 0.85, which was very high and reliable. All subscales of MHSQ had an internal consistency higher than 0.70. Furthermore, a strong correlation with DASH score was observed (r=0.771, p<0.001), which suggests a good construct validity. DASH had a statistically significant correlation with all MHSQ subscales. it indicates especially high correlation with Hand function (r=0.701; p<0.001), activity of daily life (r=0.761; p<0.001) and pain score (r=-0.620; p<0.001). No relevant ceiling and floor effect was observed among the responses.
Conclusion: Overall, the Arabic version of MHSQ proved to be a good and reliable diagnostic tool for patients with hand injuries.
Keywords
Arabic; Michigan Hand Outcomes Questionnaire; Psychometric; Reliability; Validity
INTRODUCTION
The hand is a complex limb consisting of the bones, muscles, nerves, tendons, arteries, veins, and ligament [1]. It is important that the upper limbs and the hands be in good form, both structurally and functionally, to enable an individual perform daily activities with convenience and without hindrance. Impairments such as musculoskeletal or neurological injuries to the upper limbs and the hands could have a negative impact on their functioning. Injuries also have a negative impact on the patient’s life, including leisure, work, and activities of daily living. For long, occupational therapy has focused on the ability to function independently and effectively [2]. Occupational therapists bear the responsibility of dealing with people experiencing hand injuries to assist them regain maximum usage and capability of the hands [3]. As such, it has become necessary to employ important tools and outcome measures for the assessment of the efficacy of hand rehabilitation programs [3]. Two major types have been put forward, namely, self-reported outcome measures and performance-based outcome measures [3]. Performance-based outcome measures include the Minnesota Manual Dexterity Test and the Jesben hand Function test. Both tools require the patient to carry out certain functional tasks. Contrastingly, self-reported outcome measures require the completion of questionnaires by the patient, rating their performance on a set of predetermined functional tasks [3]. Self-reported outcome measures employed in hand rehabilitation include the Disabilities of the Arm, Shoulder and hand (DASH) questionnaire, the Canadian Occupational Performance Outcome Measure (COPM), as well as the health-related quality of life-Short Form 36 (SF 36) [3]. Without a doubt, the accuracy of performance-based outcome measures may present a more accurate representation of the patient’s ability, but then self-reported information by the patient is equally important: their feelings and thoughts about their hands after sustaining injuries. By combining the patient’s subjective information on the actual performance, an occupational therapist will have a more holistic view of the patient with hand injuries. The Michigan Hand Outcomes Questionnaire (MHQ) is an example of a self-reporting outcome measure commonly used for the assessment of hand injuries [4]. The MHQ was developed in 1998 and has become a very essential tool for the measurement of health status domains, activities of daily living, overall hand function, aesthetics, work performance, and satisfaction [4]. The Michigan Hand Outcomes Measure comprises 37 items with rating scales ranging 1 to 5. Every single domain is scored and converted to values that range from 0–100 [4]. A high score indicates better results, with the exception of pain in which a high score indicates a more intense pain. It can measure the level of impairments on either side of the hand [5]. The responsiveness and validity of the MHQ has determined for various hand conditions [4]. It has also been translated into several languages like Dutch, Chinese, Japanese, German, and Thai [6,7]. The MHQ is yet to be translated to Arabic. And so, to learn more about Arabic patients with hand injuries, it is the aim of this study to translate the MHQ into Arabic and investigate its reliability and validity.
Disabilities of the Arm Shoulder and Hand (DASH)
The DASH questionnaire is made up of 30 unique items, all self-reported by patients and designed specifically for measurement of symptoms and physical functions in patients experiencing musculoskeletal disorders of the upper limbs [8]. The objective of DASH is to describe the disability that patients with upper limb disorders experience and to observe symptom changes as well as changes in functions over time following treatments [9]. DASH has proven to be a reliable tool for use by physicians in the investigation of joints in the upper extremities. Each item has a score ranging from 0 to 4. The total score is calculated by adding the scores of all rated items (0–120). Finally, the total DASH is reversed to match the majority of the MHS subscales.
MATERIALS AND METHODS
Translation
Translation was done as per recommendations of Guillemin's guidelines for validation and cross-cultural adaptation [10] after permission obtained from the original MHQ copyright holder. Two Bilingual orthopaedic surgeons were responsible for the conceptual and literary translation of the original MHQ. Two other versions were produced by independent translation companies with a background in scientific English. All the versions produced were similar. Modifications to incorporate from all the versions were made and implemented in the final version. A professional Arabic grammar checker reviewed it. The back-translation came close to the original score. A pilot test was then conducted on 10 random patients from the hand clinics, after the Arabic version was approved by the translation committee. Both the physicians interviewed the patients after completing the questionnaire to address any issues or need for assistance.
Participants
A total of 57 patients with hand disorders participated in this study. The inclusion criteria were age 18 years or older, the ability to read and write Arabic with ease, and at least 3-week duration of symptoms. Patients who were not able to fill out the forms, with major neurologic disorders or with elbow or shoulder problems were excluded from the study.
PSYCHOMETRIC PROPERTIES AND DATA ANALYSIS
Internal consistency
The outcome measures of each construct were presented using descriptive analysis. Mean and Standard Deviation (SD) were calculated. Internal consistency was evaluated by calculating the Cronbach’s α. Internal consistency determines to what extent different items within one questionnaire measure the same construct of interest [11]. According to the literature, α>0.70 is regarded as acceptable, while it should not be higher than 0.95, to avoid redundancy [12].
Construct validity
Construct validity reflects whether the questionnaire measures what it was designed to measure. In the case of hand problems, questions measure the typical complaints following Hand injuries [11].
To test the construct of the Arabic MHS, its relationship to a gold standard questionnaire like DASH, this had a validated Arabic version, needed to be examined. For this purpose, Spearman’s correlation coefficient between Arabic MHS and DASH was calculated. A higher correlation coefficient would prove the construct validity of the Arabic MHSQ. Furthermore, the accuracy of the measurement is determined by calculating the floor and ceiling effects. The floor effect is the percentage of patients who scored the lowest possible score (score of 0), and the ceiling effect is the percentage of those with the highest score (score of 48). If more than 15% of the respondents had a floor or ceiling effect, the effects would be considered to be relevant [13].
The calculations were performed using Micorosft Excel 2019, IBM SPSS v.26, and Graphpad Prism v.8.
RESULTS
57 patients participated in this study and completed the MHS and DASH questionnaires and agreed to have their data analysed for research purposes. 31 patients (54.4%) were male, while 26 were females (45.6%). The average age of the participants was 50.65 years, with a standard deviation of 16.05 years, which means that the majority of the sample was between 35 and 67 years of age. As shown in table 1, Mean, standard deviations, minimum, maximum, and floor/ceiling effects were calculated. All subscales of MHSQ seem to have no more than 2% floor/ceiling effect, which indicates that there is no problem with the accuracy of the measurement.
|
Variables |
Mean |
SD |
Min |
Max |
Range |
Floor Effect |
Ceiling Effect |
|
AGE |
50.65 |
16.05 |
18 |
79 |
61 |
- |
- |
|
Hand Function |
51.23 |
23.77 |
0 |
100 |
100 |
2% |
2% |
|
ADL |
58.19 |
21.52 |
59 |
100 |
64 |
2% |
2% |
|
Work |
56.58 |
20.54 |
0 |
100 |
100 |
2% |
2% |
|
Pain |
46.84 |
20.21 |
0 |
100 |
100 |
2% |
2% |
|
Appearance |
59.21 |
22.12 |
0 |
100 |
100 |
2% |
0% |
|
Satisfaction |
56.58 |
56.58 |
57 |
83 |
64 |
2% |
2% |
|
MHS Total |
55.52 |
12.01 |
0 |
80 |
80 |
2% |
0% |
Table 1: Descriptive analysis of demographic age and the score of the Michigan Hand Score Questionnaire, including floor and ceiling effects.
Internal consistency
To estimate the reliability of the questionnaire, Internal consistency was calculated by using overall Cronbach’s alpha which was equal to 0.859, indicating an overall high degree of internal consistency, the Cronbach’s alpha of all the subscales were also proved to be higher than 0.7, which indicate an acceptable to very good reliability (Table 2).
|
Cronbach's Alpha |
|
|
Hand Function |
0.864 |
|
ADL |
0.908 |
|
Work |
0.7 |
|
Pain |
0.71 |
|
Appearance |
0.734 |
|
Satisfaction |
0.758 |
|
MHS Total |
0.859 |
Table 2: Cronbach’s Alpha values for the whole MHSQ and each subscale.
Construct validity
The correlation of different subscales with each other was examined by calculating the Interclass correlation coefficient. The results, which are shown in table 3, indicate that there is a relatively high and significant association between the subscales. The relationship of Pain with Hand function (r=-0.814; p<0.05), Work (r=-0.886; p <0.05) was especially high (reverse association, which means, that higher pain is associated with worse daily life activity and disrupted daily work).
|
Hand Function |
ADL |
Work |
Pain |
Aesthetics |
Satisfaction |
|
|
Hand Function |
1 |
|||||
|
ADL |
0.517 |
1 |
||||
|
Work |
0.641 |
0.619 |
1 |
|||
|
Pain |
-0.814 |
-0.635 |
-0.886 |
1 |
||
|
Aesthetics |
0.315 |
0.32 |
0.329 |
-0.454 |
1 |
|
|
Satisfaction |
0.409 |
0.415 |
0.464 |
-0.528 |
0.773 |
1 |
Table 3: Interclass Correlation Coefficients between subscales of MHSQ.
Bold: Highest coefficient in each column
All coefficients are statistically significant at 0.05 level
For the validity assessment of the Arabic MHOQ, Arabic DASH is used as the standard instrument that is acceptable in almost all countries. Table 4 presents the spearman’s correlation coefficients to measure the level of association between DASH and Arabic MHSQ, and its construct validity, respectively. As shown in Table 2, Arabic DASH shows a statistically significant correlation with all subscales of Arabic MHSQ. However, it indicates especially high correlation with Hand function (r=0.701; p<0.001), activity of daily life (r=0.761; p<0.001) and Pain score (r=-0.620; p<0.001).
|
Hand Function |
ADL |
Work |
Pain |
Appearance |
Satisfaction |
MHSQ TOTAL |
|
|
DASH (TOTAL) |
0.701 |
0.761 |
0.551 |
-0.62 |
0.265 |
0.416 |
0.771 |
|
p Value |
0 |
0 |
0 |
0 |
0.0466 |
0.0013 |
0 |
Table 4: Spearman’s Correlation Coefficients indicating the validity of Arabic MHSQ.
Finally, to visualize the agreement between Arabic DASH and MHSQ, the Bland-Altman plot is used. As shown in figure 1, it seems to be no proportional bias, because as the mean scores of DASH and MHS are rising, their difference remains unbiasedly within 95% confidence interval.
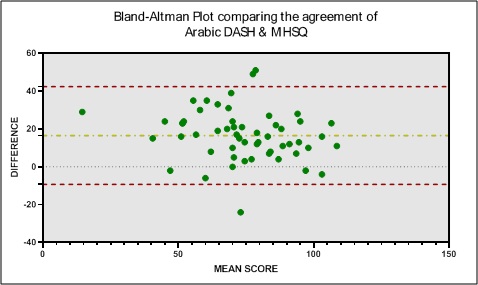 Figure 1: Bland-Altman Plot to visualize the level of agreement between DASH and MHSQ.
Figure 1: Bland-Altman Plot to visualize the level of agreement between DASH and MHSQ.
DISCUSSION
The aim of this study was to translate the MHQ into Arabic and also validate the MHQ-Arabic version. Translation of the MHQ into Arabic was done without any significant changes. Good reliability and validity results were obtained from the MHQ-Arabic version when tested.
We were satisfied with the content validity of the MHQ-Arabic version. We slightly altered the demographic data collected regarding patient characteristics. To fit into the Arabic contest, adjustments were made to the income, ethnic background, job, and medical expense reimbursement plans. We excluded the item on the ethnic background considering that the Arabic population is a relatively homogenous one and most f the population is Arab. Additionally, the MHQ-Arabic version will be used for patients with the ability to read and speak Arabic. Thus, we did not consider the ethnic background as necessary. We changed the choices on income based on the average monthly income in Kuwait. We added items on family income to the MHQ-Arabic version to showcase the demographic characteristics of the Arab extended family. Finally, we added an item to the MHQ-Arabic version to include questions on medical expense reimbursement plans as we considered that it may impact treatment continuity.
The respondents were able to answer the questions during the testing phase of the prefinal MHQ-Arabic version. Thus, the results of this study show that the MHQ was cross-adapted into Arabic with ease, which of course shares similarity to conclusions reached after its translation to other languages [6]. We also examined the construct validity of the MHQ-Arabic version. Overall hand function, ADL, work, pain aesthetics, and satisfaction were major variables considered in predicting the satisfaction of Arabic patients who had injuries of the hand. Patients with low pain score and high aesthetic scores tend to have high satisfaction scores. Also, pain assisted greatly in the prediction of hand function, work, ADL, and overall function. Patients with high pain scores tend to experience difficulty with functioning, work performance, and ADL. Contrastingly, the correlation of aesthetics with hand function was low-to-moderate, although it was a significant outcome for patients with an injury of the hand. The construct validity of the MHQ-Arabic version agreed with the original and other translations of the MHQ [5,14].
An instrument is said to be reliable if the results it produces are consistent on repeated administration [15]. The Arabic version of the MHQ achieved a high internal consistency, which agreed with the original MHQ and other translations [5,14,16,17]. Several translations retained a high Cronbach’s alpha similar to that obtained by our study (> 0.7) after cross-cultural adaptation. Every domain maintained a high degree of internal consistency with the exception of the aesthetics domain. The consistency of the aesthetics differs from the original MHQ [5].The low consistency displayed by the aesthetics domain may be due to poor interrelatedness between the items in the aesthetics domain per hand [18].
The Interclass coefficient of the total score of the MHQ-Arabic version showed high and significant association between the subscales(r=-0.814; p<0.05), Work (r=-0.886; p<0.05). This is similar to the result from the original MHQ as well as other translated versions [5,14,16,17,19,20]. This indicates the high reliability of the domains in the MHQ-Arabic version in repeated testing.
A strength of this study is that it complied was the large number of participants that took part in the prefinal version of translation. Beaton et al. suggested that the prefinal version of translation should be taken by at least 30-40 participants [21]. 57 participants were engaged in our study, their comprehension and interpretation of the questionnaire were investigated with great care. It is important to note that the study was designed to test the reliability and validity of the questionnaire. And even though there is no set guideline to determine the precise number of sample size for development of the questionnaire, large sample sizes are preferable to smaller samples. And so, future studies should employ more participants with varying hand injuries which is necessary to extend knowledge.
CONCLUSION
TheMichigan Hand Outcomes Questionnaire was translated and cross-culturally adapted into Arabic. The Arabic version had a good performance in both validity and reliability testing, which was similar to the original questionnaire and other translated versions. Provided the questionnaire is valid and reliable, it may easily be function as an outcome measurement for self-perception of hand-injured Arabic patients.
DECLARATION
Ethical approval and consent for publication
• Ethical approval was obtained
• Consent of publication was obtained in writing from all participants
• Name of Ethical Committee: Ministry of Health, Kuwait, Research and publication office
• Committee Reference Number: 2019:891
Consent to publish
Consent of participation and publish was obtain with written Format from all participants
Availability of data and material
The data that support the findings of this study are available from [ministry of health Al-Razi Orthopedic Hospital, Kuwait] but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are however available from the authors upon reasonable request and with permission of [ministry of health Al-Razi Orthopedic hospital, Kuwait].
Competing interests
The authors declare that they have no competing interests
Funding
No funding was supplied in this case report
Authors' Contributions
The data collection and the writing were done by all the four authors equally.
ACKNOWLEDGEMENT
The Authors wish to thank the original authors of the Michigan Hand Outcomes Questionnaire for making this project possible.
REFERENCES
- Falkenstein N, Weiss S (2005) Hand Rehabilitation: A Quick Reference Guide and Review. Mosby, Missouri, USA.
- Sabonis-Chafee B, Hussey MN (2012) Introduction to Occupational Therapy. Mosby, Missouri, USA.
- Case-Smith J (2003) Outcomes in hand rehabilitation using occupational therapy services. Am J Occup Ther 57: 499-506.
- Shauver MJ, Chung KC (2013) The Michigan Hand Outcomes Questionnaire after 15 years of field trial. Plastic and Reconstructive Surgery 131: 779-787.
- Chung KC, Pillsbury MS, Walters MR, Hayward RA (1998) Reliability and validity testing of the Michigan Hand Outcomes Questionnaire. The Journal of Hand Surgery 23: 575-587.
- MHQ Michigan Hand Outcome Questionnaire Medical School (2014) The MHQ is a hand-specific outcomes instrument that measures outcomes of patients with conditions of, or injury to, the hand or wrist. University of Michigan Medical School, Michigan, USA.
- Dhippayom JP, Trevittaya P, Cheng ASK (2018) Cross-Cultural Adaptation, Validity, and Reliability of the Patient-Rated Michigan Hand Outcomes Questionnaire for Thai Patients. Occup Ther Int 2018: 8319875.
- Hudak PL, Amadio PC, Bombardier C (1996) Development of an upper extremity outcome measure: the DASH (disabilities of the arm, shoulder and hand) [corrected]. The Upper Extremity Collaborative Group (UECG). Am J Ind Med 29: 602-608.
- Kennedy CA, Beaton DE, Smith P, Van Eerd D, Tang K, et al. (2013) Measurement Properties of the QuickDASH (Disabilities of the Arm, Shoulder and Hand) Outcome Measure and Cross-Cultural Adaptations of the Quick DASH: A Systematic Review. Qual Life Res 22: 2509-2547.
- Guillemin F, Bombardier C, Beaton D (1993) Cross-cultural adaptation of health-related quality of life measures: literature review and proposed guidelines. J Clin Epidemiol 46: 1417-1432.
- Kline P (2000) The Handbook of Psychological Testing. Psychology Press, Mortimer Street, London.
- Fayers PM, Machin D (2013) Quality of life: the assessment, analysis and interpretation of patient-reported outcomes. Manhattan: John Wiley & Sons, New Jersey, USA.
- McHorney CA, Tarlov AR (1995) Individual-patient monitoring in clinical practice: are available health status surveys adequate? Qual Life Res 4: 293-307.
- Koziej M, Trybus M, Myd?owska A, Sa?apa K, Gniadek M, et al. (2017) The Polish version of the Michigan Hand Outcomes Questionnaire: cross-cultural adaptation, reliability, construct validity, and measurement error. J Hand Surg Eur 43: 199-208.
- Schoneveld K, Wittink H, Takken T (2009) Clinimetric evaluation of measurement tools used in hand therapy to assess activity and participation. J Hand Ther 22: 221-236.
- Dias JJ, Rajan RA, Thompson JR (2008) Which questionnaire is best? The reliability, validity and ease of use of the Patient Evaluation Measure, the Disabilities of the Arm, Shoulder and Hand and the Michigan Hand Outcome Measure. The Journal of Hand Surgery 33: 9-17.
- Ebrahimzadeh MH, Birjandinejad A, Kachooei AR (2015) Cross-cultural adaptation, validation, and reliability of the Michigan Hand Outcomes Questionnaire among Persian population. Hand Surgery 20: 25-31.
- Tavakol M, Dennick R (2011) Making sense of Cronbach's alpha. Int J Med Educ 2: 53-55.
- Öksüz Ç, Akel BS, Oskay D, Leblebicio?lu G, Hayran KM (2011) Cross-cultural adaptation, validation, and reliability process of the Michigan Hand Outcomes Questionnaire in a Turkish population. The Journal of Hand Surgery 36: 486-492.
- Oda T, Abe Y, Katsumi Y, Ohi H, Nakamura T, et al, (2016) Reliability and validity of the Japanese version of the Michigan Hand Outcomes Questionnaire: a comparison with the DASH and SF-36 questionnaires. J Hand Surg Asian Pac 21: 72-77.
- Beaton DE, Bombardier C, Guillemin F, Ferraz MB (2000) Guidelines for the process of cross-cultural adaptation of self-report measures. Spine 25: 3186-3191.
Citation: Khaja AF, Al-Roudhan M, Hanna SS, Boshahri MO, Al-Awadh M, et al. (2020) Cross-Cultural Adaptation, Validation, and Reliability of the Michigan Hand Outcomes Questionnaire: Arabic Version. J Surg Curr Trend Innov 4: 037.
Copyright: © 2020 Sager S Hanna, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.