Desmoplastic Fibroblastoma (Collagenous Fibroma): A Case Report
*Corresponding Author(s):
Silvia TaccognaAnatomic Pathology Unit, Regina Apostolorum Hospital, Albano Laziale (RM), Italy
Tel:+39 06 93298423,
Fax:+39 06 9321138
Email:staccogna@reginaapostolorum.it
Abstract
Desmoplastic Fibroblastoma(DF) is a rare fibrotic tumor that has a wide anatomic distribution and it can appearin deep sections of the subcutis, in fascia, in aponeurosis or in skeletal muscles that rarely involving bone. The differential diagnosis of DF includes benign and malignant soft tissue tumors and the misdiagnosis may cause unnecessary surgical overtreatment, especially for those involving bone.
We report the case of a 54-year-old man admitted to the Hand and Microsurgery Unitwith a painless, slow-growing mass in the leftfoot. Magnetic Resonance Imaging (MRI) revealed a well-defined, lobulated soft tissue mass with some areas of hypointense signal on T1-weighted images, predominantly hyperintense signal with some areas of hypointense signal on T2-weighted images. The dimension of tumor is5.5 x 5 cm and a cut section appeared to bewell-circumscribed and homogeneously gray-white and very firm in nature.
The lesion was totally removed by surgical excision and it was pathologically confirmed to DF.
Keywords
Bone; Collagenoma; Desmoplastic; Fibroblastoma; Soft Tissue
BACKGROUND
Desmoplastic Fibroblastoma (DF) is a rare fibrotic tumor that has a wide anatomic distribution and it can appear in deep sections of the subcutis, in fascia, in aponeurosis or in skeletal muscles. DF is a benign tumor that usually occurs in the arms, shoulders, neck, hands, and feet in the fifth to seventh decades of life. It is a paucicellular, hypovascular tumor composed of bland spindle or stellate fibroblastic cells within abundant collagenous or fibromixomatous stroma [1-3].
We report the case of a 54-year-old man with a painless, slow-growing mass in the 1st metatarsal bone of left foot.
CASE PRESENTATION
A 54-year-old man was admitted to the Hand and Microsurgery Unit of Jewish Hospital, with a slowly growing, painless mass adjacent to the 1st metatarsal bone of the left foot. He had a history of fracture of the distal phalanx of the 3rd finger 8 years ago. Physical examination showed an approximately 5cm firm, fixed mass without tenderness. Magnetic Resonance Imaging (MRI) revealed an irregularly-shaped, well-circumscribed, with medium signal intensity on T1?weighted images andlow signal intensity on T2?weighted images (Figure 1A and B).
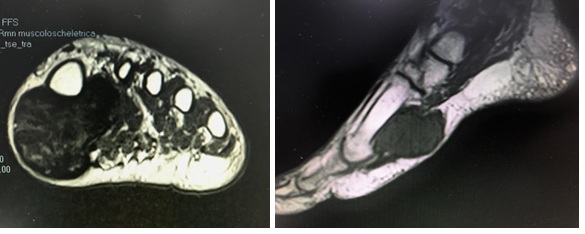 Figure 1A and B: MRI (A) Axial T2-weighted image demonstrates a well circumscribed mass in the left foot which is T2 hypointense and adjacent to the metatarsal bone. (B) Sagittal T1-weighted image confirmed a well circumscribed mass.
Figure 1A and B: MRI (A) Axial T2-weighted image demonstrates a well circumscribed mass in the left foot which is T2 hypointense and adjacent to the metatarsal bone. (B) Sagittal T1-weighted image confirmed a well circumscribed mass.
The tumor was removed by surgical excision. The tumor was attached to the 1st metatarsal bone of the left foot andhad not invaded the bone. Macroscopically, the tumor appeared as a lobulated, firm, whitish mass without gross necrosis, and it measured 5.5 × 5.0 × 2.5 cm (Figure 2). Microscopically, the lesion was hypocellular and composed of homogeneous eosinophilic collagenous matrix background, in which some areas displayed hyalinization (Figure 3A). The cells were scarce and dispersedly distributed in the dense fibrotic tissue(Figure 3B). The cells were spindle? or stellate?shaped, similar to the activated fibroblasts with eosinophilic cytoplasm (Figure 4A) with variable myxoid stroma (Figure 4B). The nuclei were oval without atypia. Immunohistochemical staining demonstrated a strong positive reaction for vimentin (Figure 5). Reaction for alpha-smooth muscle actin, CD34, CD68, EMA, S100, and β-catenin were negative.
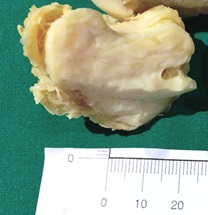 Figure 2: Gross photograph of resected specimen. A multilobulated mass with a smooth surface.
Figure 2: Gross photograph of resected specimen. A multilobulated mass with a smooth surface.
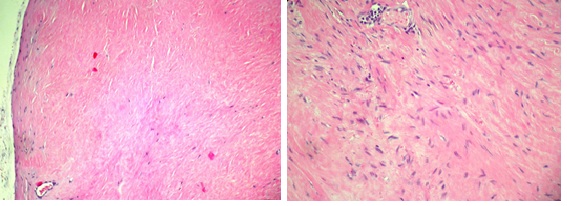 Figure 3A and B: Pathologic findings. Hematoxilin and eosin (H&E)(A) Low-power photomicrograph of the tumor demonstrating fibrous area. The tumor border is well defined(X100). (B) The cells are scarce and dispersedly distributed in the dense fibrotic tissue (X200).
Figure 3A and B: Pathologic findings. Hematoxilin and eosin (H&E)(A) Low-power photomicrograph of the tumor demonstrating fibrous area. The tumor border is well defined(X100). (B) The cells are scarce and dispersedly distributed in the dense fibrotic tissue (X200).
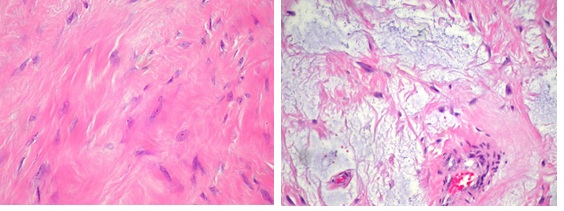 Figure 4A and B: (H&E) High-power photomicrograph (A) The area showing wavy and dense collagen fibers, cellularity is very low. (B) The tumor cells are spindle- and stellate shaped with variable myxoid stroma (x400).
Figure 4A and B: (H&E) High-power photomicrograph (A) The area showing wavy and dense collagen fibers, cellularity is very low. (B) The tumor cells are spindle- and stellate shaped with variable myxoid stroma (x400).
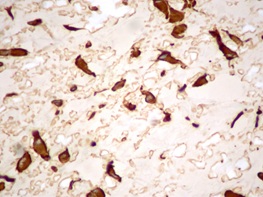 Figure 5: Vimentin immunostain highlights the cytoplasmic processes of the stellate fibroblasts (×400).
Figure 5: Vimentin immunostain highlights the cytoplasmic processes of the stellate fibroblasts (×400).
There has been no local tumor recurrence at the 36 month postoperative follow-up examination.
CONCLUSION
Desmoplastic Fibroblastoma (DF) is a rare neoplasm grossly and microscopically distinctive, benign fibrous tumor that predominantly occurs in men between the fifth and seventh decades and is rare in children and adolescents characterized by the presence of spindle- and stellate-shaped fibroblastic cells that are sparsely distributed in a collagenous stroma [1-3]. This tumor may occur in various locations of the body, including the arm (24%), shoulder girdle (19%), posterior neck or upper back (14%), feet or ankles (14%), leg (14%), hand (8%), and abdominal wall and hip (6%) [1,2]. It is a slow-growing tumor arising in predominantly subcutaneous tissue.
The MRI appearance of a DF is variable but typically shows a well-circumscribed and heterogeneous mass. All cases showed areas oflow to slightly high signal intensity on T2-weighted imagesand areas of low to intermediate signal intensity on T1-weighted images [4,5]. This tumor is composed of stellate-shaped fibroblasts and abundant interstitial collagen. DF can be confused with benign and malignant soft tissue tumors such as a neurofibroma, a nodular fasciitis, asolitary fibrous tumor, a fibroma of tendon sheet, a desmoid tumor (musculoaponeurotic fibromatosis), a low-grade fibromyxoid sarcoma or a nodular fasciitis [6]. Neurofibroma is a benign peripheral nerve sheath tumor with invasive growth. The tumor cells are spindle shaped, loosely dispersed, and surrounded by collagen fibers. It isalways S?100 positive. Solitary Fibrous Tumor (SFT) is a fibroblastic neoplasm that may be found at any location. The tumor is more cellular than DF and it exhibits a variety growth patterns, thick bands of collagen and prominent branching, hyalinized vessels. The tumor cells are characteristically immunoreactive for CD34. Nodular fasciitis is a self?limited lesion, which more often occurs in young adults and grows rapidly. It is composed of plump fibroblasts (or myofibroblasts) with numerous small vessels. Extravasated erythrocytes, lymphocytes and osteoclast-like giant cells are frequently identified. Fibroma of tendon sheath is a slowly growing, dense, fibrous nodule that is firmly attached to the tendon sheath and isfound most frequently in the hands and feet. Most lesions are well circumscribed and have a lobular configuration. It is composed of spindle-shaped cells resembling fibroblasts with elongated nuclei. A characteristic feature is the presence of elongated “cleft-like” spaces of thin-walled vessels particularly at the periphery of the lobules. The lesional cells are more prominently Smooth Muscle Antibody (SMA) positive than DF [6]. Desmoid tumors have more cellularity and vascularity,more infiltrative and less circumscribed at the periphery than DF. At immunohistochemical the cells express vimentin and SMA; butnuclear-positive staining signal of beta-catenin was found in more than 70% of desmoid?type fibromatosis, while no positivity was described in the DF [7].
Low grade fibromyxoid sarcomas have more cellularity and more vascularity and a less homogenous appearance than DF [1]. They also have contrasting fibrous and myxoid zones and a swirled growth pattern. Nodular fasciitis is also more cellular than DF, exhibit a nodular proliferation of fibroblasts, strong mucin deposition, inflammatory infiltration or fascicles of collagen fibers variously oriented [1,3,8].
The exact nature of this lesion is still unclear but some studies stated that it might develop due to a chromosomal rearrangement (11q12) [9] that could also occur in the fibroma of the tendon sheath [10]. Some authors considered this lesion as a neoplasm, which does not have a preceding traumatic or inciting factor [11]. The treatment of choice for this lesion is total surgical excision and the prognosis is excellent with no recurrence [2].
Most patients have been treated by a conservative simple excision, and neither local recurrence nor metastasis has been reported [2,3,11].
A resection of the whole tumor is regarded as an adequate treatment with no reported incidence of local recurrence or metastases.
DF is characterized by distinct histopathologic and clinical features; to distinguish a DF from other tumors correctly is critical for choosing the proper therapy.
CONFLICTS OF INTEREST
The authors declare that there are no conflicts of interest regarding the publication of this paper.
ACKNOWLEDGEMENTS
The authors thank to Alessandro Minciarelli for technical assistance.
REFERENCES
- Miettinen M, Bridge JA Fletsch JF (2013) Desmoplastic fibroblastoma. World Health Organization Classification of Tumours of Soft Tissue and Bone.Lyon, France: IARC Press; 2013 60-61.
- Evans HL (1995) Desmoplastic fibroblastoma. A report of seven cases. Am J Surg Pathol 19:1077-1081.
- Miettinen M, Fetsch JF (1998) Collagenous fibroma (desmoplastic fibroblastoma): A clinicopathologic analysis of 63 cases of a distinctive soft tissue lesion with stellate-shaped fibroblasts. Hum Pathol 29: 676-682.
- Shuto R, Kiyosue H, Hori Y, Miyake H, Kawano K, et al. (2002) CT and MR imaging of desmoplastic fibroblastoma. Eur Radiol 12: 2474-2476.
- Bonardi M, Zaffarana VG, Precerutti M (2014) US and MRI appearance of a collagenous fibroma (desmoplastic fibroblastoma) of the shoulder. J Ultrasound 17: 53-56.
- Gong LH, Liu WF, Ding Y, Geng YH, Sun XQ, et al. (2018) Diagnosis and Differential Diagnosis of Desmoplastic Fibroblastoma by Clinical, Radiological, and Histopathological Analyses. Chin Med J (Engl) 131: 32-36.
- Carlson JW, Fletcher CDM (2007) Immunohistochemistry for b-catenin in the differential diagnosis of spindle cell lesions: analysis of a series and review of the literature Histopathology 51: 509-514.
- Enzinger and Weiss’s SOFT TISSUE TUMORS, ED. 6 2014 Goldblum JR, Folpe AL, Weiss SW. Desmoplastic fibroblastoma p 60-1.
- Nishio J, Akiho S, Iwasaki H, Naito M (2011) Translocation t(2;11) is characteristic of collagenous fibroma (desmoplastic fibroblastoma). Cancer Genet 204: 569-571.
- Sciot R, Samson I, van den Berghe H, Van Damme B, Dal Cin P (1999) Collagenous fibroma (desmoplastic fibroblastoma): Genetic link with fibroma of tendon sheath? Mod Pathol 12: 565-568.
- Nielsen GP, O'Connell JX, Dickersin GR, Rosenberg AE (1996) Collagenous fibroma (desmoplastic fibroblastoma): a report of seven cases. Mod Pathol 9: 781-785.
Citation: Taccogna S, Ienzi S, Molayem I, D’Angelo M, Pagnotta A, et al. (2020) Desmoplastic Fibroblastoma (Collagenous Fibroma): A Case Report. Archiv Surg S Educ 2: 010.
Copyright: © 2020 Silvia Taccogna, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.