Development of a Model for the Care of the Aged in the Cape Coast Metropolitan Area, Ghana
*Corresponding Author(s):
Irene Korkoi AbohDepartment Of Adult Health School Of Nursing And Midwifery, University Of Cape Coast, Cape Coast, Ghana
Tel:+233 261774164,
Email:iaboh@ucc.edu.gh
Abstract
Background: Formal and informal care for the aged shows the dynamisms between home support workers and family care givers.
Aim: To build a culturally accepted model for the care of the aged in the Cape Coast Metropolis (CCM).
Methods: This was mixed methods study conducted with four different target populations in the Cape Coast Metropolis. The research was a multi-staged, multi-sampled method to build a model for the aged.
Results: The idea of assisted living was received well with a lot of enthusiasm, but on condition that care provided is culturally and spiritually sensitive. About 98 percent of caregivers and 78 percent of nurses thought establishment of an assisted living facility would be a great idea.
Conclusion: The model for care would be appreciated in caring for the aged in an era where there are lack resources and employment. Caregivers and nurses could be trained specifically to care for the aged.
Keywords
Aged; Cape Coast Metropolitan area; Care; Model
BACKGROUND
Globally, the population of older adults is growing more rapidly than any other age segment; three decades from now, the number of seniors worldwide is projected to surpass the number of children under the age of 15 [1]. This shift is already taking place in regions where population ageing is “far advanced” [1,2]. Factors contributing to this demographic transition include declining fertility rates, increasing life expectancy, and the ageing of the babies born between 1946 and 1964 who have begun to reach 65years in 2011 and are still living [1,3].
Although both family care and home support are considered essential components of home-based health-care, the experiences of family caregivers who have a relative in receipt of home support services are not well understood because little is known about what constitute home support services [4]. The document add that ageing, combined with a strong desire to age in place, creates an increased likelihood that many elderly people will use homecare. The fundamental principles of ageing in place are that the older persons are able to maintain a sense of normalcy, purpose in life, safety and functional health in their current home environment [5]. However, [5] adds that environmental factors and increase in persons becoming infected with HIV and AIDS at older ages, combined with shortages of nursing and healthcare supplies, make ageing in place more complex in South Africa. Home-care work involves a variety of paid workers with different levels of training and qualifications. They include nurses, social workers, physiotherapists, occupational therapists, and home support workers [4]. Most home-care workers provide direct care or home support: non-professional services in the form of personal assistance with daily activities such as bathing, dressing, grooming, and light household tasks [6]. While some of the responsibility for care of older adults comes from paid health-care services, individuals and families are the cornerstone of home health-care [6].
Practice guidelines and models have been tried in various instances by individuals or organizations in relation to costs, quality, access, patient empowerment, professional autonomy, medical liability, rationing, competition, benefit design, utilization variation, bureaucratic micromanagement of health care and more. The concept has acted as a magnet for the hopes and frustrations of practitioners, patients, payers, researchers, and policy makers [7]. Guidelines for the provision of clinical care are linked to almost every major problem and proposed solution on every policy agenda. The organization of care delivery is determined by a variety of factors such as economic issues, leadership beliefs, and the ability to recruit and retain staff. Evidence of the effect of care models on quality and patient safety is a major factor in decision-making [8]. Historically, there are two categories of models of care: traditional and non-traditional. Traditional care models are represented by four models that have dominated the organization of inpatient nursing care. Functional and team nursing models are task-oriented, while total patient care and primary nursing are patient-oriented but rely on nurses for implementation [9]. In the late 1980s, a number of non-traditional nursing care delivery models emerged that use various mixes of licensed and unlicensed nursing workforces [10]. Care models do not exclusively pertain to the organization of nursing care or inpatient setting [10]. Models have been examined for medical house-staff, pharmacy services and social workers [11]; others have considered ambulatory care, home care and nursing homes [12]. Care models also exist for specific patient populations, such as elderly patients, people with mental health needs, and individuals with chronic conditions, to include disease management and use of technology [13].
Models for delivery of nursing care have been implemented over the past few decades and have performed successfully in workforces that mainly consisted of registered nurses [14]. Several adaptations and combinations of traditional models of patient care delivery have accommodated the changing roles of nurses and various levels of nursing skills mix [15]. These included team-oriented models such as partners in care, shared care nursing, modular nursing and partners in practice [16]. Evaluations of the various models of care delivery have shown that a registered-nurse/prime-skill is associated with better patient health outcomes [17] and lower mortality, improved quality of care, and reduction in medication errors and wound infections [18], which can be explained by registered nurses’ ability to discover early patient deterioration and make timely intervention [19]. Improvements in staff satisfaction, recruitment and retention of staff and reduction in sick leave, improved team spirit and a cleaner ward environment have been attributed to implementation of caring models [20].
AIM
The aim of the study was to build a model of care for the aged that would be culturally accepted in the Cape Coast Metropolis of Ghana.
MATERIALS AND METHODS
Design and setting
The objective of the study was to build a culturally accepted model of care for caring of the aged in the CCM. A mixed method study design was used in which qualitative data was augmented by quantitative data in a sequential approach. An initial exploratory qualitative investigation was followed by a second phase of quantitative investigation with a large sample so that there could be generalization of results to the population [21]. The second, quantitative phase used questionnaires based on the findings from the qualitative phase. The study was carried out in the Cape Coast Metropolitan Area, one of the 17 districts of the Central Region of south Ghana. The metropolis is further divided into 25 sub-districts for administrative purposes. Of the 25 sub-districts, 10 were randomly selected using SPSS version 20 software. These 10 sub-districts were further classified using the existing political administrative instrument for Ghana into three ecological zones: urban (elite residential communities), peri-urban (either urban or rural, but densely populated) and rural (lacking almost all the social amenities). For quick reference the zones were demarcated as zones A, B and C (Figure 1).
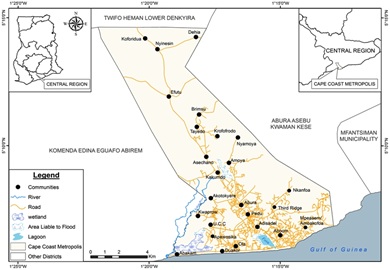
Figure 1: The sub-districts of the cape coast municipality - GIS, UCC, 2014.
In view of the disparities in population density between the various communities, a proportional-to-size approach was used for distribution in recruitment of study participants. The urban and rural areas were allocated 25% each of sample size and the peri-urban was allocated 50% as it was heavily populated with old people.
Sampling and data collection techniques
Four different types of population were recruited for the study: 60 aged persons out of 162 aged were selected by snowball technique, 388 care givers recruited through systematic sampling, 248 nurses who were conveniently selected from four health institutions from the metropolis and 10 stakeholders who were also purposefully selected for the study. The methods employed were individual in-depth interviews, Focus Group Discussions (FGDs) and responses to questionnaires. The inclusion criterion were as follows: aged persons in the age group 65 years, persons taking care of someone in the age group 65 years and older, individuals incharge of caring for an aged, licensed nurses and people in charge of implementation of government policies. The Principal Investigator (PI) and a research assistant collected all the qualitative data. To commence with data collection an Assembly Member (AM) was recruited in each subdistrict or locality to identify a frail and dependent aged for the first interview. After that researchers kept locating one aged after the other with the help of the one they had just finished interviewing. 20 individual indepth interviews and three different focus group discussions were done using the aged. Each discussion was held in the three ecologically identified zones. All caregivers identified for the study were not registered because in Ghana family caregivers are relatives. The assembly members identified caregivers with the help of researchers given inclusion criteria. Systematic random sampling was used – a situation every other household was used for recruiting caregivers. They were so many that researchers had to readjust the age limit to 70 years and above just to create a gate keeper to contain caregivers who wanted to be part of the study. And all questionnaires were answered in full; caregivers who were not able to read and write were assisted to fill the translated questionnaire that was in the local language. 44 caregivers were given the opportunity to take part in the FGDs; one discussion each in the three ecological zones. Four health facilities were used for the study - so nurses used fell into the categories of registered nursing with a regulatory board. Sixty nurses were sampled from each facility through their research unit. 248 questionnaires came back complete and two groups of 20 nurses were arranged for FDGs for 2 health facilities. From computation 36 stakeholders were earmarked for the study but due to their busy schedule 20 were agreed by the researchers. Only ten were able to make time for researchers before data collection went down.
A semi-structured guide was used to conduct the FGDs. Four main questions were responded to by all four groups in both sets of data. The main question centered on participants’ views on the inception of assisted care in Cape Coast and what strategies were to be put in place for the programme. An assembly member for each zone was identified, appointed, and given a few days to choose convenient locations for the scheduled discussion and to organize participants. After each FGD, questionnaires were distributed around the community for responses. Data collection began in October 2016 and ended in January 2017. Discussion lasted between 40 minutes to one hour. Quantitative data was extracted from the questionnaires that were answered in full. Participants and respondents were assured of confidentiality and anonymity before each procedure started. They were given consent forms to read and sign. Those who could not read and write were given detailed explanation on what they were about to do before consenting by thump printing. Minors were asked to present their guardian who either agreed or declined their participation (Table 1).
|
Target Group |
Target population |
Sample Size Estimated |
Actual Sample Proposed |
Sample Used |
Sampling Technique |
Instrument Used/ Method of Data Collection |
|
Aged |
10,873 |
375 |
162 |
64 |
Snowball |
Question guide/individual in-depth interview |
|
Caregivers |
87,784 |
384 |
382 |
388 |
Systematic |
Question Guide/questionnaire |
|
Nurses |
691 |
248 |
248 |
240 |
Convenient |
Question Guide/questionnaire |
|
Stakeholders |
40 |
36 |
20 |
10 |
Purposive |
Question guide/individual in-depth interview |
Table 1: Data collection sampling and techniques.
Data management and analysis
The tape recorded FGDs were transcribed verbatim from the native language into English by the PI and the trained research assistant. The transcripts were checked for accuracy and quality and cleaned for anonymity by the PI and the research assistant. When no discrepancies were identified, the files were coded for analysis by the two research fellows. The method of analysis was interpretive descriptive content analysis to gain insight into participants’ perceptions and strategies in relation to the inception of assisted living in the Cape Coast Metropolis. The initial stage involved reading the contents of the data files to identify major thematic areas. The main task was to display data in a way that meaningfully indicated conceptual distinctions and provided contents that illuminated the concept being investigated. Two meaningful themes emerged from the data: (a) perception of the inception of assisted living in Ghana and (b) strategies to be put in place. These themes emerged with supporting statistical information as backing for the development of the model for the caring of the aged.
RESULTS
Participant characteristics
Study participants learning about the purpose of the study were willing to give researchers information. Among the four different categories of participants recruited for the study, the majority spoke English. Marital status categories of participants were married, never married, widowed and separated/divorced. Ages ranged from 18 years to 98 years; most were Christians, distributed among the following recognized sects of the Christian religion: Roman Catholic faith, Methodist, Anglican, Disciples of the Twelve Apostles and Awayo. They included former fishmongers, petty traders or artisans but subsequently unemployed when they assumed their new role as caregivers. Numbers of children for those who were parents ranged from two to ten.
Inception of assisted living in Ghana
The Strength Weakness Opportunities Threats (SWOT) analysis approach was used to explain the concept of assisted living to participants. The reaction to the concept was different among the four groups. The aged regarded the concept favourably and were curious to know what the programme entailed. They all wanted to have a feel of it, but since they were no longer earning money and decisions had to be made by significant others or their children, they were quick to add that they needed permission before a decision could be made where they would be part of the programme when established. Their caregivers were in a dilemma because although they were interested they were also worried about community reactions since this was not a culturally accepted practice. Nurses were adamant that the change was about to take place in their work domain. They felt day care would be ideal, as this way families would continue to be involved in taking care of their own aged rather than passing the responsibility on to other people. Nurses stressed the importance of reciprocation of care since everyone would ultimately be in need of old age care from younger generations who had once been cared for by them in childhood. Government and political office holders who were interviewed as stakeholders were not in favour of government involvement in the disbursement of funds because they felt that the government already had too many other financial priorities. There were also suggestions that, except in the case of aged who had no one to look after them, the only care intervention that might be provided for the elderly was provision of nutritious hot meals.
Responses from aged participants
The following comments are illustrative of responses for elderly participants who were involved in the study as focus group participants:
- • The day-care sounds very interesting … I am interested in that one because I feel very lonely and bored most of the time … it is a laudable idea. … Government should do something about this programme. Female, Site 4
- • Oh (laugh) that will be interesting … and there will be caregivers and people my age with nurses 24/7? It will be a good idea … are you sure? Is money involved? I think my children will pick up the cost … If there will be a way to visit the shed I will love to be part of it. Male, Site 3
- • For me, I am hearing of this for the first time … I have to talk it over with my children … sell the idea to them. FA 1
- • Yes, it is laudable programme … but I will prefer the day-care aspect … because it is so lonely when my grandchildren leave for school. FA 6
- • I have to discuss it with my children so that we collectively decide what to do. … We have to listen to our significant others before making a decision … so I will suggest we met again on this issue. … If I say something now without the decision from my children … it would be a lie. FA 5
Responses from caregivers
A number of caregiver participants expressed cultural misgivings, but there were also expressions of positive interest:
- • In Ghana we don’t do these things … to be frank people will insult you … and cast insinuations that you were not look after your parents who matter most in your life. FC 5
- • I like it … just as we take our children to the day-care and leave them with an attendant; we anticipate attendant recklessness … now we need to do this for our parents. It is because we are all working … we need to accept this programme and find a place for them. FC7
Almost all caretaker respondents (98.2 percent) in the quantitative investigation were in favour of the establishment of an assisted living facility, although 40.5 percent said they would not be happy to send their wards to an institution for continuous care.
Responses from nurses
Some nurses expressed initial disapproval at the beginning of focus group discussions:
- • Looking at our culture, you see it cannot be possible because looking at our economy as a country … bringing this programme will change our people. FN1
- • The society too comes to play when we are discussing this issue … because it is said that ‘if someone looks after you and you erupted your teeth - you must also look after that person until his teeth falls out’. So it means that it is our responsibility to care for our parents since they took care of us … this is what the society taught us … so when somebody leaves the mother in the care of people who are not family members … the society will frown at that daughter or child. … I think we have to consider our belief systems and our customs. FN7
After further discussion, more positive comments were made:
- • I think we are arguing because there is no clear cut policy on how the aged are to be cared for and it will need an intense health education to change some things … we are to highlight the benefits of this caring system to our clients and other members of their family. … Again I think we also need dialogue with the government to put up structures. FN8
- • I think if government can implement that by establishing aged homes … like in the developed countries … why not, so that our aged can have a place. They are poor and they need government to support them. And they must be allowed between the home and the institution and the aged wishes. FN3
- • I saw this nursing in a foreign movie once … and it was very fine … Due to our cultural beliefs the old ones believe there is a spirit of the environment so they would not like to leave their environment. … But if government too can do that for us it will be fine. … Nurses can take nursing to the doorstep of the aged. … Caring for their spiritual needs is also very important so if they can retrain the nurses. … Every month or twice a month, a nurse can go and visit them at home and involve family members in their care. FN6
- • Government should train more Community Health Officers (CHOs) to handle the aged just like they are handling the children. Meanwhile, the young ones cannot say they will not work to look after their aged parents … so the government should train nurses solely for this programme to go round the homes to help with caring for the aged. FN5
In the questionnaire responses, when nurses were asked if they would accept responsibility for providing care for the aged in the institution, almost all (98%) were in favour of government establishing a home for the aged, 65% were ready to accept redeployment to the facility as staff members, and 33% did not want to be in such environment.
Responses from stakeholders
Characteristic comments from office-bearer stakeholders were:
- • It will be for the rich people … but only few can patronize such a programme … usually these rich aged like hiring people to take care of them or their parents. IS1
- • The programme is a laudable idea but it should add the style of the school feeding programme where we will serve hot food … some of the death among the aged is not due to old age but to hunger, loneliness, sadness, bitterness… they feel left out. So the school feeding strategies should be adopted. IS3
- • The aged should be at home so that the caregivers will visit and take care of them. For the nurses their visit could be daily or number time in the week or month for a certain fee. … The programme should also be a multifaceted kind of thing. IS5
Strategy for the programme
The aged expressed desire for the programme to be established. They confirmed that they did not have money to pay for their upkeep should the need arise, but that their children and relatives would take care of their bills. Some confirmed that they would only support the notion of assisted living if the programme was privately controlled, since a government initiative was likely to collapse. Caregivers also thought the cost of upkeep should be the responsibility of the family, in particular the children. Nurses gave a lot of input; they thought the programme would succeed if it was run by a private entrepreneur, and it should be funded by the aged, the family and government. They suggested that there should be flexibility in regard to residence in the institution, so that the aged could, if they wished, choose to alternate between staying at home and living in the facility. The institution needed also to make provision for religious observance by residents in relation to the needs of their religious sects. The stakeholders felt that the environment provided by the facility needed to be responsive to the needs of the elderly, and that there should also be awareness raising and education on the programme and on the policy for the aged. Costs must be solely the responsibility of immediate family and relatives. Government input in the programme should be formulation of policy to protect users of the programme and provision of an insurance scheme to support the programme. A system for feeding the aged at home should be incorporated in the programme. There should be training of the workforce and amendment of the curriculum.
- • The programme is a laudable idea … Government should do something about … the day-care sounds very interesting and I am interested in that one because I very lonely bored and bored most of the time. Male, Site 4
- • This is interesting … and there will be carers and people my age with nurses 24 /7? It is a good idea. I do not believe in programmes controlled by government. If there will be a way to visit the shed I would love to be part of it. Male, Site 3
- • My daughter will be the one to take care of payment if I should attend. … I think it is the duty of the relatives to pay for their wards’ upkeep. Female, Site 9
Two caregiver responses on strategy were
- • The government must support aged until they die … it is a very laudable programme … funding must be from the individual but government must subsidized cost … the children would support. FB2
- • me too … I think government should come in … just like social security. FB4
Indicative nurse comments on strategy were:
- • To care for the aged we need a database … we can monitor them and the number of people who will be joining every year so that government would plan for them. … The family too should be prompted of their supporting roles so that they can pay something. FN14
- • There must be training of nurses to go from house to house on monthly basis to check on the aged at home. … I think government could partner with a private entrepreneur to make it more privately owned and run. The consent of the aged must be sorted before he/she is taken there so that they can choose their option. FN5
- • If we say that government should take up responsibility, it should be in the form of setting up policies to care for the aged … just like it did for the three tier system in the social security scheme then make provisions for after years in active service when one goes home. … Such funds could easily be accessed for the owner. … More emphasis should be laid on social support. FN8
- • For the day-care, our communities are structured such that every community in Ghana has a community or social centre … so the chiefs should allow their people to be trained … so that they care of the aged at the community centre. … The day care will work … it will be a place where they will have a lot of fun then they come home in the evening … this will work in Ghana. FN3
Indicative stakeholder comments were:
- • There should be a lot of advocacy, lobbying, awareness creation and education so that the people of CCM would accept the programme. IS4 & IS1
- • Educate the people on the aged policy of Ghana. IS2
- • The family must take up payment of the bills … you will need to start like an agency where those who need services can apply either to work or stay in then you give them the cost. … So that the family would take the cost, yea. IS1
- • There should be a place - an environment with proper facilities such as bathroom, living place, etc. and then be able to employ people to work e.g. the semi-skilled. IS4
- • The programme should be able to serve hot meals to the aged at home … it should add the style of the school feeding programme where we will serve hot food. IS3
DISCUSSION
The findings from this study indicated elements for incorporation in an interventional model that will help in care given to the aged both at home and in an assisted living environment. The discussion was based on a technology acceptance model - TAM and the SWOT analysis. Figure 2 presents the model in flow-chart form.
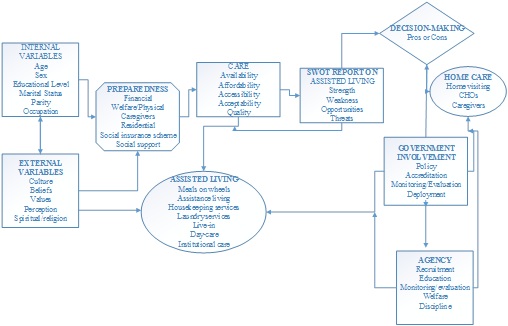
Figure 2: Model for assisted living care for cape coast metropolitan area.
Overview of the model
The findings from this study enabled definition of categories and indicated major themes informing concepts of caring for the aged in the proposed caring system in CCM. Ten interlinked concepts emerged that reflected how the people of CCM would want this concept to flow, and the programme can only be achieved if stringent attention is given to these factors: the factors are internal and external factors, preparedness, care and SWOT report on assisted living. Application of this model to the existing caring practices will facilitate a well-defined and planned approach of caring for the aged in the CCM.
Components of the model
The context
Caring for the aged is the responsibility of the family [22] and it takes place in a complex community within the environment where they live [23]. This model was a product of interactions between four target groups: the aged, their caregivers, nurses of all categories, and government office holders or stakeholders. There is recognition that caring for the aged is increasingly being abandoned by communities and gradually becoming the sole responsibility of individual nuclear families in the present phase of scarce resources [24]. The model provides a clear understanding of how factors are interrelated in implementing care for the aged, irrespective of where they are or the cultural context.
The target
The target for this model is elderly persons aged 65 years and older, who are frail and depend on significant others for survival. It also links with the individuals to prepare adequately for their retirement and ageing.
Objectives of the model
The overall aim of the model is to improve caring practices for the aged in Ghana. The objectives of the model are as follows:
- • Assist individuals and families to prepare adequately for retirement and ageing
- • Create awareness and educate communities on assisted living facilities
- • Train aids and retrain nurses on their roles in assisted living
- • Advocate for government to formulate policies to help establish assisted living in Ghana
Provisions of the model
Assisted living is designed to accommodate the needs of frail individuals or seniors through design features, housing management, and access to healthcare services [25]. It is the most rapidly growing field in the care market since the mid-1990s; its opportunity is demonstrated by expanding numbers of residents and settings [26,27]. Assisted living facilities currently serve the largest percentage of seniors who are frail and require assistance with their activities of daily living but do not require the 24-hour medical care provided in a long-term care setting [27]. The model provides an integrated approach to planning for ageing in a peaceful and harmonious environment. It is an unassuming but exceptional model that provides an opportunity for policy makers and other stakeholders to adapt a caring practice to help the aged in their own chosen environments. The model proposes a guide to how family, significant others and the general public can come together to care for the aged.
Structure of the model
The model fits into Theoretical Acceptance Model (TAM) a theoretical model that helps to explain and predict a user’s behaviour with information technology [28]. TAM provides a basis with which one traces how external variables influence belief, attitude and intention to use [29]. The model is intended to apply to all aged in the communities in the delivery of care at all levels in the socio-economic category but with emphasis on a multidimensional side-to-bottom approach that will preserve the principle of informed decision making in the use of assisted living. The different factors that interacted at multiple stages were categorized and it was confirmed that TAM could be modified and applied to the study of acceptability and motivation to make uses of a new technology. In implementing the model, the participants will include the aged, caregivers, healthcare workers and political or government office-bearers. The model defines internal and external variables which are characteristics of an individual’s preparedness for retirement and ageing in relation to the care that he would want to receive whether at home or in assisted living. SWOT analysis comes in to explain both sides of the care, but especially the assisted care. The aged can then decide either to stay at home under the supervision of a caregiver and the community health officer or to stay in assisted living care. If he chooses the latter, he makes application through an agency controlled by government policy and is admitted to the facility. Government has a direct link with the assisted living facility through monitoring and evaluation teams and with the home through the community health officers. The assisted living facility will run in a culturally accepted manner. The model is structured to include linkages involved in an individual’s preparedness for making an informed choice of assisted living in an environment that would be politically and culturally accepted by stakeholders.
Propositions of the model
As people get older, they may find it harder to take care of themselves however, not everyone has a family to go to when this time comes, so it is up to an assisted living facility to help them [30]. The strength of the model lies in its appropriateness within the context of traditional caring at home and the perception of the consumers of the product. A multifaceted side-to-bottom approach will enhance achievement of the objectives set for model.
Expected outcomes of the model
The expected outcome will be enhanced opportunity for the aged to enjoy good care at home or in assisted living.
Purposes and uses of the model
Assisted living facilities provide only the services the resident needs, such as food purchased and prepared, with some preferring to do these things on their own. Many facilities offer services for health care, including on-site nurses or complete ambulatory centres [30]. The complexity of implementing assisted living in an under resourced environment requires re-modelling of strategies within workable contexts [19]. Hence, the purpose of the model is to enhance aged caring practices in assisted living facilities in Ghanaian communities.
Essentials of the model
Assisted living options for older adults include support services such as dining, wellness, social activities, personal care, medication management and more, in setting that may provide either independent or shared living accommodations [31]. To discuss and decide on these options, the team members and client need to have clear understanding of the type of care desired and how it will be funded. The programme is designed for implementation to begin when the individual retires or becomes frail and needs additional care. It provides specific activities for planning according to varying individual demands and circumstances. When all the steps in the model have been considered individually and accounted for, family members will be able to send their aged to the facility for care. The assisted care facility will need to have clear strategies, guidelines or policies covering preparedness and preferences in relation to the care to be rendered.
Concepts of the model
Where people were once at the mercy of the healthcare system they now have the opportunity to be more engaged in their own care and to reap better in the process. According to [32], the patient is becoming the customer, and smart providers are delivering better experiences to customers on their own terms. The first set of elements in the model is internal and external variables. Internal variables include biological, psychological and cognitive dimensions. They are often described as non-modifiable variables because, for the most part, they cannot be changed. Internal variables, according to [33], include age, sex, race and genetic makeup. In the model, internal variables include parenthood, marital status, educational level and occupation, which influence the individual in the sociological context. However, when internal variables are linked to health and wellness, it is necessary to work diligently with the client to influence external variables or culture. Culture is a belief system which involves norms and values that may assist in health promotion and prevention of illness. Culture and social interactions influence how a person is cared for at home. Each culture has ideas about life and these are often transmitted from parents to children. Usually this transmission is through tradition and a sense of attribute which shows the degree to which an individual’s culture has been translated into norms, values and beliefs and has been cultivated to a particular level of sophistication.
Care: Care is a product for sale, and it is made up of Activities of Daily Living (ADL) and Instrumental Activities of Daily Living (IADL). This product will be readily available because it will be delivered by attendant who will be skilled or semi-skilled, and it is made acceptable, affordable, accessible and of quality. The quality of the care to be provided will be the proper performance (according to standards) of interventions that are known to be safe, that are affordable to the society in question, and that have the ability to produce an impact on mortality, disability and malnutrition [34].
SWOT report: Strengths would be findings or observations that would favour or are likely to support and encourage caretakers and nurses to adopt new skills and ideas to serve their aged. Weakness are findings or factors which might not favour or are likely to hinder, and discourage caretakers, nurses and family from encouraging the adoption of an assisted living facility for the aged. Opportunities are conditions or factors that might arise from external influences, such as societal views, norms and values external to the creation of an assisted living facility that can help assist to promote the achievement of the set objectives. Threats are external conditions that can hinder achievement of aged assisted living objectives. Examples could be inadequate financial status or non-existence of insurance to assisted living.
Decision making: Healthy individuals need to make economic, social and religious decisions about how they want to live their lives in their retirement. This will reduce dependence on significant others and uncertainty in decision making. People must actually have a say in issues involving their finances. Family members or benefactors must weigh the pros and cons of assisted living to make a decision.
Government involvement: one major reason that governments exist is that they create rules, but whether the rules are necessary or desirable is opened to question, because different types of governments have certainly created a wide variety of rules [35]. Government originated with the need to protect people from conflicts and to provide law and order. Our study findings indicate that participants wanted government to formulate a policy to govern the programme. Government also has an obligation to protect stakeholders such as caregivers and receivers in the programme through mechanisms such as licensing and accreditation for commencement, monitoring and evaluation of the programme, and to manage and control the programme and deploy government workers to run the facility. Government also has a role to play in the community in protecting those who would not be direct beneficiaries of assisted living facilities.
Home care: in the model, home care (age in place) will be provided for elderly persons by domestic workers if their own children are unable to co-reside with them to provide care due to occupational and other demands. This presuppose that the aged will be in situation where pertinent decisions concerning their care will be made for them. Thus, the aged will be staying at home and receiving care directly or indirectly from assisted living through the government or the agency.
Agency: A senior in-home care agency would be responsible for hiring and paying caregivers, and for training, screening, and supervision of the individual caregivers. An in-home care registry, on the other hand is a referral service that matches clients with caregiver who are independent contractors. Independent in-home caregivers will be hired through the agency. The agency will also be responsible for setting up a tax withholding system for independent caregivers. The agency will be responsible for overseeing the welfare of caregivers as well as instilling discipline in all stakeholders.
Assisted living facility: Choosing an assisted living care can be perplexing, and families need help to make more deliberate and thoughtful decisions. There are various options for assisted living facility services, each with their own implications that need to be taken into account in making proper informed choices during what can be a very uncertain and stressful time. Assisted living decisions usually involve several people (the older person and family members for a start). Different options included in this model are meals on wheels, assisted living, housekeeping services, laundry services, live-in care, day and institutional care.
Boundaries of the model
The model as presented will fall within the existing traditional home care structure, with the central focus being the aged who require assistance from the general public.
Unique contributions of this research
The current model will be a pioneer model to be developed for care of the aged in the CCM and will create opportunities for collaboration within and among stakeholders involved in the Primary Health Care programmes. At each step of the model, the aged and the caregivers will be active participants in their own preferred environments and the agency will also help to deploy personnel and regulate the caring practices.
CONCLUSION
When all stakeholders (care consumers and givers) adhere to this model of care, delivery of care will be extended to cover all the aged in CCM.
IMPLICATION FOR NURSING
The model will create a platform for comprehensive and holistic caring for all aged in the CCM. It was designed with the concept of primary health care in mind. Government have been quiet on issues of aged care - with this model all aged will be included in data where they will be monitored and cared for by community health officer's an auxiliary health team of the Ministry of Health/ Ghana Health Service. The aged will be cared for irrespective of their social status, colour or creed or needs.
ETHICAL APPROVAL
The study was approved by the Humanities and Social Sciences Research Ethics Committee of the University of KwaZulu-Natal (HSS/0608/016D) and the Dodowa Research Centre (IRB Ghana Health Service) of Ghana (DHRCIRB/06/06/16). Voluntary participation was accorded with written and signed consent.
COMPETING INTERESTS
The authors declare that they have no competing interests
AUTHORS’ CONTRIBUTIONS
IKA conceived the study, was the principal investigator and made most extensive contribution to the research, as well as drafting the manuscript. BPN was involved in the conception of the research, guided the development of the protocol to its completion and contributed to the draft of the manuscript. IKA and BPN revised the manuscript for its intellectual and professional content.
ACKNOWLEDGEMENT
We thank sub-districts that granted permission to conduct this research, and the field work was self sponsored as a student from the University of KwaZulu-Natal, Durban, South Africa.
REFERENCES
- United Nations (UN) (2017) World population ageing. United Nations, New York, USA.
- Public Health Agency of Canada (PHAC) (2006) Healthy aging in Canada: A new vision, a vital investment from evidence to action, A Background Paper Prepared for the Federal, Provincial and Territorial Committee of Officials (Seniors). Public Health Agency of Canada, Ottawa, Canada.
- Statistics Canada (2007) A portrait of seniors in Canada, 2006. Statistics Canada, Ottawa, Canada.
- Sims-Gould J, Martin-Matthews A (2010) We Share the Care: Family Caregivers' Experiences of Their Older Relative Receiving Home Support Services. Health Soc Care Community 18: 415-423.
- Booker SQ (2015) Lessons Learned About Ageing and Gerontological Nursing in South Africa. Curationis 38: 1216.
- Canadian Home Care Association (2008) Home care Association Annual report ‘Portraits of Home Care in Canada’. Canadian Home Care Association, Ottawa, Canada.
- Jgreen (2014) Nursing careers and jobs, nurse.com powered by Relias.
- Titler MG (2008) The Evidence for Evidence-Based Practice Implementation. In: Hughes RG (ed.). Patient Safety and Quality: An Evidence-Based Handbook for Nurses. Agency for Healthcare Research and Quality (US), Rockville, USA.
- Tiedeman ME, Lookinland S (2004) Traditional Models of Care Delivery: What Have We Learned? J Nurs Adm 34: 291-297.
- Jennings BM, Clancy CM, Lavizzo-Mourey R (2008) Foreword. In: Hughes RG (ed.). Patient Safety and Quality: An Evidence-Based Handbook for Nurses. Agency for Healthcare Research and Quality (US), Rockville, USA.
- Gathercole MF, DeMello LR (2001) Development of the Workload Analysis Scale (WAS) for the Assessment and Rehabilitation Services of Ballarat Health Services. Soc Work Health Care 34: 143-160.
- Finnema E, deLange J, Dröes RM, van Tilburg W (2001) The Quality of Nursing Home Care: Do the Opinions of Family Members Change After Implementation of Emotion-Oriented Care? J Adv Nurs 35: 728-740.
- Jerant AF, Azari R, Martinez C, Nesbitt TS (2003) A Randomized Trial of Telenursing to Reduce Hospitalization for Heart Failure: Patient-Centered Outcomes and Nursing Indicators. Home Health Care Serv Q 22: 1-20.
- Fernandez R, Johnson M, Tran DT, Miranda C (2012) Models of Care in Nursing: A Systematic Review. Int J Evid Based Healthc 10: 324-337.
- E-Morris M, Caldwell B, Mencher KJ, Grogan K, Judge-Gorny M, et al. (2011) Nurse-directed Care Model in a Psychiatric Hospital: A Model for Clinical Accountability. Clin Nurse Spec 24: 154-160.
- Tran DT, Johnson M, Fernandez R, Jones S (2010) A shared care model vs. a patient allocation model of nursing care delivery: Comparing nursing staff satisfaction and stress outcomes. Int J Nurs Pract 16: 148-158.
- Needleman J, Buerhaus P (2003) Nurse Staffing and Patient Safety: Current Knowledge and Implications for Action. Int J Qual Health Care 15: 275-277.
- Needleman J, Buerhaus P, Pankratz VS, Leibson CL, Stevens SR (2011) Nurse Staffing and Inpatient Hospital Mortality. N Engl J Med 364: 1037-1045.
- Clarke SP, Donaldson NE (2008) Nurse Staf?ng and patient care quality and safety. In: Hughes RG (ed.). Patient Safety and Quality: An Evidence-Based Handbook for Nurses. Agency for Healthcare Research and Quality (US), Rockville, USA.
- NSW Department of Health (2006) First Report on the Models of Care Project. NSW Department of Health, Sydney, USA.
- Creswell JW (2003) Research design: Qualitative, quantitative, and mixed methods approaches. SAGE Publications, California, USA. Pg no: 246.
- Lindsey E, Hirschfeld M, Tlou S (2003) Home-based Care in Botswana: Experiences of Older Women and Young Girls. Health Care Women Int 24: 486-501.
- Aboderin I, Hoffman J (2015) Families, Intergenerational Bonds, and Aging in Sub-Saharan Africa. Can J Aging 34: 282-289.
- Ghana Statistical Service (2012) 2010 Population and Housing Census. Summary Report of Final Results. Ghana Statistical Service, Accra, Ghana.
- Health Canada (2005) ARCHIVED - 2005 GOL Public Report - Strengthening On-Line Results at Health Canada [Health Canada, 2005]. Health Canada, Canada.
- McGrail KM, Lilly M, McGregor MJ, Broemeling AN, Salomons K, et al. (2012) Who uses assisted living in British Columbia?: An initial exploration. UBC Centre for Health Services and Policy Research. Vancouver, Canada.
- Al-Omari E (2014) Seniors' experiences in assisted living facilities: a study exploring quality of life. University of Lethbridge Research Repository, Canada.
- Legris P, Ingham J, Collerette P (2003) Why do people use information technology? A critical review of the technology acceptance model. Information & Management 40: 191-204.
- Park SY (2009) An Analysis of the Technology Acceptance Model in Understanding University Students' Behavioural Intention to Use e-Learning. Educational Technology & Society 12: 150-162.
- O'Brien R (2017) Difference between Assisted Living and Supportive, Living. Our everyday life.
- MetLife Mature Market Institute (2012) The Essentials Assisted Living Communities, MetLife Mature Market Institute, New York, USA.
- Johnson S (2016) Start-ups powering the shift to proactive care. The Senior List.
- Berman AT, Snyder S, Frandsen G (2016) Kozier & Erb's Fundamentals of Nursing: Concepts, Process, and Practice (10thedn). Macmillan Heinemann, USA.
- World Health Organisation (2013) Guidelines: Updates on the management of severe malnutrition in Infants and children. World Health Organisation, Geneva, Switzerland.
- Slaughter AM (2017) 3 responsibilities every government has towards its citizens. World Economic Forum, Cologny, Switzerland.
Citation: Aboh IK, Ncama BP (2020) Development of a Model for the Care of the Aged in the Cape Coast Metropolitan Area, Ghana. J Gerontol Geriatr Med 6: 055.
Copyright: © 2020 Irene Korkoi Aboh, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.