Diabetes Mellitus among Old People and Associated Comorbidities
*Corresponding Author(s):
Salem AlsuwaidanResearch And Innovation Center, King Saud Medical City, Ministry Of Health, Riyadh, Saudi Arabia
Tel:+966 545566722,
Email:sa.alsuwaidan@ksmc.med.sa
Abstract
The purpose of this study is to find suggestions on how to deliver adequate standard of care and reductions of hospitalizations in older people with diabetes, and to find out the prevalence of most associated diseases in elderly patients with diabetes.
Methods: This retrospective cross-sectional study included patients aged ≥65 years with diabetes mellitus. Data were collected retrospectively from 2853 older patients diagnosed with diabetes mellitus, including sociodemographic characteristics and other comorbidities.
Results: A total of 2853 elderly patients aged 74.1 years (±7.3 SD) were included, with an average of 2.68 (±0.9 SD) diseases associated with diabetes mellitus. In older patients, the disease most associated with diabetes mellitus was hypertension (2324 patients), followed by other heart diseases (927 patients). Most older patients had three comorbidities (1197 patients). Elderly with Diabetes Mellitus (DM) decreased with older age by 180 patients (15.85% of the patients) every 5 years. There were 1634 older male patients with DM compared with 1219 older female patients. Saudi patients were the most prevalent (2061 patients).
Conclusion: There was a 15.85% decrease every 5 years in the number of older patients with DM, with this proportion decreasing in line with increasing age. Diabetes self-care monitoring is complex, and it is important to follow recommendations for dietary requirements to achieve adequate standards for reducing hospitalization and appropriately managing diabetes.
Keywords
Comorbidity; Diabetes mellitus; Elderly; Prevalence
Introduction
Diabetes Mellitus (DM) is a major public health problem worldwide and it is more relevant in elderly population. Diabetes in the elderly is associated with various risk factors and complications. It is estimated that third of the United States population for those aged of 65 years and above were diabetic and this ration is increasing in parallel of the age increasing [1]. Exhausting of beta-cell function in elderly, in addition to weight gain resulted in insulin resistance [2], which could lead to worsen lifestyle, nutrition, ended with accumulation of glucose in the blood.
The prevalence of DM was 30% in those patients with average of age of about 55 years old [3]. According to the American Diabetes Association (ADA), diabetes may be diagnosed based on one of the following criteria: Fasting Plasma Glucose (FPG) level of 126 mg/dL (7.0 mmol/L) or higher, or a 2-hour postprandial plasma glucose level of 200 mg/dL (11.1 mmol/L) or higher after a 75-g Oral Glucose Tolerance Test (OGTT), or a random plasma glucose of 200 mg/dL (11.1 mmol/L) or higher in a patient with classic symptoms of hyperglycemia or hyperglycemic crisis, or a hemoglobin A1c (HbA1c) level of 6.5% (48 mmol/L) or higher [4].
Diabetes is a major cause of morbidity and mortality worldwide, and it is associated with poor general health and lower quality of life. It also carries a risk of macrovascular complications, with elderly patients being disproportionately affected [5]. Diabetes mellitus, its complication, and associated diseases were becoming big alarm as worldwide health problem [6]. Diabetes mellitus considered as the second most extensive prevalence condition among older patients [7]. It has been reported by the World Health Organization (WHO) that Saudi Arabia ranks as the second highest country in the Middle East and the seventh highest country worldwide in the rate of diabetes. The population of diabetic patients was estimated to be 7 million and almost 3 million are pre-diabetes [8]. The proportion of the diabetic patients in older population is projected to exceed 30% in the USA [9]. It has been reported that an increased mortality in elderly diabetics compared with normally glucose-tolerant subjects [10].
Currently, there is no universally accepted age threshold to define the term of old people, however, most developed countries have accepted and reported that the chronological age of 65 years old as a definition of elderly individuals, mainly as a construct equivalent to the traditional age of retirement. In addition, the definition of older patients may be better be delineated not by age, but by an individual’s active contribution to society or other socially constructed indicators [11]. Moreover, most of previous literature considered the age of 65 years and above as a cut-off definition [12]. Globally, the population is ageing and the World Health Organization (WHO) predicts that, by 2050, the world’s population aged 60 years and older is expected to be 2 billion, up from 900 million in 2015 [13].
The worse scenario diabetes in elderly patients is a patient with poor glycemic control associated with brittle diabetes, insulin resistance, recurrent diabetic ketoacidosis and also with insulin experience [14-16] in addition to poor compliance and education [17]. As the duration of diabetes increased in elderly patients, there will be more susceptibility to increased risk of diabetes- related complications, and at further risk for developing geriatric syndromes [18]. The purpose of this study is to find suggestions on how to deliver adequate standard of care and reductions of hospitalizations in older people with diabetes, and if there is any possibility to reduce mortality resultant from DM in elderly.
Aim: To estimate the number of associated comorbidities among old population (≥65 years of age) at KSMC. In addition, to find out the prevalence of most associated diseases in elderly patients with diabetes.
Methods
Setting: The study took place at King Saud Medical City in Riyadh during the period from Jan 2017- Dec 2019; this is to exclude any effect of the COVID-19 pandemic and targeting most of elderly patient’s records.
Design: This study is a retrospective cross-sectional study of the database linked with patient information available from the medical files of all patients aged 65 years and older with diabetes mellitus included in this study. The data was collected retrospectively, including socio-demographic features as well as comorbidities.
Population: The geriatric patients admitted from different departments at King Saud Medical City. This study considered geriatrics as subjects aged 65 years and older have one or more chronic medical conditions including diabetes mellitus to be included.
Sample size: This study was conducted on 2853 elderly patients (65 years aged and above) whom have been diagnosed with diabetes mellitus as Inclusion criteria.
Exclusion criteria: Subjects will be excluded if they are less than 65 years, any elderly subject with other than diabetes mellitus. Any elderly subject has no medical profile in the King Saud Medical City.
Database collection: Data collection sheet template structured using Excel included age, gender BMI and the categories of the comorbidities.
Only qualified and professional candidates were chosen for data entry and data verification to present the quality and accuracy of data.
Statistical consideration
The primary hypothesis of this study is to identify the number of associated diseases in diabetic patients among the elderly and to explore the association between age and the number of comorbidities aiming to evaluate prevalence of comorbidities in elderly patients. The primary analysis will use descriptive analysis for demographic and exposure characteristics of the participants.
Results
This study was conducted own 2853 elderly patients aged 74.1 years (±7.3 SD), with average of associated diseases with diabetes mellitus of 2.68 diseases (±0.9 SD). The most associated disease in elderly patients with diabetes mellitus was hypertension with 2324 patients (81.5%), then with other heart diseases 927 patients (32.5%). Other associated diseases were explained as in detail at table 1.
|
Age (year) Number (%) |
All (n=2853) |
65-69.9 (n=972) |
70-74.99 (n=727) |
75-79.99 (n=568) |
80-84.99 (=344) |
85-89.99 (n=135) |
99 & above (n=107) |
|
|
Female
|
1219 (42.7%) |
367 (37.8%) |
298 (41%) |
279 (49.1%) |
150 (43.6%) |
63 (46.7%) |
62 (57.9%) |
|
|
Male
|
1634 (57.3%) |
605 (62.2%) |
429 (59%) |
289 (50.9%) |
194 (56.4%) |
72 (53.3%) |
45 (42.1%) |
|
|
HTN
|
2324 (81.5%) |
746 (76.7%) |
596 (82%) |
483 (85%) |
300 (87.2%) |
111 (82.2%) |
88 (82.2%) |
|
|
Asthma
|
138 (4.8%) |
47 (4.8%) |
27 (3.7%) |
31 (5.5%) |
21 (6.1%) |
6 (4.4%) |
6 (5.6%) |
|
|
Dyslipidemia
|
143 (5%) |
51 (5.2%) |
35 (4.8%) |
34 (6%) |
16 (4.7%) |
6 (4.4%) |
1 (0.9%) |
|
|
Heart Dis.
|
927 (32.5%) |
303 (31.2%) |
230 (31.6%) |
193 (34%) |
131 (38.1%) |
48 (35.6%) |
22 (20.6%) |
|
|
Lung Dis.
|
354 (12.4%) |
106 (10.9%) |
94 (12.9%) |
75 (13.2%) |
42 (12.2%) |
17 (12.6%) |
20 (18.7%) |
|
|
Renal Dis.
|
354 (12.4%) |
124 (12.8%) |
99 (13.6%) |
67 (11.8%) |
37 (10.8%) |
13 (9.6%) |
14 (13.1%) |
|
|
Rehumatic D
|
21 (0.7%) |
10 (1%) |
5 (0.7%) |
3 (0.5%) |
1 (0.3%) |
1 (0.7%) |
1 (0.9%) |
|
|
Cancer
|
98 (3.4%) |
27 (2.8%) |
27 (3.7%) |
23 (4%) |
9 (2.6%) |
9 (6.7%) |
3 (2.8%) |
|
|
Neurological
|
400 (14%) |
92 (9.5%) |
84 (11.6%) |
92 (16.2%) |
69 (20.1%) |
34 (25.2%) |
29 (27.1%) |
|
|
Mental Dis.
|
31 (1.1%) |
14 (1.4%) |
10 (1.4%) |
3 (0.5%) |
1 (0.3%) |
2 (1.5%) |
1 (0.9%) |
|
|
Number of Comorbidity
|
1 |
265 (9.3%) |
110 (11.3%) |
69 (9.5%) |
38 (6.7%) |
24 (7%) |
13 (9.6%) |
11 (10.3%) |
|
2 |
914 (32%) |
343 (35.3%) |
238 (32.7%) |
171 (30.1%) |
94 (27.3%) |
37 (27.4%) |
31 (29%) |
|
|
3 |
1197 (42%) |
391 (40.2%) |
299 (41.1%) |
261 (46%) |
152 (44.2%) |
47 (34.8%) |
47 (43.9%) |
|
|
4 |
429 (15%) |
117 (12%) |
113 (15.5%) |
83 (14.6%) |
67 (19.5%) |
36 (26.7%) |
13 (12.1%) |
|
|
5 |
45 (1.6%) |
11 (1.1%) |
8 (1.1%) |
13 (2.3%) |
7 (2%) |
2 (1.5%) |
4 (3.7%) |
|
|
6 |
3 (0.1%) |
2 (0.4%) |
1 (0.9%) |
|||||
Table 1: Frequency and percentages of associated diseases in elderly patients with diabetes mellitus along with age progressing (in year). The table showed also number of comorbidities in elderly patients with diabetes mellitus along with age progressing.
Elderly patients were associated with three comorbidities with 1197 patients (42%), then with two comorbidities 914 patients (32%), with four comorbidities with 429 patients (15%), then with one comorbidity with 265 patients (9.3%), and with 5 to 6 comorbidities with 45 patients (1.6%) and three patients (0.1%) respectively. A profile for the average numbers of associated diseases started from 2.56 diseases at age of 65 - 70 years old, then increase the profile until it reaches average of 2.83 associated diseases at age of 85 - 90 years old, then the profile become declining with age over 90 years old to reach 2.73 diseases as a minimum average of associated diseases as seen in figure 1.
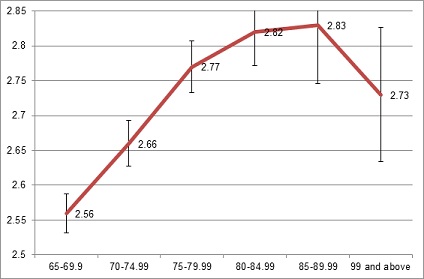 Figure 1: A profile showing the average number of associated diseases along the age progress of elderly patients with diabetes mellitus.
Figure 1: A profile showing the average number of associated diseases along the age progress of elderly patients with diabetes mellitus.
Results showed that number of old patients with DM become reduced as the age progress with -180 patients (15.85% of the patients) every five years. Another profile for elderly patients with diabetes showing reduction in number of elderly with diabetes mellitus with average of -180 patients every five years figure 2.
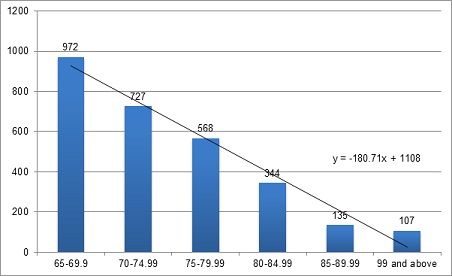
Figure 2: Prevalence of elderly patients with diabetes mellitus, showing a declining in number of patient with -180 patients every five years.
Male elderly patients with diabetes mellitus were 1634 with (57.3%) compared with the female elderly patients with diabetes mellitus of 1219 patients (42.7%). Saudi patients were the most prevalence with 2061 patients (72.2%) compared with Arabic middle east with 461 patients (16.2%), then African countries with 209 patients (7.3%), then Asian and far east with 117 with patients (4.1%), and lastly with five patients (0.2%) from American and European countries.
Discussion
The association of DM with cardiovascular diseases in older population was described in previous study [19], and here will discuss the associated comorbidities among old people with diabetes mellitus. Results showed that 2853 old patients with average aged of 74.1 (±7.3 SD years), and with average of associated diseases with diabetes mellitus of 2.68 diseases (±0.9 SD), which is less, compared with associated diseases with cardiovascular diseases of 2.61 diseases (±1.1 SD) with no significant difference (p<0.05). Diabetes in older patients was mostly associated with hypertension with 2324 patients (81.5%), then with cardiovascular diseases with 927 patients (32.5%). A similar results were found that cardiac failure was frequently associated with elderly diabetics, considering the worst scenario with old female diabetics [20].
Association of diseases with DM in older patients was varied and ranging from one disease and reach up to six diseases; however the most frequent association was with three comorbidities with 1197 patients (42%), then with two comorbidities 914 patients (32%). The most important findings for this study were a profile for the average numbers of associated diseases along the age progress. The profile showed the average number of associated diseases started from 2.56 diseases at age of 65 - 70 years old, then increase the profile until it reaches average of 2.83 associated diseases at age of 85 - 90 years old as the peak average of associated diseases. The profile become declining with age over 90 years old to reach 2.73 diseases as a minimum average of associated diseases, which is the same interpretation for diabetes mellitus among the Canadian elderly people showed the incidence of the DM declining among the very old [21]. There were 180 patients declining every five years showing 15.85% of number of the old patients with DM becomes reduced as the age progress every five years. The increased declining of DM patients in older patients for more than 180 patients every five years after 70 years old is a resultant of death; however it has been noticed in this study that the declining of associated comorbidities was reduced after 90 years old.
A controversy results showed in the results of this study for male elderly patients with diabetes mellitus were 1634 with (57.3%), as higher percentage compared with the female elderly patients with diabetes mellitus of 1219 patients (42.7%), unlike previous study showed that older women (older than 65) with diabetes were with higher percentage compared to older men with diabetes in the USA [22]. Although pulmonary and renal diseases were considered as 12.4% associated with DM in elderly patients suggested that albuminuria and low glomerular filtration rate are associated with frontal lobe dysfunction in elderly type 2 diabetic patients [23]. Moreover in the elderly, male sex, diabetes, insulin therapy and high C-peptide immune reactivity levels were considered as risk factors [24]. Saudi patients were the most prevalence with 2061 patients (72.2%) compared with Arabic Middle East with 461 patients (16.2%) and other nationalities with (11.6%).
Early diabetes awareness should be a step had been done earlier for all old patients with diabetes. The most important part is how to deliver adequate standards to reduce hospitalization to reach appropriate management to DM specifically and to prevent the associated diseases. Seeking of signs and symptoms of the predicted comorbidities to plan for self-care and good monitoring is the first priority for the older patients with diabetes [25,26]. It is also important to investigate for the signs and symptoms in patients with DM on age processing in order to find advice and to ask for support before DM or its complications become more difficult [27]. Diabetes self-care monitoring is complex with important recommendations for dietary requirements, physical activity, checking glucose levels, taking medication, modification of lifestyle, adjusting environment factors such as lifestyle and eating habits, information about diabetes, and motivation and support [28,29].
Specific health promotion programs for older patients with diabetes should be organized to promote knowledge and awareness about diabetes self-care will result in healthier environment. Reduced the duration of occurrence of chronic complications [30]. Diabetes self-care monitoring is complex with important recommendations to deliver adequate standard to reduce hospitalization to reach appropriate management to DM specifically and to DM comorbidities.
Conclusion
The average of associated diseases with diabetes mellitus of 2.68 diseases (±0.9 SD) for the elderly patients with average of their age of about 74 years. The most frequent disease associated with diabetes mellitus was hypertension with 81.5% then cardiac diseases with 32.5%. This study showed that male elderly patients with higher percentage compared with the female elderly patients with diabetes mellitus. There were 15.85% of elderly patients with DM declining every five years and the profile become reduced as the age progress. Diabetes self-care monitoring is complex with important recommendations for dietary requirements to deliver adequate standard to reduce hospitalization to reach appropriate management to DM.
Highlights
- The average of associated diseases for the elderly with diabetes mellitus was 2.68 diseases (±0.9 SD)
- The most frequent diseases associated with diabetes mellitus was hypertension with 81.5% then cardiac diseases with 32.5%
- Elderly male patients were with higher percentage compared with the female elderly patients with diabetes mellitus
- There were 15.85% of elderly patients with DM declining every five years and the profile become reduced as the age progress
Ethical Consideration
This study was approved by the King Saud Medical City, Institutional Review board, IRB Registration Number with KACST, KSA: H-01-R-053 under a reference number : H1RI-02-Jul20-02.
Sponsorship
Nil.
Conflict of Interest
None declared.
References
- Menke A, Casagrande S, Geiss L, Cowie CC (2015) Prevalence of and trends in diabetes among adults in the United States, 1988-2012. JAMA 314: 1021-1029.
- Milanesi A, Weinreb JE (2020) Diabetes in the Elderly. Endotext [Internet].
- Alqurashi KA, Aljabri KS, Bokhari SA (2011) Prevalence of diabetes mellitus in a Saudi community. Ann Saudi Med 31: 19-23.
- American Diabetes Association (2020) Standards of Medical Care in Diabetes-2020 Abridged for Primary Care Providers. Clin Diabetes 38: 10-38.
- Yang W, Li Y, Tian T, Wang L, Lee P, et al. (2017) Serum vaspin concentration in elderly patients with type 2 diabetes mellitus and macrovascular complications. BMC Endocr Disord 17: 67.
- Chentli F, Azzoug S, Mahgoun S (2015) Diabetes mellitus in elderly. Indian J Endocrinol Metab 19: 744-752.
- Alsuwaidan S, Algharbi A, Alyami S, Almukhlifi N (2021) Prevalence of Comorbidity Among Elderly. Glob J Aging Geriatr Res 1: 2021.
- Al Dawish MA, Robert AA, Braham R, Al Hayek AA, Al Saeed A, et al. (2016) Diabetes mellitus in Saudi Arabia: a review of the recent literature. Curr Diabetes Rev 12: 359-368.
- Gregg EW, Engelgau MM, Narayan V (2002) Complications of diabetes in elderly people: Underappreciated problems include cognitive decline and physical disability. BMJ 325: 916-917.
- Croxson SCM, Price DE, Burden M, Jagger C, Burden AC (1994) The mortality of elderly people with diabetes. Diabetic Med 11: 250-252.
- Ministry of health Saudi Arabia (2020) Elderly Health. Ministry Of Health, Saudi Arabia.
- Alsuwaidan A, Almedlej N, Alsabti S, Daftardar O, Al Deaji F, et al. (2019) A comprehensive overview of polypharmacy in elderly patients in Saudi Arabia. Geriatrics (Basel) 4: 36.
- Veronese N, Kolk H, Maggi S (2020) Epidemiology of fragility fractures and social impact. In: Falaschi P, Marsh D (eds.). Orthogeriatrics: The Management of Older Patients with Fragility Fractures (2ndedn) Springer, Berlin, Germany.
- Benbow SJ, Walsh A, Gill GV (2001) Brittle diabetes in the elderly. J R Soc Med 94: 578-580.
- Griffith DNW, Yudkin JS (1989) Brittle diabetes in the elderly. Diabetic medicine 6: 440-443.
- Jolobe OMP, Khin N (2002) Brittle diabetes in the elderly. J R Soc Med 95: 58.
- Mather HM (1994) Diabetes in elderly Asians. Journal of the Royal Society of Medicine 87: 615.
- Corriere M, Rooparinesingh N, Kalyani RR (2013) Epidemiology of diabetes and diabetes complications in the elderly: An emerging public health burden. Curr Diab Rep 13: 805-813.
- Alyami SS, Algharbi A, Alsuwaidan S (2022) Characteristics of Associated Diseases in Older Patients with Cardiovascular Disease. Advances in Aging Research 11: 151-161.
- Day JJ, Bayer AJ, Chadha JS, Pathy MS (1988) Myocardial infarction in old people. The influence of diabetes mellitus. J Am Geriatr Soc 36: 791-794.
- Rockwood K, Awalt E, MacKnight C, McDowell I (2000) Incidence and outcomes of diabetes mellitus in elderly people: Report from the Canadian Study of Health and Aging. CMAJ 162: 769-772.
- Morley JE, Mooradian AD, Rosenthal MJ, Kaiser FE (1987) Diabetes mellitus in elderly patients. Is it different? Am J Med 83: 533-544.
- Umemura T, Kawamura T, Umegaki H, Kawano N, Mashita S, et al. (2013) Association of chronic kidney disease and cerebral small vessel disease with cognitive impairment in elderly patients with type 2 diabetes. Dement Geriatr Cogn Dis Extra 3: 212-222.
- Ishii M, Yamaguchi Y, Hamaya H, Ogawa S, Imura M, et al. (2019) Characteristics of factors for decreased lung function in elderly patients with type 2 diabetes. Sci Rep 9: 20206.
- Weinger K, Beverly EA, Smaldone A (2014) Diabetes self-care and the older adult. West J Nurs Res 36: 1272-1298.
- Emine E, Sevgi K, Ezgi Ü, Melike B (2020) Care Dependency and Diabetes Self-Care Activities in Elderly Individuals with Diabetes. Elderly Health Journal 6.
- Caughey GE, Roughead EE, Vitry AI, McDermott RA, Shakib S, et al. (2010) Comorbidity in the elderly with diabetes: Identification of areas of potential treatment conflicts. Diabetes Res Clin Pract 87: 385-393.
- Asiimwe D, Mauti GO, Kiconco R (2020) Prevalence and risk factors associated with type 2 diabetes in elderly patients aged 45-80 years at Kanungu District. Journal of diabetes research 2020.
- Pennbrant S, Berg A, Johansson LF (2019) Self-care experiences of older patients with diabetes mellitus: A qualitative systematic literature review. Nordic Journal of Nursing Research 40: 64-72.
- Watcharanat P, Khuancheree K, Lee B (2021) Factors Associated with Self-Care Behavior of Elderly Patients with Type 2 Diabetes in Thailand. The Open Public Health Journal 14: 494-497.
Citation: Algharbi A, Alyami S, Alsuwaidan A, Alsuwaidan S (2022) Diabetes Mellitus among Old People and Associated Comorbidities. J Gerontol Geriatr Med 8: 154.
Copyright: © 2022 Abrar Algharbi, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.