Ear map or RAC in Ear Acupuncture, Comparison of Different ear Maps and Interpretation of their Differences
*Corresponding Author(s):
Gerhard RiehlFacharzt Für Allgemeinmedizin, Naturheilverfahren, Akupunktur, Essen, Germany
Tel:+49 1739198001,
Email:mail@dr-riehl.com
Abstract
Since the ear somatotope was first published in 1957 by P. Nogier there was intensive further developement of maps for ear acupuncture by various researchers and schools. Nowadays we see some differences in the location of therapeutic points between the schools` mappings. These differences led to uncertainties about the reliability of the mappings. Some factors of the differences found are discussed. Furthermore the differences between french school and RAC-related ear acupuncture in particular will be shortly discussed with reference to an article from 2021 [1,2].
Keywords
Ear Acupuncture; Ear Maps; RAC
Basic Remarks on the Compared maps Für Ear Acupuncture
After the first known publication of a map for auricular acupuncture by Paul Nogier in “Dtsch. Ztschr. F. Akupunktur” 1957 [3] there were several further map drafts of the auricular representations. After a first Chinese Publication of an ear card by Dr. Xu Zuo-Lin in Beijing 1959 after the clinical validation of 255 patients [4] there were published several more mappings. For example a textbook with the title "The Therapy of Acupuncture Ear Needling" was published by the "Shanghai City Auricular Acupuncture Study Group" quoted by Bucek, [5].
There were slight differences in the comparison of the maps, which led to the differentiation of a French school and a Chinese school and, due to differences in the localization of some representations, led to questions about the correctness of the point localizations [2]. In addition a Viennese school and a Russian school were founded, but using the vegetative "RAC" or “Nogier-reflex” -also discovered by Paul Nogier -, an additional German school developed under the leadership of F. Bahr. [6,7]. With the help of this RAC-reflex, the exact activated point on the auricle could be determined and needled.
Testing the exact activated point via the RAC proved very fruitful and produced a large number of other points, especially as points could be detected that were not found by means of pressure methods or electrical testing.
There were other points in both the Chinese mapping and the Bahr mapping that went beyond the purely anatomically and physically oriented original mapping by Nogier, for example the “ShenMen” point in the Chinese schools, several points from the RAC-guided search with psychologically effective reactions. But the localization of anatomical points on different maps also showed differences [4,5,7-9].
Comparison of the French School and the Bahr School Using RAC
In 2013, T. Ots formulated the question of how these differences come about [2]. Do the different localizations result from personal ambition, from different test methods, are there multiple representations of an anatomical organ, or are some localizations simply wrong?
For individual comparisons of various points, I refer to my main article from 2021 [1]. In the present review I limit myself to the results and conclusion.
Conclusion
In principle, mapping of the auricle has proven very useful for teaching and in the search for a representation of the symptom to be treated. This applies both to the mapping of the French school and to the school of RAC-based point detection.
Regarding the differences: In my article “RAC or ear map” [1] about the comparison of different mappings of the auricle, with special reference to the maps of Rubach (Deutsche Ärztegesellschaft für Akupunktur) [8] and the school of Bahr and Strittmatter [6,7], I came to the conclusion that multiple factors are responsible for the differences in the mappings.
I identified three factors that are partly responsible for the differences. First of all, it has to be taken into account that, despite the known basic structure of the auricle, each auricle also has its own structure, as was shown for example by Rubach in his book [8] with a number of examples. The lobule for example is formed very differently, the antihelix with its representation of the spinal segments varies in its width and the sections of the different spinal regions of cervical, thoracic and lumbar spine distend differently depending on the patient (Figures 1-3).
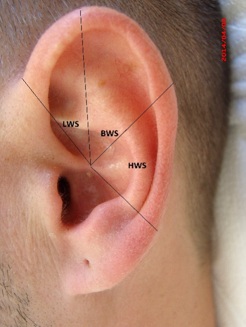 Figure 1: Examples of different ear shapes.
Figure 1: Examples of different ear shapes.
 Figure 2: Examples of different ear shapes.
Figure 2: Examples of different ear shapes.
 Figure 3: Examples of different ear shapes.
Figure 3: Examples of different ear shapes.
The same applies to the triangular fossa or the depiction of the arm and shoulder and much more. The auricle seems to be as different as a fingerprint. This makes it almost impossible to localize exact anatomical points for all patients on a fixed map - with a known basic structure of the auricle, there are always deviations that require exact localization of the activated point before therapy, using electrical methods or the RAC.
Secondly, as early as 2013, in my article on the localization of the large leg joints [10], I pointed out that the activated point for pain over the hip or knee joint pain is not found at the exact same point in different patients. Depending on the patient and the point of pain above the joint, the activated points found via RAC on the auricle also differ in a typical slightly expanded region (Figure 4).
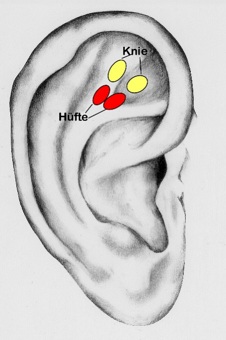 Figure 4: Scattering of the activated points for knee joint and hip.
Figure 4: Scattering of the activated points for knee joint and hip.
[10] Regions of the French and Chinese schools on which to find and specify the activated point for hips and knees. In the Chinese school on the crus superior, in the French school in the intercrural fossa.
This leads to the conclusion that inspite knowledge of the auricular structure, one should detect the activated point before needling in the region of the mapped point, in order to find the best therapy point.
Considering these criteria - the differences in ear anatomy, as well as looking for representative regions rather than points - most of the anatomical points of these schools are already reasonably compatible.
The third thing to observe is, that the greatest differences between different maps are found in the localization of psychic points. Some point categories are not present in both maps. But it seems plausible that categories such as "depression," "grief," "despair," and other psychoemotional labels depend on the therapist's interpretation of the symptomatology and do not appear entirely uniform. If, for example, depressive symptoms improve under therapy, which acupuncture doctor can say exactly which previously undefined psychological component was responsible for the improvement in the depressive symptoms? Was the improvement caused by previous painful experiences, an improved ability to look ahead, a change in serotonin levels, or something else entirely? These factors are very likely to have different therapeutic representations on the auricle- the type of detection method also plays a major role here. Many activated points in connection with psychological symptoms, which are clearly found with the RAC, cannot be detected electrically.
Summary
Taking into account the individual ear shape variations and the differently extended representation of different spinal column sections on the auricle, different pain locations in or on the affected joint, a fixed mapping will be very helpful for the point search and the teaching. But in the individual treatment case, despite various good maps, the mapped point cannot be transferred exactly. A map does not replace the individual search for the maximum activated representation on the auricle, ideally by using RAC.
Besides experience shows that no fixed point was found for psychological points such as the representation of mental injuries [11]. The representative point for mental injury or trauma must be detected on a case-by-case basis above the lobule. These points do not react at all to the electrical detection method, but can only be found using the RAC so far.
Therefore, from my point of view, even if you know a good mapping, the exact localization of the maximum activated point in the area should always be sought with a current detection, ideally with the RAC.
References
- Riehl G (2021) Diagnostik und Therapie nach Ohrkarte oder nach RAC? Deutsche Zeitschrift für Akupunktur 64(1):55-60.
- Ots T (2013) Zu klärende Fragen in der Ohrakupunktur (Teil1). Dt Ztschr f Akup 56(1):18-22.
- Paul N (1957) Über die Akupunktur der Ohrmuschel Dtsch. Zeitschrift für Akupunktur 6: 25-33.
- Romoli M (2010) Ear Acupuncture: Historical Abstract. Dt Ztschr f Akup 53(4):24-33.
- Bucek R (2000) Praxis der Ohrakupunktur. Haug Verlag, Heidelberg, Germany.
- Bahr F, Strittmatter B (2014) Das große Buch der Ohrakupunktur.2. Aufl. Haug Verlag, Stuttgart, Germany.
- Strittmatter B (2017) Taschenatlas Ohrakupunktur nach Nogier/Bahr,6. Überarbeitete Auflage, Stuttgart, Haug Verlag, Germany.
- Rubach A (2000) Propädeutik der Ohrakupunktur. Hippokrates, Stuttgart, Germany.
- Angermaier M (2017) Leitfaden der Ohrakupunktur- Mit französischen und chinesischen Punkten. Elsevier, München, Germany.
- Riehl G (2013) Vergleich verschiedener Repräsentationspunkte der großen Beingelenke in der Ohrakupunktur. Dt Ztschr F Akup 56(4):6-8.
- Bahr FR, Wesemann CT (2020) Psychische Verletzungen- Seelische Traumen“ Eigenverlag. C Version 1.1, München, Germany.
Citation: Riehl G (2022) Ear map or RAC in Ear Acupuncture Comparison of Different ear Maps and Interpretation of their Differences. J Altern Complement Integr Med 8: 293.
Copyright: © 2022 Gerhard Riehl, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.