Effectiveness of Auricular Acupressure for Post-Stroke Constipation: A Systematic Review and Meta-Analysis
*Corresponding Author(s):
Irene J SuShantou University Medical College, Shantou, China
Tel:+1 2488738894,
Email:suirene@hotmail.com
Abstract
Background: Post-stroke constipation was very common in clinical setting. Auricular acupressure was increasingly being used in the management of functional constipation.
Objective: This study aimed to systematically examine the effectiveness of auricular acupressure in the management of post-stroke constipation.
Method: A systematic search of the following databases was conducted: Cochrane Library, Pubmed, Web of science, China National Knowledge Infrastructure (CNKI), Wan Fang database, Chinese Biomedical Literature (CBM), and China Science and Technology Journal to identify relevant studies of randomized controlled trials on the efficacy of auricular acupressure in the treatment of constipation among stroke patients from inception of the database to April 2021. Quality of the included studies was evaluated using Cochrane Reviewer's Handbook 5.1.0. Data were analyzed using RevMan 5.3 software.
Result: A total of 899 patients were included in the ten randomized controlled trials. The experimental group treated with auricular acupressure had a better overall clinical effectiveness rate than the control group (OR=5.15, 95% CI [3.45, 7.69], P < 0.00001). Three studies used the clinical symptom score for constipation post intervention as an evaluation index. The experimental group was also superior to the control group. In addition, compared with the control groups, auricular acupressure had fewer adverse effects.
Conclusion: The preliminary findings of this study concluded that auricular acupressure was an effective and safe measure of intervention for the management of post-stroke constipation. We are hoping to see more high-quality studies to validate this result to disseminate the evidence-based practice of Traditional Chinese medicine (TCM).
Keywords
Auricular Acupressure; Meta-analysis; Post-Stroke Constipation; Traditional Chinese Medicine; Stroke
Introduction
Stroke now ranked as the second leading cause of death and the primary cause of disability around the globe, with dramatically increased burden [1,2]. Many gastrointestinal complications could occur in stroke patients, such as dysphagia, constipation, gastroduodenal ulcers, and fecal incontinence. Of note, post-stroke constipation was very common in clinical setting [3]. A systematic review showed that the prevalence of constipation in stroke patients was 48% [4]. This complication could reduce the quality of life, increase hospital length of stay, and even cause the recurrence of cerebrovascular diseases [3,5,6].
Currently, there was still a lack of fundamental solution for post-stroke constipation globally. Western medical treatments such as oral laxatives, glycerin anal suppositories, and enemas could partially relieve constipation symptoms, but could not essentially improve the patient's bowel function. These strategies usually hadmany side effects [7]. Lifestyle or diet modifications were found to improve the condition [8]. However, hemiplegia and dysphagia often occurred among stroke patients, making these methods more difficult to implement.
To date, with the rapid development of auricular acupressure, it was increasingly used in the management of functional constipation [9,10]. Auricular acupressure guided by the theory of Traditional Chinese Medicine (TCM), used small hard and smooth seeds or pills to apply pressure to ear acupuncture points and stimulate these points with mechanism of action similar to that of acupuncture therapy [11]. Our literature search did not find any systematic review and meta-analysis on the effectiveness and credibility of this treatment method. Therefore, the purpose of this study aimed to systematically examine the effectiveness of auricular acupressure in the management of post-stroke constipation to provide empirical evidence for clinical practice.
Methods
Search strategy
The following database were searched for relevant studies in the Chinese and English languages: Cochrane Library, Pubmed, Web of Science, China National Knowledge Infrastructure (CNKI), Wan Fang Database, Chinese Biomedical Literature (CBM), and China Science and Technology Journal Database from their inception to April 2021. The search strategy included MeSH terms and their associated free words. The Chinese search terms were: “cu zhong” (stroke) and “zhong feng” (stroke); “bian mi” (constipation), and “pai biankun nan” (difficult defecation); “er xue” (ear points), “er ya” (ear pressure), “er xue tie ya” (auricular acupressure), “er xueyadou” (ear acupressure bean),and “er xuezhiliao” (auricular point treatment).The English search terms were: “stroke”, “cerebrovascular accident”, “apoplexy”, and “brain vascular accident”; “constipation”, “dyschezia”, “colonic inertia”, and “astriction”; “auricular point”, “ear point”, “semen vaccariae”, “auricular point sticking”, “auricular point pressing”, “auricular plaster therapy”, and “application of auricular pressure”.
Selection criteria and literature data extraction
Inclusion criteria: (1) Study type: Randomized controlled clinical trials. (2) Study subjects: Patients with post-stroke constipation. (3)Intervention: Auricular acupressure. (4)Control: Blank control or conventional care according to guidelines (details shown in table 1 in section 3.3.)(5) Primary outcome: Clinical effectiveness rate; Secondary outcome: Constipation symptom score and adverse effects.
Exclusion criteria: (1) Unpublished or duplicate studies, conference abstracts, and case reports.(2) Study with unclear evaluation criteria for efficacy. (3)Study without primary outcome. (4)Studies with combination of auricular acupressure and other TCM treatment methods.
Two investigators independently conducted literature screening based on the inclusion criteria and extracted data from included studies. In the case of disagreement or discrepancy, the investigators would discuss to negotiate a solution until an agreement was reached. The following information was extracted: author, year of publication, number of participants, average ages, acupoint selection, type of stimulator, method of seed taping on ear, time and frequency of acupressure, frequency of seed replacement, clinician who applied the intervention, and outcome indicators.
Methodological quality
The quality assessment criteria for randomized controlled trials was based on the Cochrane Reviewers' Handbook [12], which included the following six items: random sequence generation, allocation concealment, blinding of participants, blinding of outcome assessment, incomplete outcome data, selective reporting, and other concerns about bias. Two investigators independently rated the above areas as “low risk” (low degree of bias), “high risk” (high degree of bias), and “unclear” (lack of relevant information or uncertain bias). If there was a disagreement, it would be resolved through discussion or the assistance of a third evaluator.
Statistical analysis
Data were analyzed using RevMan 5.3 software. Continuous variables were analyzed using the weighted mean difference (WMD) and its 95% confidence interval (CI) as the indicator statistic. The odds ratio (OR) was adopted for dichotomous variables, and 95% CI was calculated. The results of the included studies were examined for heterogeneity using the χ2 test. When there was no heterogeneity or low heterogeneity (P≥0.1 or I2≤50%), the fixed effects model was used. Conversely, when there was significant heterogeneity (P2>50%), the random effects model was used. In addition, a funnel plot was used to analyze whether there was a publication bias.
Results
Study selection
377 articles were identified. Duplicate articles were excluded (n=271). The initial screening excluded 90 articles based on the abstract or tile alone. After reading 16 full-text articles, 10 articles published in the Chinese language were retained strictly in accordance with the inclusion criteria and none in English was selected. The PRISMA flow chart is shown in figure 1[13].
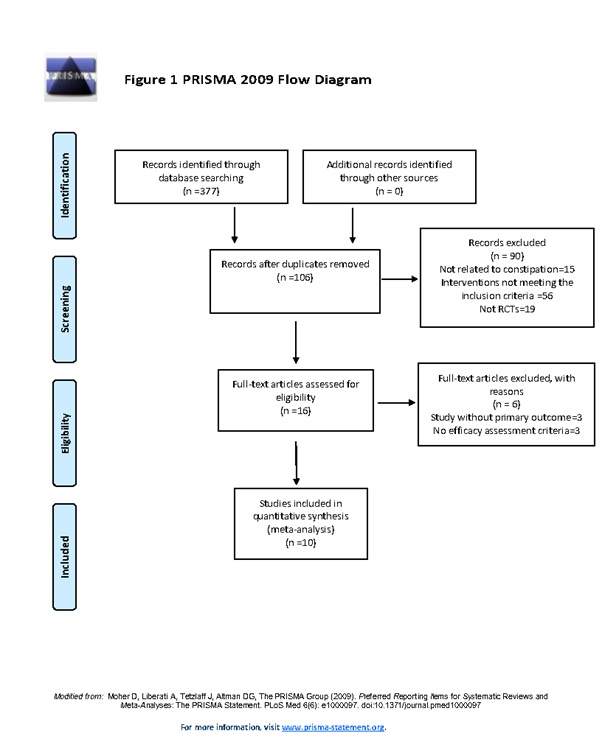 Figure 1: PRISMA flow chart.
Figure 1: PRISMA flow chart.
Methodological quality
The 10 included studies were evaluated for literature quality. Details of the quality assessment of all included studies are shown in figure 2.
 Figure 2: Risk of bias summary.
Figure 2: Risk of bias summary.
Characteristics of studies
A total of 899 patients were included in the ten randomized controlled trials with 340 women and 559 men [14-23]. These research subjects were all hospitalized patients in general hospitals or hospitals of Chinese medicine. Because the control group utilized a variety of conventional treatment methods, table 1 offers a brief summary. The experimental group added auricular acupressure to the conventional interventions. This study evaluated 3 outcome indicators: clinical effectiveness rate, clinical symptom score of constipation, and adverse effects. The included studies used two methods to grade the clinical efficiency. Three of these studies [15,18,21] adopted the Guidelines for Clinical Research on New Chinese Medicines and seven studies [14,16,17,19,20,22,23] adopted the Diagnostic and Efficacy Criteria for Chinese Medical Evidence. Based on the Guidelines for Clinical Research on New Chinese Medicines [24], the criteria for cure would be met if defecation occurred within 2 days, with moistened stool, easy defecation, and resolution of related symptoms. The criteria for significant effects were: Defecation within 2 days, with moistened stool, difficult defecation, and relief of constipation symptoms. The criteria for effectiveness were: Defecation within 3 days, with dry stool followed by soft stool, difficult defecation, and relief of constipation symptoms. Ineffectiveness was no improvement of constipation symptoms. According to the Diagnostic Efficacy Criteria for Chinese Medicine [25], the criteria for cure were one bowel movement within 2 days, with moistened stool, and easy defecation with no short-term recurrence of symptoms. The criteria for improvement were bowel movement within 3 days, with moistened stool, and difficult defecation. The criteria for failure to cure were no improvement in symptoms. Three studies used clinical symptom scores for constipation, which included time of first defecation, urge to defecate, degree of difficulty, defecation speed, characteristics of stool, and time between bowel movements. Only two studies [18,20] reported adverse effects. Specific characteristics of the included studies are shown in table 2.
|
First author, Year |
Conventional interventions |
|
Jia Guo, |
Standard protocol to treat constipation for stroke patients as prescribed by the medical provider. |
|
Aiping Qian |
Routine guidance and health education: (1) Patient education such as cause of constipation. (2) Dietary guidelines. (3) Instruction for abdominal massage. (4) Provide a comfortable and secluded environment for patients and develop regular bowel habits. (5) Psychological support. |
|
Hui Yin |
Health guidance: (1) Psychological support. (2) Personalized dietary guidance. (3) Develop regular bowel habits. |
|
Jie JI |
(1)Explanation to patients and their families about the risk of constipation and its hazards. (2) Dietary guidelines. (3) Psychological support. (4) Medication protocol: Those who did not have a bowel movement for 3 days were given glycerine enema to assist with bowel movement. |
|
Limin Lv |
Routine therapeutic interventions: (1) Routine treatment of stroke according to guidelines. (2) Patient education on pathophysiology of the disease. (3) Psychological support. (4) Bowel training: Instruct patients to exercise their abdominal and pubicmuscles. (5) Timed bowel training. (6) Instruct patients on personalized rehabilitation exercises. (7) Develop a dietary plan. (8) Oral phenolphthalein, 2 tablets, once daily at bedtime for 2 weeks. |
|
Qing Wang |
Conventional method of care: (1) Daily care: Personalized strengthening exercise, meticulous hygiene practice. (2) Medication adherence: Lactulose oral solution 3 times daily as needed. (3) Dietary guidelines. |
|
Chunying Zhang |
(1) Medication guidance: Take 2 laxative capsules orally at bedtime every night as prescribed. (2) Dietary guidelines. (3) Abdominal massage. (4) Psychological support. |
|
Changxi Yu0 |
Routine care and health guidance: (1) Patient education on risks of constipation and hazards of straining for bowel movements. (2) Dietary guidelines. (3) Instruct patients on exercise and defecation habits in bed. (4) Instruct patients to develop good bowel habits. |
|
Bichou Cai |
(1) Dietary guidance. (2) Instruct patients to develop good bowel habits. (3) Abdominal massage. |
|
Hongmei Xu |
Routine nursing interventions: (1) Dietary guidelines. (2) Medication compliance with laxatives as prescribed. |
Table 1: Description of conventional treatments in the control group.
|
First author& year |
No. of participants (T/C) |
Mean age ±SD in years at baseline (T/C) |
Acupoint Selection |
Stimulator |
Method of Seeds Taped on Ear |
Time and Frequency of Acupressure |
Frequency of seed replacement |
clinician who applied the intervention |
Outcome indicators |
|
Jia Guo |
90/90 |
61.52±4.88/ 61.51±4.84 |
Subcortex, Spleen, Sanjiao, Rectum, Lung, Small intestine |
Vaccaria seeds |
NR |
30 seconds for eachacupoint, 4 times a day for 14 days |
2-3d |
Nurse |
A, B
|
|
Aiping Qian
|
42/42 |
37.1/31.1 |
Large intestine, Sanjiao, Spleen, Abdomen, Digestive Systemic Subcortex, Lung, Sigmoid colon |
Vaccaria seeds |
Alternate ear |
3 to 5 minutes each time, 2 to 3 times daily for 14 days |
2-3d |
NR |
A |
|
Hui Yin
|
60/60 |
NR |
Large intestine, Small intestine, Rectum, Sanjiao, Endocrine, Lung, Spleen, Kidney |
Vaccaria seeds |
Alternate ear |
60 seconds for each acupoint, 3 to 5 times a day for 60 days |
NR |
NR |
A |
|
Jie JI
|
40/40 |
61.3±8.6/ 59.6±9.7
|
Rectum, Large intestine, Lung, Sanjiao, sympathy, Constipation point |
Vaccaria seeds |
Alternate ear |
3 minutes each time,3 times daily for 8 days |
NR |
NR |
A, B |
|
Limin Lv
|
30/30 |
66.13±5.81/ 65.20±5.17 |
Large intestine, Lower rectum, Lung, Constipation point, Subcortex, Stomach, Sanjiao, Spleen, Kidney |
Magnetic seeds |
Alternate ear |
3 minutes for each eachacupoint , 4 times a day for 14 days |
3d |
Trained personnel |
A, B, C
|
|
QingWang |
30/30 |
56.5±0.8/ 56.7±0.8 |
Large Intestine, Small Intestine, sympathy, Kidney, Spleen, Sanjiao |
Vaccaria seeds |
Alternate ear |
1 to 2 minutes each time, 2 to 3 times daily |
2-3d |
NR |
A |
|
Chunying Zhang
|
40/40 |
71.46±4.32/ 70.21±5.12 |
Constipation point, Large Intestine, Spleen, Sanjiao |
Vaccaria seeds |
Alternate ear |
3 minutes each time, 3 times daily |
3d |
NR |
A, C |
|
Changxi Yu |
50/50 |
41±7.28/ 43±6.89 |
Lung, Stomach, Large intestine, Small intestine, Sigmoid colon, Sanjiao, Spleen, Kidney, Endocrine, Shenmen |
Vaccaria seeds |
Alternate ear |
3 minutes for eachacupoint, 3 times a day for 15 days |
4-5d |
Patients |
A |
|
Bichou Cai |
28/28 |
57±20/ 56±20 |
Lung, Stomach, Large intestine, Small intestine, Sanjiao |
Vaccaria seeds |
Alternate ear |
1 to 2 minutes for each acupoint, 2 to 3 times a day for 28 days |
3d |
NR |
A |
|
Hongmei Xu |
40/39 |
58.48±9.01/ 60.46±7.34 |
Large intestine, Sanjiao, Constipation point, Spleen |
Vaccaria seeds |
Alternate ear |
20 seconds for Eachacupoint, 3 to 4 times a day |
3-5d |
NR |
A |
Table 2: Characteristics of the included studies.
A= clinical effectiveness rate; B= Constipation clinical symptom score; C= adverse events
Abbreviations: NR= not reported
Effectiveness of auricular point acupressure for constipation
Comparison of clinical effectiveness rate: All included studies used the overall effective rate as an evaluation indicator. Of the 899 patients included in the studies, 450 were in the experimental group and 449 were in the control group respectively. No significant heterogeneity was observed among these studies (P=0.28, I2=18%). Therefore, the fixed effects model was used. The results showed that the group using auricular point acupressure had a better overall clinical effectiveness rate than the control group (OR=5.15, 95% CI [3.45, 7.69], P < 0.00001, Figure 3).
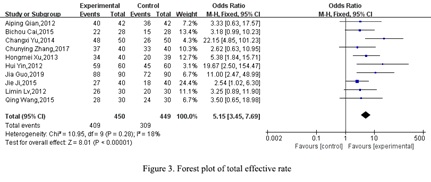 Figure 3: Forest plot of total effective rate.
Figure 3: Forest plot of total effective rate.
Constipation symptom score: Constipation symptom scores were used by three studies, two of which [14,17] reported the score of constipation clinical symptoms post intervention with the finding of a statistically significant difference between the experimental and control groups (WMD=-1.11, 95% CI [-1.15, -1.07], P < 0.00001, Figure 4).In addition, one study [18] reporting individual symptoms of constipation found no statistically significant differences in terms of characteristics of stool between the experimental and control groups while other symptom categories demonstrated statistically significant differences.
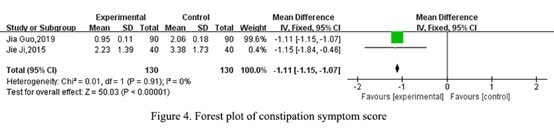 Figure 4: Forest plot of constipation symptom score.
Figure 4: Forest plot of constipation symptom score.
Reports of adverse events
One study [20] reported that two patients in the experimental group had mild itching of the skin at the ear points due to alcohol allergy during the intervention period, with resolution of the discomfort after discontinuation of the use of alcohol swabs. Another study [18] found the difference between the two groups in terms of diarrhea or recurrence of constipation after stopping the intervention was statistically significant. Overall, the experimental group had fewer adverse events than the control group.
Publication bias
A funnel plot analysis of clinical effective rate was performed as displayed in figure 5. The results showed that there was no publication bias in the clinical efficacy of constipation treatment.
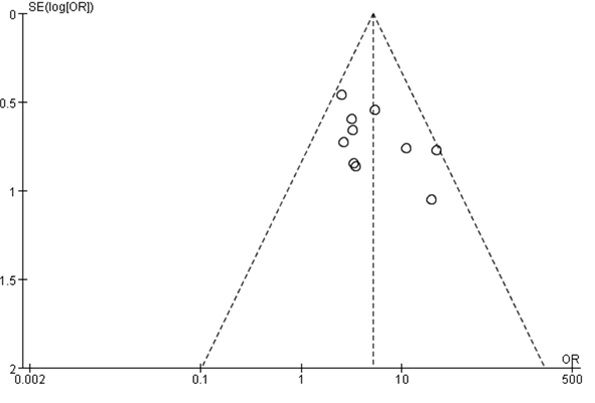 Figure 5: Funnel plot of publication bias.
Figure 5: Funnel plot of publication bias.
Discussion
Effectiveness and safety of auricular acupressure for post-stroke constipation.
The result of this meta-analysis suggested that auricular acupressure was safe and could be an effective treatment method for post-stroke constipation. Other studies also reported remarkable clinical efficacy of auricular acupressure in preventing the development of constipation after stroke [26,27]. One of the included studies [18] showed that there was no statistically significant difference between the scores of defecation traits of the two groups. It may be related to the mechanism of action of phenolphthalein in conventional treatment to prevent the intestinal wall from absorbing water resulting in softened stool. In the experimental group, there was no recurrence of constipation two weeks post cessation of the intervention. This may be attributed to the continuous effect of auricular acupressure, which targeted both the symptoms and the root cause. The etiology of post-stroke constipation was not well understood. The cause of the disorder was believed to be multi-factorial. Constipation after stroke may be related to neurocentral damage, changes in diet and bowel habits, prolonged bed rest, and depression or anxiety [28]. It was of interest to note that the use of evidence-based dietary and auricular pressure interventions for stroke patients could also effectively improve sleep quality and neurological deficits and alleviate anxiety or depression [29].
Although the application of acupuncture points was generally consistent, the selection and localization of auricular points were not clearly referenced to sources and without detailed descriptions in the included studies. Most of the studies were guided by either conventional wisdom or prior experience of success in the choice of auricular points. Unfortunately, only two studies reported on the dialectical application of acupressure points. Such an approach followed the belief of TCM where constipation was classified as deficiency and excess [30]. The treatment for the condition of excess was based on heat circulation and dissipation. The management of deficiency was primarily based on the principle of nourishing and preserving Yin and the blood while warming up Yang and replenishing Qi. The treatment of constipation should first identify whether it originated from deficiency or excess in order to re-establish equilibrium by targeting both the symptoms and the underlying condition of the problem. Also, it was worth mentioning that the treatment protocols were not consistent in the choice of stimulator, frequency and intensity of compression, or duration of the therapy among the included studies. Most studies did not describe who the clinician applying the intervention was. A few studies listed nurses, trainees, or patients, but none monitored compliance with auricular acupressure. These factors could have resulted in patients receiving different dosage of the acupressure, hence leading to varied degrees of treatment effectiveness. In addition to differences in intervention protocols, treatment effects were complicated by confounding variables such as diet, exercise, and medications. This issue was not addressed thoroughly by the researchers either.
The current diagnostic methods of constipation included clinical presentation and evaluation, endoscopy, anorectal manometry, balloon expulsion testing, barium enema, defecography and magnetic resonance defecography and Colonic Transit Time (CTT) [31]. However, studies in this review used subjective, non-standardized outcome evaluation metrics. We would like to see objective indicators such as CTT adding to the research. Finally, most studies had focused on the short-term efficacy of auricular acupressure for relief of constipation and lacked follow-up evaluation of long-term result. Only one study had a two-week post-intervention follow-up with a small sample size over a short period of time. Better designed trials may produce more creditable results related to the long-term effects of the therapy.
Underlying mechanism
The Yellow Emperor's Classic of Internal Medicine stipulates that "the ear is the place where the meridians are gathered” [32]. All twelve meridians of the human body are directly or indirectly connected to the ear. Stimulating the ear points can trigger the corresponding meridian sensory transmission and regulate the function of the internal organs to bring them into balance for the purpose of treating diseases. According to the Law of Biological Holography [33], the ear is the epitome of the human body, and the auricular acupuncture points are the areas where the epidermis of the ear communicates with the internal organs and meridians of the body. There are reflection points corresponding to the stomach, small intestine, large intestine, rectum, anus, and other internal organs. The auricular nerve is rich in innervations sources, which have been hypothesized by many scholars as having a mechanism of action closely related to the nerve conduction in the auricle [34]. By stimulating the ear acupuncture points, the sympathetic and parasympathetic activities of the body would be continuously regulated. This in turn would improve the activity of the gastrointestinal tract [35].
Implications for practice
Although the application of auricular acupuncture for treating constipation has been recognized in China, auricular acupressure is not recommended in international medical guidelines [39,40]. More studies are needed to validate its effectiveness and safety before it can be promoted as an ancillary therapy in clinical practice.
Limitations
The included literature presents some major limitations. First, their methodological quality is not high due to lack of clarity in blinding or allocation concealment. This may be due to the difficulty in making patients or caregivers oblivious to the auricular acupressure application. In addition, the diagnostic criteria for post-stroke constipation, the implementation of interventions, and the methods and timing of outcome assessment indicators varied among the included studies resulting in clinical heterogeneity. In the future, a standardized treatment protocol should be summarized in an evidence-based approach. Finally, all of the studies were conducted in China. Because of the cultural and geographical differences, the applicability of auricular acupressure for post-stroke constipation in other ethnic populations still needs to be further explored.
Conclusion
In summary, this review suggested that auricular acupressure was effective and safe in the treatment of post-stroke constipation. However, these results should still be interpreted with caution and can only provide some references for clinical practice at this time. We expect to see more rigorous randomized controlled trials to validate this TCM technique as an alternative or supplementary treatment method in the acute care and community settings.
References
- GBD 2015 Neurological Disorders Collaborator Group (2017) Global, regional, and national burden of neurological disorders during 1990-2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet Neurol 16: 877-897.
- Katan M, Luft A (2018) Global Burden of Stroke. Semin Neurol 38: 208-211.
- Camara-Lemarroy CR, Ibarra-Yruegas BE, Gongora-Rivera F (2014) Gastrointestinal complications after ischemic stroke. J Neurol Sci 346: 20-25.
- Li J, Yuan M, Liu Y, Zhao Y, Wang J, et al. (2017) Incidence of constipation in stroke patients: A systematic review and meta-analysis. Medicine (Baltimore) 96: 7225.
- Ingeman A, Andersen G, Hundborg HH, Svendsen ML, Johnsen SP (2011) In-hospital medical complications, length of stay, and mortality among stroke unit patients. Stroke 42: 3214-3218.
- Zhang T, Wang G, Li B, Wang L, Guo J, et al. (2018) Effect of acupuncture for constipation after ischemic stroke: study protocol for a randomized controlled trial. Trials 19: 454.
- Roque MV, Bouras EP (2015) Epidemiology and management of chronic constipation in elderly patients. Clin Interv Aging 10: 919-930.
- Shin JE, Park KS, Nam K (2019) Chronic Functional Constipation. Korean J Gastroenterol 73: 92-98.
- Li Y, Qi D, Gong L, Qu H, Xu B, et al. (2017) Effect of auricular points treatment combined with acupoints application in patients with constipation after lung cancer surgery. J Cancer Res Ther 13: 844-848.
- Jing X, Liu J, Wang C, Ji M, Chen X, et al. (2018) Auricular acupressure is an alternative in treating constipation in leukemia patients undergoing chemotherapy: A systematic review and meta-analysis. Complement Ther Clin Pract 31: 282-289.
- Chen PY (2012) Fundamentals of Chinese Medicine Nursing [in Chinese]. People's Health Press, Beijing, China.
- Cumpston M, Li T, Page MJ, Chandler J, Welch VA, et al. (2019) Updated guidance for trusted systematic reviews: a new edition of the Cochrane handbook for systematic reviews of interventions. Cochrane Database Syst Rev 10: ED000142.
- PRISMA (n.d.) (2017) PRISMA transparent reporting of systematic reviews and meta-analyses.
- Guo J (2019) Analysis of the effect of nursing intervention of auricular acupressure of beans on stroke patients with constipation [in Chinese]. Pharmaceutical industry 18: 0053-0053.
- Qian AP (2012) 42 cases of subarachnoid hemorrhage with constipation treated with auricular acupressure beans [in Chinese]. Chinese Journal of Traditional Medical Science and Technology 19: 469-470.
- Yin H, Qin LH (2012) Efficacy of auricular acupressure in the treatment of constipation in patients with qi deficiency and blood stasis type of stroke [in Chinese]. Clinical Journal of Traditional Chinese Medicine 24: 504-505.
- Ji J, Ren SL, Wang YW (2015) Efficacy of auricular acupressure in the treatment of actual constipation in the acute phase of stroke [in Chinese].Beijing Journal of Traditional Chinese Medicine 34: 661-663.
- Lv LM (2012) Clinical research of magnetic bead acupressure auricular point on patients with constipation after stroke [in Chinese]. Fujian University of Chinese Medicine.
- Wang Q (2015) Effectiveness of auricular seed burial on the care of constipation in patients with cerebral infarction [in Chinese]. Nei Mongol Journal of Traditional Chinese Medicine 5: 175-176.
- Zhang CY, Yao XQ (2017) Efficacy of auricular acupoint embedding as an adjunctive treatment for constipation in elderly stroke patients [in Chinese]. Smart Healthcare 3: 57-59.
- Yu CX, Jin LH, Chen XF (2014) Efficacy of ear acupressing beans in the treatment of constipation in patients with traumatic subarachnoid hemorrhage. Nursing and Rehabilitation Journal 13: 164-166.
- Cai BC, Zhang CY (2015) Efficacy of ear acupuncture bean burial to improve constipation symptoms in stroke patients. Chinese Medicine Modern Distance Education of China 13: 87-88.
- Xu HM, Liu CX, Wang CX (2013) Efficacy of auricular acupressure beans in 40 cases of constipation in stroke. Clinical Journal of Traditional Chinese Medicine 25: 1003-1004.
- Ministry of Health of the People's Republic of China (1994) Guiding Principles for Clinical Research of New Chinese Medicines. People's Health Press, Beijing,
- State Administration of Traditional Chinese Medicine. (1994) Diagnostic Efficacy Criteria for Chinese Medical Evidence. Nanjing University Press, Nanjing,
- Huang P, Liao HM (2014) Clinical effects of auricular application and comprehensive nursing intervention in stroke patients with constipation. World Chinese Journal of Digestology 22: 2800-2803.
- Hai HP, Wu GR, Wang SQ (2014) Effects of auricular plaster therapy to prevent constipation after stroke. Chinese Clinical Nursing 6: 108-110.
- Winge K, Rasmussen D, Werdelin LM (2003) Constipation in neurological diseases. J Neurol Neurosurg Psychiatry 74: 13-19.
- Chen X, Guan DL, Yang LX, Cao ZB (2021) The effect of evidence-based meal administration and auricular acupressure on patients in recovering from stroke. Journal of Qilu Nursing 27: 78-80.
- Zhang B (2015) Clinical observation on the treatment of constipation after stroke by ear acupuncture point embedding beans. Master dissertation. Anhui University of Traditional Chinese Medicine, China.
- Forootan M, Bagheri N, Darvishi M (2018) Chronic constipation: A review of literature. Medicine (Baltimore) 97: 10631.
- Chen YF, Zhan XL, Chen XH (2021) Clinical care observation of auricular acupuncture bean burial to improve Qi deficiency and constipation in the elderly. Fujian Journal of Traditional Chinese Medicine 43: 62.
- Wen XT (2012) Biological holography as a counter-evidence to the Tibetan theory of Chinese medicine. Journal of Basic Chinese Medicine 18: 1145-1146.
- Ma L (2014) Clinical efficacy and nursing experience of auricular acupressure of Vaccaria seeds in the treatment of constipation caused by antipsychotic drugs. Journal of New Chinese Medicine 2014: 190-192.
- Lu SF, Clinical efficacy of body acupuncture with auricular acupressure in the treatment of post-stroke deficiency evidence of constipation (2010) Master dissertation. Liaoning University of Traditional Chinese Medicine,
- Bosshard W, Dreher R, Schnegg JF, Büla CJ (2004) The treatment of chronic constipation in elderly people: an update. Drugs Aging 21: 911-930.
- Wang L, Shang SM (2016) Overview of auricular acupressure to prevent constipation in recent years. Journal of Basic Chinese Medicine 22: 1007-1010.
- Dennison C, Prasad M, Lloyd A, Bhattacharyya SK, Dhawan R, et al. (2005) The health-related quality of life and economic burden of constipation. Pharmacoeconomics 23: 461-476.
- Paquette IM, Varma M, Ternent C, Meaux GM, Rafferty JF, et al. (2016) The American Society of Colon and Rectal Surgeons' Clinical Practice Guideline for the Evaluation and Management of Constipation. Dis Colon Rectum 59: 479-492.
- Mearin F, Ciriza C, Mínguez M, Rey E, Mascort JJ, et al. (2016) Clinical Practice Guideline: Irritable bowel syndrome with constipation and functional constipation in the adult. Rev EspEnferm Dig 108: 332-363.
Citation: Li Y, Chen L, Su IJ (2021) Effectiveness of Auricular Acupressure for Post-Stroke Constipation: A Systematic Review and Meta-Analysis. J Altern Complement Integr Med 7: 213.
Copyright: © 2021 Yi Li, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.