Endovascular Repair of Radiation-induced Bilateral Common Carotid Artery Stenosis and Pseudoaneurysm with Covered and Uncovered Stent Graft using Double Embolic Protection Device
*Corresponding Author(s):
Javier Rodriguez-PadillaDepartment Of Vascular Surgery And Angiology, Hospital Universitario Severo Ochoa, Avenida Orellana S/n, 28912, Madrid, Spain
Email:javierrodriguezpadilla@gmail.com
Abstract
Purpose: We present an unpublished case of bilateral carotid injury due to radiation-induced treated by endovascular therapy using double embolic protection device as a novel technique.
Methods: Extracranial carotid artery pseudoaneurysm is a rare condition among head and neck cancer patients treated with radio therapy. We report a case of pseudoaneurysm in the right Common Carotid Artery (CCA) and critical stenosis in the left CCA.
A 72 years-old patient laryngeal cancer treated with laryngectomy and radiotherapy 26 years before admission. He presented to us complaining of right neck pain and right hemispheric TIA symptoms.
Results: Performed ultrasonography and magnetic resonance angiography revealed right Common Carotid Artery (CCA) pseudoaneurysm (size:13x25 mm) and critical stenosis in the left CCA.
Endovascular treatment was performed in bilateral carotid artery using covered stent in pseudoaneurysms in the right CCA and uncovered stent due critical stenosis in the left CCA using double embolic protection device. Both procedures showed successful exclusion of the pseudoaneurysm and widely patent artery.
Conclusion: Endovascular treatment in injury artery radiation-induced is safe and effective approach with low rate complications. The combined use of proximal cerebral protection devices and distal filter protection could decrease the rate of cerebral embolization procedure related.
Keywords
Carotid artery disease; Carotid artery pseudoaneurysms; Covered stent; Embolic protection devices; Radiation-induced carotid artery disease
Introduction
Extracranial carotid artery pseudoaneurysm is a rare condition among head and neck cancer patients treated with radiotherapy. Their formation and progression to carotid burst syndrome are the most feared complications with a small but significant rate of 4% [1,2].
Management of this complication is challenging. This is further complicated when the involvement is bilateral, the stenosis can compromise the cerebral vascular flow and predispose the patient to multiple ischemic attacks and the pseudoaneurysm that can cause the rupture, causing massive bleeding associated with high morbi-mortality.
We report a case of pseudoaneurysm in the right Common Carotid Artery (CCA) and critical stenosis in the left CCA after 26 years after neck radiotherapy that were successfully treated by bilateral stenting.
Case Report And Technical Note
A 72 years-old male patient with a history of ex-smoker, hypertension, hypercholesterolemic and laryngeal cancer treated with permanent laryngectomy and radiotherapy 26 years before admission. He presented to us complaining of right neck pain and right hemispheric TIA symptoms.
Performed ultrasonography and magnetic resonance angiography revealed right Common Carotid Artery (CCA) pseudoaneurysm (size: 13x25 mm) and critical stenosis in the left CCA. After obtaining informed consent, endovascular treatment was performed.
Throughout this procedure, the patient received a total of 5.000 units of heparin intravenously to ensure adequate anticoagulation.
Percutaneous arterial access was achieved from right common femoral artery and a 90 cm, 8 Fr sheath was placed. An 8 Fr sheath was advanced to the descending thoracic aorta over a 0.035 super stiff angled glide wire. A 6 Fr vertebral catheter was advanced through the sheath over wire into the right External Carotid Artery (ECA). The wire was removed and exchanged for a 0.035, 260 cm stiff Amplatz wire and 8 Fr sheath was advanced into the right CCA. The stiff Amplatz was exchanged for a 0.018, 300 cm. A 5 cm long Viabahn stent graft (WL Gore and Associates) was placed with the distal end just proximal to the ECA origin and extended proximally. Post-dilation was then performed using an 8x40mm diameter. Diagnostic angiography showed successful exclusion of the pseudoaneurysms and a widely patent ECA and ICA (Figure 1). There were no neurological or other complications.
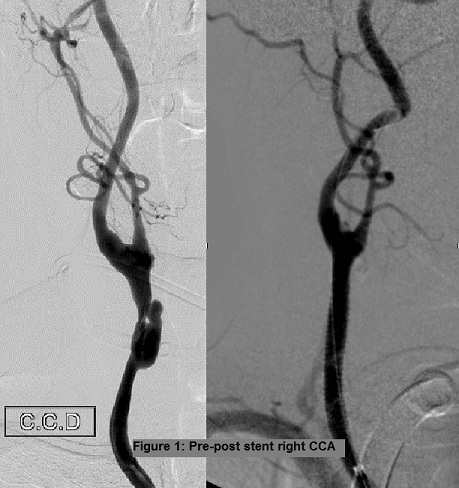 Figure 1: Pre-post stent right CCA.
Figure 1: Pre-post stent right CCA.
At 2 month we decided to proceed with stenting of the contralateral lesion. A 9F sheath was then positioned within the right common femoral artery. Using a 7F Simmons-3 catheter in combination with a 10F guide catheter, successful catheterization of the left CCA was achieved. We used proximal cerebral protection (Mo.Ma Medtronic™) and distal filter protection. Acculink carotid stent system 5x70mm (Abbot ™) was deployed into the patient’s left CCA. There was immediate improvement of the caliber of the artery (Figure 2).
 Figure 2: Pre-post stent left CCA.
Figure 2: Pre-post stent left CCA.
He was placed on antiplatelet therapy, Clopidogrel 75 mg daily for 3 month and long-term aspirin therapy (100 mg daily). Follow-up duplex scan at 6 months and 1 year showed that there was no flow in the pseudoaneurym in the right CCA and good patency in the left CCA.
Discussion
The consequences of carotid artery injury radiation-induced have not been as clearly defined. These mechanisms of is not fully understood, but may result from obliteration of the vasa vasorum, premature atherosclerosis, and weakening and necrosis of the arterial wall [2]. In a retrospective study performed by Carmody et al, it was concluded that high-dose radiotherapy to the head and neck region may be a significant risk factor for accelerated carotid atherosclerotic disease [3]. Classically it was classified radiation-induced carotid vasculopathy into three categories: acute carotid artery rupture, acute vessel occlusion within several months as a probable direct arterial injury, and late development of atheromatous and occlusive carotid disease [4].
The standard treatment for pseudoaneurysm has been open surgical therapy [1]. More recently, endovascular techniques using stents have offered a less invasive approach.
Three main endovascular techniques for carotid pseudoaneurysm repair have been reported; endoluminal stent placement across the neck of the pseudoaneurysm with subsequent coiling [5-6], percutaneous injection of thrombin and use covered stent. Holder, et al. treated carotid artery pseudoaneurysm by percutaneous injection of human thrombin into the sac [7]. Such a technique requires a long neck connecting the artery to the sac; a short neck increases the risk of complication due to thrombin leaking into the systemic.
In the present case, the patient had bilateral lesions. On the right side, neurologically symptomatic pseudoneurysm. We performed to endovascular treatment with a covered stent.
Pseudoaneurysm exclusion with use of covered stents is as in an open surgical repair; this enables total exclusion of the pseudoaneurysm, but with potentially much less morbidity and minimize the risk of distal embolization [8-9]. We decided to use Viabahn stent graft due longitudinal flexibility and shape memory make this graft more resistant to deformation by mechanical forces. The absence of atheromatous plaques and stenotic lesion, we thought that the risk of cerebral embolism during the procedure was less if we did not use embolic protection devices.
On the left side he presented critical stenosis radiation-induced, neurologically asymptomatic. We performed endovascular treatment using an uncovered stent with a double embolic protection device: Mo.MA (Proximal Protection Device) and a distal filter protection. Moteki, et al. suggested a more reliable embolic protection can be achieved with the combined use of Mo.Ma and distal filter protection device. The advantages of the combined use of filter devices are the simplicity of the procedure and the ease of dealing with ischemic intolerance [10].
Conclusion
Our case is interesting because of the bilateral carotid lesion involvement related to neck cancer treated by radiotherapy more than 20 years before the TIA symptoms. Endovascular treatment on hostile necks minimizes complications related to open surgery. Although there is no long-term evidence in the literature of these treatments, the use of covered stents for cases of carotid pseudoaneurysms is a safe and effective approach with a low rate complications. For stenotic lesions, the combined use of proximal cerebral protection devices (Mo.Ma) and distal filter protection could decrease the rate of cerebral embolization procedure related.
References
- Nadig S, Barnwell S, Wax MK (2008) Pseudoaneurysm of the external carotid artery-Review of literature. Head Neck 31: 136-139.
- Ellens DJ, Hurley MC, Surdel D, Shaibani A, Pelzer H, et al. (2010) Radiotherapy-induced common carotid pseudoaneurysm presenting with initially occult upper airway hemorrhage and successfully treated by endovascular stent graft. Am J Otolaryngol 21: 195-198.
- Okamura HO, Kamiyama R, Takiguchi Y, Kimizuka K, Ishikawa N, et al. (2002) Histopathological examination of ruptured carotid artery after irradiation. ORL J Otorhinolaryngol Relat Spec 64: 226-228.
- Carmody BJ, Arora S, Avena R, Curry KM, Simpkins J, et al. (1999) Accelerated carotid artery dis- ease after high-dose head and neck radiotherapy: Is there a role for routine carotid duplex surveillance? J Vasc Surg 30:1045-1051.
- Loftus CM, Biller J, Hart MN, Dion JE, Lumsden AB (1987) Management of radiation-induced accelerated carotid aterosclero- sis. Arch Neurol 44: 711-714.
- Bush RL, Lin PH, Dodson TF, Dion JE, Lumsden AB (2001) Endoluminal stent placement and coil embolization for the management of carotid artery pseudoaneurysms. J Endovasc Ther 8: 53-61.
- Holder R, Hilton D, Martin J, Harris PL, Rowlands PC, et al. (2002) Percutaneous thrombin injection of carotid artery pseudoaneurysm. J Endovasc Ther 9: 25-28.
- Scavee V, De Wispelaere JF, Mormont E, Coulier B, Trigaux JP, et al. (2001) Pseudoaneurysm of the internal carotid artery: treatment with a covered stent. Cardiovasc Interv Radiol 24: 283-285.
- Gupta K, Dougherty K, Hermman H, Krajcer Z (2004) Endovascular Repair of a Giant Carotid Pseudoaneurysm With the Use of Viabahn Stent Graft. Catheter Cardiovasc Interv 62: 64-68
- Moteki Y, Niimi Y, Sato S, Inoue T, Shima S, et al. (2016) Effectiveness of the Combined Use of Distal Filter Protection Device and Mo.Ma Ultra: Technical Note. J Stroke Cerebrovasc Dis 25: 2627-2631.
Citation: Rodriguez-Padilla J, Carrascosa T (2021) Endovascular Repair of Radiation-induced Bilateral Common Carotid Artery Stenosis and Pseudoaneurysm with Covered and Uncovered Stent Graft using Double Embolic Protection Device. J Angiol Vasc Surg 6: 062.
Copyright: © 2021 Javier Rodriguez-Padilla, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.