Epidemiology of Hepatitis B, C and HIV in Gastrointestinal Tract Patients of Muzaffarabad Azad Jammu and Kashmir, Pakistan
*Corresponding Author(s):
Waill ElkhateebChemistry Of Natural And Microbial Products Department, National Research Centre, Dokki, Giza, 12622, Egypt
Email:waillahmed@yahoo.com
Abstract
Hepatitis B and hepatitis C are basis of high death rates, particularly in people infected with HIV disease. Hepatitis B and C are related in conveyance by the sexual contact, erect from mother to unborn young and by injections within veins. Main conveyance of hepatitis C is route of a blood communication. Weakened immune system cause dangerous influences of hepatitis C virus. Study was conducted for consideration resources of HBV, HCV and HIV in general inhabitants of Muzaffarabad, Azad Jammu and Kashmir-Pakistan. Hepatitis B, hepatitis C and HIV are tested by ELISA and ICT were consumed. Immunogen was noticed for hepatitis B and for hepatitis C, HCV, HIV protective immune proteins were noticed. PCR for HBV-DNA and RT-PCR for HCV-RNA also finalized. Almost 500 patients registered in this analysis from which 33% caught positive for HBV, all were male and no female was positive after final acceptance by PCR. 66% HCV positive persons were found, 5.5% were male and 94.5% were female. No HIV positive person was found by technique of PCR. 20-30 age group was most dominant in HBV, HCV HIV. Conclusion: Genetic constitution 1a is more dominant in HCV comparable to genetic constitution of 2b in HBV.
Keywords
Gastrointestinal Tract; HBV; HCV; Hepatitis B; Hepatitis C; HIV; Kashmir; Muzaffarabad Azad Jammu; Pakistan; Prevalence
Introduction
Ultimate source of ruin of entire world is hepatitis. Five subdivisions of hepatitis viruses that influence liver cells in irregular way (HAV, HBV, HCV, HDV and HEV) basis of chronic disease of liver cells and result in Liver Cancer [1]. Liver is influenced by existence of exciting cells, and organs. Earlier hepatic stages of hepatitis have no indication. Slowly it can goes to pale-yellow colour of dermis, eyes, urine along loss of appetite and malaise. Hepatitis changed into recurrent stage, after 6 months. It is guesstimated that entire world is influenced by set of viral diseases. It may because of harms of hepatitis, more alcohol and drugs consumption are source of hepatitis. Connection with impure blood and fluids spread Hepatitis E. Saliva, fluid semen, and vaginal fluids of the sufferer, particularly HBV. Main source of HCV is impure blood. HBV and HCV has no indication at beginning [2].
B virus is source of hepatitis B that is long-lasting exciting disease cause damage of liver cells. 3200 nitrogen bases are present in genome of small, circular HBV virus. Genetic form of this virus arranged from (A-E). HBsAg present on surface of virus and fix upon presence of virus. Severe liver diseases stimulated by hepatitis B. About 240 million people influenced by it and it give rise to ruin of about 600,000 people. Homogeneity between diseases with hepatitis B and HIV diseases proved by investigation, cases grow worse at a calculated rate confront to other infected with hepatitis B without HIV. Infection rates increased by many factors involving lack of vaccination of children or anomaly in it, erect conveyance from mother to unborn young, infected blood transfusion poor immunization and medical staff [3].
Inhabitants of Pakistan are suffered by rapid transmission of hepatitis B infection because of unsatisfactory standard of living and subsided health conditions. 67.5% inhabitants live in backwoods area and vulnerable to low business and social status system. There is no indication of hepatitis at start, but indications start to appear with improvement and form jaundice in eyes, skin and pain in lower abdomen [4].
Sexual contacts, injections of drugs blood transfusion and injections disperse widely hepatitis C. Hepatitis C influence 200 million people in entire world and ruin 350,000 cases each year. Moreover, HIV influences 36.9 million people 53.1% live in Africa particularly in desert space. Every year, 240 million people are upset by HBV and HCV a reality. Long lasting infection are result of hepatitis viruses, causing impurity of liver, liver failure and cancer of liver cells. Long lasting liver diseases occur if hepatitis diseases occur for less than six months and liver functions wind-up. Massive consumption of drugs like ATT, cephalosporin's anticonvulsant, steroids is source of hepatitis [5].
Primary logic for transmission of hepatitis B and C infection are injections because people used previously used injections due to poor health condition in Pakistan. In Pakistan each year 1.5 million units of blood are transmitted. Viral infections transfuse by spread of drug addiction by injections. Fluctuation between HBV and HCV in HIV-infected patients consisted on variance in socio demographic surroundings and approach to immunization.
Objectives of the Study
The objectives of the study are:
- Analyzing and estimating dominance of hepatitis B, hepatitis C and AIDS in customary people having gastro intestinal track disorders.
- Get source dominance of HBV, HCV and AIDS in customary people.
- Check out hazardous thing in people positive for any virus.
- Boost up awareness among the general people of Muzaffarabad.
Materials and Methods
People having GIT disorders are targeted in Muzaffarabad because mostly suffer types of surgery, fluid transmission etc. These were significant jeopardy events in the transfusion of hepatitis B, hepatitis C and HIV. People having low healthful conditions and socioeconomic are major reason for spreading destructive diseases. People having severe problems of GIT are tested mostly to find out spread of destructive diseases.
Inclusion and Exclusion Criteria
In this analysis people having GIT disorders are included.
Sample Size and Blood Sampling
Common techniques and sterilized syringes are used for vein puncture to take sample of patients. Centrifugation of blood give serum at 3000-4000 rpm.
Screening of HBV Antigen, HCV, and HIV Antibodies
Blood is collected by immuno-chromatography technique. 5ml blood is taken from patients. . Blood was placed into tubes after collection. Tubes are retaining in room temperature. Maximal for 10 minutes. For five minutes samples are rotated at 3,000-4,000rpm. After this gel tubes were used. At room temperature serum is stored in gel tubes. . HBV antigen and HCV antibody encountered by serum. Screening ICT kits are used for earlier screening of anti-HBsAg, anti-HCV. Antigen and antibody hybridization determine ICT methodology. ICT kit having C and T band filled with serum. 3 drops of buffer are added in serum in. If band present at C side, shows people having HBsAg and anti-HCV antibody. It shows if both bands appear on C as well on T side, patient is infected [6].
Enzyme-Linked Immunosorbent Assay (ELISA)
The method given by Oi et at., (2009), is required to be done is ELISA. Buffer solution used to dilute the 100 microliter antibody and placed in well and incubated at 4C for night and covered with plate. Buffer solution B were washes out wells. Empty plates are inverted in a sink at beginning. In each well, ten microliters of test sample were put in buffer B and incubated for two hours at room temperature before being deposited onto the plate. In the buffer solution, 100 microliters of conjugated antibody and enzyme complex were added. The plate was incubated at room temperature for one hour. Each well received 100 microliters of chromogenic substrate C, and the plate was kept dark. To stop reaction 100 microliter of 0.5M H2S04 were added. By using ELISA automated photometer result were read 490nm out from bottom microwell. Standard curve was plotted at 490nm by using logarithm paper [7].
Polymerase Chain Reaction (PCR)
To confirm HBsAg, HCV, HIV positive cases PCR is used after using ICT kit method and ELISA. Housekeeping primer stc1. H1R, stc1. H1R1 for confirmatory purpose [8].
HBV PCR Screened in Positive Individuals
DNA isolation for HBV: from the serum of HBsAg positive individual viral DNA was isolated and incubated for 5 minutes at room temperature. 200 microliter of isopropanol and 250 microliter of serum was added. Then for 5 minutes mixture rotated at 7000rpm and leaves a clear liquid. In 5 minutes at 7000rpm mixture is centrifuged 70 percent ethanol and dried in open place [9]. Amplification of DNA was carried out to study the HBV surface gene through PCR. To detect the quantity of virus amplification is done in two rounds. Uses reagents are shown .Sct1.H1R primer is used for that purpose, with following sequence:
Forward Primer: 5-GATCCTGCCTCATCT-3 Tm 60°C
Reverse: 5-TGAAGAATGGCACG-3 Bp; 180
|
Agents |
first round |
2nd round |
|
|
Volume |
Volume |
|
Buffer |
2.4 |
2.4 |
|
Free water Nuclease |
3.3 |
9.6 |
|
Magnesium chloride |
1.5 |
1.5 |
|
2.5 ml dNTPs |
1.3 |
1.3 |
|
Polymerases |
0.2 |
0.2 |
|
Template of DNA |
10.2 |
4.4 |
|
Primer Reverse (11pmole per µL) |
1.2 |
1.2 |
|
Primer Forward (11 pmole per µL) |
1.2 |
1.2 |
|
Final volume |
20.1 |
20.1 |
For denaturation, the PCR was run at 93°C for 6 minutes, followed by 33 cycles at 93°C in each 33s. Annealing at 53°C for 40s done and for 33s at 70°C final extension for 4 min.
Screening of HCV with PCR
RNA Isolation: in the Gel tube serum is placed and 600 µL isopropranolol added. It was mixed gently. For 15 minutes and 11,800rpm centrifugation is done replaced the clear solution carefully. Pellet was washed and dried in air by using ethanol and to dissolve the solution 50 µL of sterilized water was added [10].
HCV Genotyping: Using different reverse primers genotyping of positive sample design from HCV genome present.
Reverse-primer: AT (AG) TACCCCATGAG (AG) TCGGC- 3’
|
Agents |
Volume |
|
Primer –Reverse |
1.2 |
|
Buffer |
4.4 |
|
dNTPs |
1.0 |
|
RNA |
10.3 |
|
DEPEC |
2.5 |
|
Transcriptase- Reverse |
1.2 |
|
Inhibitors |
0.2 |
|
Total- volume |
20.1 |
At 37°C for 50 min and 72°C 6min thermocycler of reverse transcriptase was set. To activate the DNA PCR, basic PCR was utilized in the first round, and multiplex PCR was employed in the second round using two sets of primers. For its round and 2nd-round primer sets are as follows;
For its round of PCR amplification, reaction mixture:
Forward- Primer: 5’ -GGGAGGCACCATG- 3’
Reverse -Primer: AT (AG) TACCCCATGAG (AG) TCGGC-3’
Round second.
|
Mixture I |
Mixture II |
|
G2a 5’-CGCTCC-3’ |
G1a 5’-GCATAGGACCT -3’ |
|
G2b 5’-GCGAGAC-3’ |
G3a 5’-GTCCCTTCGCT -3’ |
|
G3b 5’-CTTACGTAC-3’ |
G4a 5’-CAACGTCCAT -3’ |
|
|
G5a 5’-GAGGAGAGCAA-3’ |
|
|
G6a 5’-GGTCCAATGT-3’ |
HIV Screening with ICT KIT Method
By using 5cc sterilized syringe 2ml blood was taken at beginning and 2-3 drops added in ICT kit. 2 or 3 drops of buffer are added in ICT device. Sample is placed in room temperature for five min. In kit, sample run to make 2 bands on T side. HIV is positive in that person if two bands are shows in ICT kit
Statistical Analysis
Using SPSS version 21 statistical program results were analyzed. Calculation of number and proportion of variable is done.
Results
The entire population of the study was 500 people, with 233 men (47.3%) and 269 women (54.6%). The ICT kit was used to test all patients for anti-HCV and anti-HIV antigens and antibodies at the start. 66 ICT-positive patients were tested for matching antibodies and antigens using quantitative ELISA. PCR was used to establish the presence of associated antibodies and antigens in all 34 ELISA-positive patients. PCR has completed 28 (91%) of the 34 cases.
Hepatitis B, Hepatitis C, and Hiv Prevalence using ICT Kit
Only GIT patients were counted in Muzaffarabad, with a total of 500 people (232 men and 268 women). All patients were tested for HBsAg, anti-HCV, anti-HIV antigens, and associated antibodies using the ICT technique. There were 21 (32.3%) HBsAg ICT positive participants out of 65, with males accounting for 18 (85.7%) and females accounting for 3 (14.3%). There were 42 (64.6%) males and 35 (83.4%) females among the 65 anti-HCV antibody ICT positive people. Positive people for anti-HIV antibody were detected in 2 (3.1%) of the 65 anti-HIV antibody ICTs, all of whom were females. No males were reported positive for anti-HIV antibody following the ICT Method.
|
Overall Population |
Overall Positive Individuals (=500) |
||||||
|
501 |
65 (13%) |
||||||
|
HBsAg |
Anti-HCV |
Anti-HIV |
|||||
|
21 (32.4%) |
42 (64.7%) |
2 (4.2%) |
|||||
|
Male |
Female |
Male |
Female |
Male |
Female |
Male |
Female |
|
233 |
269 |
19 (86. %) |
4 (15.3%) |
8 (17.6%) |
36 (85.4%) |
---- |
2 (99%) |
ELISA
Using quantitative ELISA 66 ICT positive people were more verified for antibodies and antigens. From 33 Anti HCV antibodies ICT, by ELISA 22(66.6%) are positive in male 21(95.5%) and only 01(4.5%) Through quantitative ELISA 66 ICT positive people are more verified for antibodies as well antigens. From 34 positive individuals were 02(4.1%) consist of women 02(99%) positive anti HIV antibody.
|
Overall Population |
Overall Positive (n=66) |
||||||
|
501 |
34 (51%) |
||||||
|
HBsAg |
Anti-HCV |
Anti-HIV |
|||||
|
11 (31.3%) |
23 (67.6%) |
02 (4.1%) |
|||||
|
Male |
Female |
Male |
Female |
Male |
Female |
Male |
Female |
|
232 |
268 |
_ |
10 (100%) |
21(95.5%) |
01 (4.5%) |
-- |
01 (100%) |
Polymerase Chain Reaction (PCR)
Table 6 shows the results of PCR testing on 33 ELISA positive people for associated antibodies and antigens. By PCR, 27(81%) were more verified out of 33. By PCR, HBsAg ELISA positive individuals were confirmed consist of only male 9(100%) no female was positive. ELISA confirmed positive individuals 19(67.7%) from 27 anti-HCV antibodies. After PCR, 19 positive 1(6.5%) man and women 18(95.5%) was positive. ELISA positive individual was not verified 0(0%) from 27 anti-HIV antibodies. After PCR, males and females were not positive for anti-HIV antibodies.
|
Overall Population |
Overall Positive Individuals (n=34) |
||||||
|
501 |
28 (82%) |
||||||
|
HBV |
HCV |
HIV |
|||||
|
08 (34.3%) |
19 (67.7%) |
_ |
|||||
|
Male |
Female |
Male |
Female |
Male |
Female |
Male |
Female |
|
233 |
269 |
08 (99%) |
_--- |
02 (6.5%) |
18 (95.5%) |
_-- |
--_ |
Amplification of STC1.H1R gene for HBV
PCR amplification was performed at a particular annealing after primer optimization at temperature 60oC. On 2% agarose gel amplified PCR was placed containing ethidium bromide. Size of specific gene product (180bp) was estimated by invitrogen ladder of 100 base pair (bp). Amplification Stc1. HIR was shown by bands (Figure 1) 100 bps
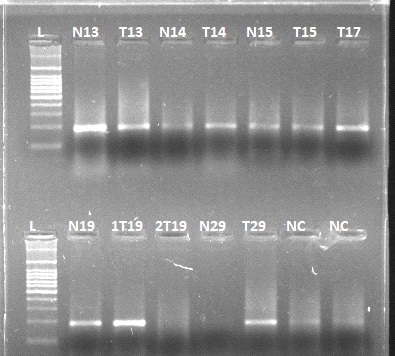 Figure 1: Amplification of STC1.H1R gene for HBV
Figure 1: Amplification of STC1.H1R gene for HBV
Amplification of STC1.H1R1 gene for HCV
PCR amplification was performed at a specific annealing after primer optimization at temperature 65o C for the HCV gene. On 3% agarose gel amplified PCR was placed containing ethidium bromide. Size of the specific gene product, which is 190 base pair, was estimated by Invitrogen ladder of 100 base pair (bp) amplification of Stc1 H1R1 shown by bands (Figure 2).
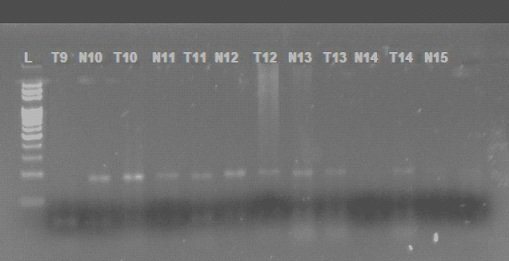 Figure 2. Amplification of STC1.H1R1 gene for HCV
Figure 2. Amplification of STC1.H1R1 gene for HCV
Age Groups
Population size was 500 begins from 10 to above 40. From 65 starting positive screened patients age groups are 10-20, 20-30,30-40 and above 40. 28 were positive for HBV, HCV and by performing PCR 0 positive case was shown for HIV. 9(18%) HBV positive and 19 individuals consist of 1 man and 18 women from 27 individuals and 19(4.6%) were positive HCV and no HIV individual were positive by PCR. In age groups of 20-30, 30-40 and above 40 years HBV and HCV positive individuals were shown.
|
No. |
Age |
HBV occurrence |
HCV occurrence |
HIV occurrence |
|
001 |
20-30 |
01 |
01 |
0 |
|
002 |
30-40 |
07 |
09 |
0 |
|
003 |
40-45 |
02 |
06 |
0 |
|
004 |
Above 50 |
03 |
05 |
0 |
500 were total individuals in present analysis. In estimation 54 (11.6%) knew about hepatitis B and hepatitis C before awareness 448 (90.4%), not known after awareness 501 (99%). Hepatitis influences the hepatic function 06 (2.0%) known before-awareness and 496(98%) not known after-awareness 501(99%) found known. Jaundice is a prevalent sign of hepatitis B and C, and 16 (24.4 percent) have previously been aware of it. After-awareness 384 (77.6%) not known 479 (96.6%) were found to be known, while 23 (5.4%) were discovered to be unknown. Before-awareness transmission by unsterilized surgical tools, 383 (77.4%) knew about hepatitis B and hepatitis C. There were 119 (24.6%) people who had no idea who they were. After-awareness was discovered in 501 (99%) of the cases.
383 (77.4%) were known hepatitis may spread by contaminated body fluids before awareness 119(24.6%) not known after-awareness 501 (99%) found known. 186 (38%) hepatitis B and hepatitis C transmitted by using contaminated blades known before-awareness and 316 (64%) not known 501 (99%) found known after-awareness. 1(1%) hepatitis B and hepatitis C transmitted from mother to offspring before awareness known 367(74.2%) found known after-awareness and 135 (27.8%) were not known after- awareness.
|
No. |
Questions |
BEFORE-Awareness |
AFTER- Awareness |
||
|
YES |
no |
YES |
no |
||
|
001 |
Heard about Hepatitis B and C? |
54 (10.7%) |
448 (88.4%) |
501 (99%) |
(1%) |
|
002 |
Are Hepatitis B and Hepatitis C are viral diseases? |
06 (1.2%) |
496 (98%) |
501 (99%) |
1 (1%) |
|
003 |
Can Hepatitis affect Hepatic functions? |
06 (1.2%) |
496 (98%) |
501 (99%) |
1 (1%) |
|
004 |
Is jaundice one of the most prevalent symptoms of Hepatitis B or C? |
118 (24.4%) |
384 (77.6%) |
479 (96.6%) |
24 (5.4%) |
|
005 |
Are unsterilized syringes, needles, and surgical equipment capable of transmitting Hepatitis B or C? |
383 (77.4%) |
119 (24.6%) |
501 (99%) |
1 (1%) |
|
006 |
Is it possible to contract Hepatitis B or C from infected blood or blood products? |
383 (77.4%) |
119 (24.6%) |
501 (99%) |
1 (1%) |
|
007 |
Is it possible to contract Hepatitis B or C via barber's blades/ear and nose piercing? |
186 (38%) |
316 (64%) |
501 (99%) |
1 (1%) |
|
008 |
Is it possible for hepatitis B or C to be passed down from mother to child? |
1 (1%) |
600 (101%) |
367 (74.2%) |
135 (27.8%) |
|
009 |
Is a Hepatitis B vaccine available? |
06 (2.0%) |
496 (98%) |
403 (81.4%) |
99 (19.7%) |
Many risk factors influence spreading of hepatitis viruses, Treatment for a dental problem, Surgery, Personal belongings Sharing, Barber/Beauty Parlours visit, hospital-related history, and Piercing /Tattooing. Most influencing risk was Barber/Beauty Parlours visit Personal belongings Sharing (100%), then Piercing/Tattooing (60.6%), Treatment for dental problem (20.4%), Hospital related history (15.8%), , and Surgery (7%).
|
11
|
management for dental problem |
YES |
103 (21.4%) |
|
NO |
399 (80.6%) |
||
|
22 |
SURGERY |
YES |
36 (8.0%) |
|
NO |
466 (94%) |
||
|
33 |
PERSONAL SHARING |
YES |
600 (200%) |
|
NO |
1 (1%) |
||
|
44 |
Beauty Parlours visit |
YES |
600 (200%) |
|
NO |
1 (1%) |
||
|
55 |
HOSPITAL RELATED HISTORY |
YES |
80 (16.8%) |
|
NO |
422 (85.2%) |
||
|
66 |
Piercing/ Tattooing |
Yes |
303 (60.6%) |
|
No |
197 (39.4%) |
Discussion
General population of Muzaffarabad was marked for analysis having GIT disorders Muzaffarabad is the capital city of AJK packed with socio-economic background. 500 is overall volume marked individuals. Result shows high rates of infection with the B virus, particularly in men, which may because of them being more vulnerable to jeopardy factors.
Range of ages is from 10 to above 40 years. For starting screening of my marked population ICT method was used. Total volume of population was 600, 65 individuals marked positive. In the ICT technique, HBsAg 21 was found positive, 42 was found positive as anti-HCV antibody, and 2 was found positive as anti-HIV antibody in 66 persons. HBV and HIV infection was marked in 12 percent of sufferers, while HCV and HIV infection was marked in 14 percent of sufferers [11]. From 66 people who were first screened positive, more were confirmed as positive persons for (HBV, HCV, and HIV) in ELISA. From 27 (81 %) individuals were confirmed by PCR.
HBV, HCV, HIV and accumulative epidemiology in Muzaffarabad have gastrointestinal tract disorders. The prevalence of HBV varied between 33.3%, 30.3%, and 33.3%. HBV prevalence is high in evaluated occurrence rates of HBV in AJK, particularly, Lahore in 1998 is 5.06% [12], and Karachi in 2001 was 5.47%, in 2003 is 5.84% and in Pinddi in 2003 is 3.54% and Isl 2005 was 2.57% and 2.82% prevalence in Fuji foundation hospital Rawalpindi in 2006 and HCV was 7.56%. HIV prevalence ranges from 3.1% is high In contrast along the evaluation in 1970s mostly positive cases of HIV and AIDS were 0.6%. 3% blood donor was influenced along HIV at beginning [12].
Viral infection and age group has a relation, as it was shows that infection was more focalized in the age group of 20-30. In contrast, Researchers showed that HBV and HIV was more general in sufferers aged 36 to 46 years while HCV and HIV was dominant general in sufferers above 46 years. It shows that HCV and HIV was prominent in the man population with 30 to50 years. Transmission of hepatitis C and B virus is mainly due to use of injections in medical care setting particularly in developing countries. . It shows 500 (100%).It is in harmony of Khan study which manipulated study on 203 people. 0n visiting 96 people got injections. From 135 patients, 19% positive for anti BV antibody whose sera have anti-HCV antibodies [13].
People use 4-5 injections per year and influenced by hepatitis B in Punjab. In contrast to people who don’t take injections these are affected 11.9 times [14]. These viruses can also be transmitted by blood derivatives. When compared to professional blood donors, voluntary blood donors had a lower HBV prevalence. (p 0.001) (9 percent vs. 0.8 percent) [13]. Drugs also spread viruses 500,000 people use heroin in Pakistan consisted 5000 were regular and 150,000 are occasional. In IDUs in Lahore and Quetta, prevalence was 94% and 76%. Punjab and Baluchistan have prevalence rates of 94% and 76%, respectively [15]. Shaving tools mostly transfer this infection people exposed to same societal factors mostly infected with HBV. Hygienic tools inside house spread virus. Many vulnerable factors cause spread of this virus, and the chance of transfusion of virus is high compared to the transmission of hepatitis C and HIV [16].
Many vulnerable factors cause spread of hepatitis virus, Treatment for a dental problem, Surgery, Personal belongings Sharing, Barber/Beauty Parlours visit, hospital-related history, and Piercing/Tattooing. The most effective risk were Barber/Beauty Parlours visit Personal belongings Sharing (100%), then Piercing/ Tattooing (60.6%), Treatment for dental problems (20.4%), Hospital related history (15.8%), and Surgery (7%). These agree with Qureshi et al. (2009) decided that vulnerable factors for the transfusion of viruses were clearly identified in analysis [17-19].
Conclusion
This analysis threw a light on correlation between hepatitis B and C virus infection and HIV infection in Pakistan. In targeted analysis, hepatitis C was high preeminent. In young generation, HCV found positive in vulnerable condition. To stop transmission of this virulent disease it is appealed to upper hands to do something. Useful knowledge, diagnosis, treatment and vaccination of these virulent disorders should be given importance to alleviate this dangerous disease. Set up level of medical services, health awareness on methods of infection, boost up methods of vaccination help reduced upraised percentage of virus infection.
References
- Su T-H, Peng C-Y, Chang S-H, Tseng T-C, Liu C-J, et al. (2021) Serum PIVKA-II and alpha-fetoprotein at virological remission predicts hepatocellular carcinoma in chronic hepatitis B related cirrhosis. Journal of the Formosan Medical Association 121 :703-711.
- Alqahtani SA, Colombo M (2020) Viral hepatitis as a risk factor for the development of hepatocellular carcinoma. Hepatoma Research, 6:58.
- Rebeaud F, Bachmann M (2012) Virus-like particles as efficient delivery platform to induce a potent immune response Innovation in Vaccinology 87-122.
- Khalil AT, Ali M, Tanveer F, Ovais M, Idrees M, et al. (2017) Emerging viral infections in Pakistan: issues, concerns, and future prospects. Health security, 15: 268-281.
- Barros MM, Ronchini KR, Soares RL (2018) Hepatitis B and C in pregnant women attended by a prenatal program in an universitary hospital in Rio de Janeiro, Brazil: retrospective study of seroprevalence screening. Arquivos de gastroenterologia, 55: 267-273.
- Tyfoor LM (2016) Parasitological and Immuno-Molecular Diagnosis of Kala-Azar from Peripheral Blood Buffy Coat in El Gedaref State, Sudan (2013-2016). University of Gezira.
- Lequin RM (2005) Enzyme immunoassay (EIA)/enzyme-linked immunosorbent assay (ELISA). Clinical chemistry, 51: 2415-2418.
- Ito K, Shimizu N, Watanabe K, Saito T, Yoshioka Y, et al. (2013) Analysis of viral infection by multiplex polymerase chain reaction assays in patients with liver dysfunction. Internal Medicine, 52: 201-211.
- Li G, Li W, Guo F, Xu S, Zhao N, et al. (2010) A novel real-time PCR assay for determination of viral loads in person infected with hepatitis B virus. Journal of virological methods, 165: 9-14.
- Maragkoudaki X (2014) The Effect of Diet-induced Maternal Obesity on Offspring Energy Balance in a Murine Model and the Therapeutic Potential of a Maternal Dietary Intervention with a Fibre Supplement. King's College, London.
- Sharma V, Ramachandran VG, Mogha NS, Bharadwaj M (2018) Hepatitis B & C virus infection in HIV seropositive individuals & their association with risk factors: A hospital-based study. The Indian journal of medical research, 147: 588.
- Busch MP, Young MJ, Samson SM, Mosley JW, Ward JW, et al. (1991) Risk of human immunodeficiency virus (HIV) transmission by blood transfusions before the implementation of HIV?1 antibody screening. Transfusion, 31: 4-11.
- Simonsen L, Kane A, Lloyd J, Zaffran M, Kane M (1999) Unsafe injections in the developing world and transmission of bloodborne pathogens: a review. Bulletin of the World Health Organization, 77: 789-800.
- Khan H (1996) A study of seroprevalence of hepatitis B and C in mothers and children in Lahore. Pak Pediatr J, 20: 163-166.
- Khan MA, Ashraf M, Rehman A, Ali A, Ashraf M, et al. (2006) Prevalence of HBV, HCV and HIV in blood donors at Liaquetpur. The Professional Medical Journal, 13: 23-26.
- Pasha O, Luby SP, Khan AJ, Shah SA, McCormick JB, et al. (1999) Household members of hepatitis C virus-infected people in Hafizabad, Pakistan: infection by injections from health care providers. Epidemiology & Infection, 123: 515-518.
- Matters USD, Narcotics, US Affairs LE (2000) International Narcotics Control Strategy Report: The Bureau.
- Bauchner H, Fontanarosa PB, Livingston EH (2020) Conserving supply of personal protective equipment-a call for ideas. Jama, 323: 1911.
- DeLoach CD (2003) Understanding the phenomenology of racism: Willingness to access health care in African American women with HIV: Azusa Pacific University.
Citation: Irshad M, Akram M, Khan F, Elbossaty W, Saeed M, et al. (2022) Epidemiology of Hepatitis B, C and HIV in Gastrointestinal Tract Patients of Muzaffarabad Azad Jammu And Kashmir, Pakistan, J Adv Microbiol Res 5: 017.
Copyright: © 2022 Muhammad Irshad, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.