Evaluation of Public Awareness, Knowledge and Attitudes towards Basic Life Support among Non-Medical, Adult Population in Muscat City, Oman: Cross-Sectional Study
*Corresponding Author(s):
Aisha AldhakhriDirectorate Of Nursing Affair, Sultan Qaboos University Hospital, P.O. Box 38, P.C 123, Al-Khod, Muscat, Oman
Tel:+968 99191494,
Email:aisha3@squ.edu.om
Abstract
Background: Life-threatening illnesses or injuries may occur at places where there are no health service providers, so it is imperative that laypeople are equipped with all necessary knowledge and skills to provide BLS.
Purpose: This cross-sectional study investigated public awareness, knowledge and attitudes levels towards BLS among non-medical adult-Omanis in Muscat, Oman and explored the association between knowledge and attitude with socio-demographic characteristics.
Methods: 426 subjects were investigated between February and March 2020, using Adopted, validated, online questionnaire, including 37 items. Results were presented in tables with descriptions.
Findings: Knowledge level scored very low (Mean 3.5) whereas attitude levels cored very high (Mean 54.5).
Conclusion: The awareness was substantial. Knowledge level was very low but it differs with respect to socio-demographic characteristics. All participants had positive attitude toward BLS. Study findings advocating the need for mandatory training in BLS for all non-medics in Oman and incorporating BLS teaching in school curriculum.
Keywords
Attitude; Awareness; Basic Life Support; Cardiopulmonary resuscitation; Knowledge; Public
INTRODUCTION
Basic Life Support (BLS) is a level of medical care that is offered to victims of life-threatening illnesses or injuries until they can be given full medical care at a hospital [1]. Considering that life-threatening illnesses or injuries may occur at places where there are no medical practitioners or health service providers, it is imperative that laypeople are equipped with all the necessary knowledge and skills to provide BLS. Nevertheless, there is a tendency of people to make assumptions that BLS ought to be performed by qualified medical personnel and this has resulted in some deaths that could have been avoided. Therefore, it is necessary to assess the general public on their knowledge, and awareness about BLS; and their attitude toward BLS so that proper interventions could be performed as appropriate [2]. In the Oman population, the annual incidence of OHCA was reported in 2017, and it stated that the annual incidence ranged between 516-780 cases [3]. Furthermore, the outcomes and coronary angiography findings of patients following OHCA in Oman indicated that 13% of patients survived and were discharged, although three survivors suffered from permanent hypoxic brain damage [3]. Further, the Sultan Qaboos University Hospital in Oman observed that virtually every cardiac arrest patient admitted was brought to the hospital by friends or family relatives without being given Cardiopulmonary Resuscitation (CPR) first aid. Therefore, the foregoing situation in Oman may be attributed to lack of adequate knowledge, awareness and skills of the general public in performing BLS.
METHODS
Participants and design
A total of 426 non-medical Omani participants were included; who aged 18 or more; willing to participate in the study; and able to speak and read Arabic or English languages. Particularly, data collection took virtually one month from 28th February, 2020 until 28th March, 2020. However, cross sectional design was used and subjects were collected using non-probability convenience sampling technique. Therefore, the interested and eligible participants were approached every day during the study period from 9 am up until 6 pm in Sultan Qaboos University (SQU) public areas, waiting areas in Sultan Qaboos University Hospital (SQUH) and other public places like shopping malls, sports facilities, parks and other entertainment areas. A website-based questionnaire tool was easily accessed by the subjects.
Setting
The study setting was based in Muscat City, the Capital and largest City of the Sultanate of Oman where the majority of the population resides approximately 1,475,000 according to 2017 statistics. Therefore, those people were selected in the study to represent the study population, which can reflect positively on the sampling representativeness and generalizability. Thus, this gave more chance in attaining the required sample and increased variation of the measured variables.
Instrument
A specific, validated self-administered Arabic questionnaire was developed, which consisted of four sections. The first part which contains socio-demographic information was designed by the researcher. This part consisted of five questions that tapped information regarding participants’ age, gender, marital status, education and occupation. The second part consisted of four questions asking about participant’s awareness of BLS. The third part was about participant’s knowledge of BLS that has 15 multiple choice questions. This validated part of the questionnaire was adopted from the Author, Dr. Maha Al-Mohaissen, who had developed the original questionnaire and used it in her study, Knowledge and Attitude Toward Basic Life Support Among Health Students at a Saudi Women’s University; a cross-sectional study, which was conducted in Suadi Arabia in 2016 [4]. Her self-administered questionnaire was presented in English language with reliability test of 0.81. The questionnaire with its key answers conformed to the latest American Heart Association (AHA) BLS guidelines. The fourth part, Attitude toward BLS, was about participants’ attitude toward BLS which was Likert Rating Scale with five levels (1=Strongly disagree, 2=disagree, 3=uncertain, 4=agree and 5=strongly agree). It was adopted from the author named Dr. Anurag Bhai Patidar who used it in his study titled; Attitude of school students towards Basic Life Support in Punjab, India, 2014 [5]. The 37 items questionnaire was modified by consulting with five Ph.D experts from both the clinical and academic nursing departments in Oman. The CVI result was good with an average validity score of 92%. Furthermore, test retest reliability coefficient of the attitude scale was calculated as r=0.784. Both Forward-Backward translation with the validity of the accuracy of wording were done. The tool was tested on 20 eligible subjects prior to data collection. A website-based questionnaire tool was designed for data collection and easily accessed by the participants.
Analysis
The Statistical Package for the Social Sciences (SPSS) was used to analyze the collected data. A qualified statistician and data manager were employed to manage and analyze these data appropriately. Categorical variables were summarized as counts and percentages, whereas continuous variables, including knowledge and attitude, were summarized as means and corresponding standard deviations, or medians and Interquartile Range (IQR). Furthermore, the difference between proportions within a categorical variable was tested using the homogeneity test of proportions, while the differences in the distributions of knowledge and attitude between the categories of a socio-demographic characteristic were assessed using independent samples tests and, where necessary, the post hoc analysis was performed to detect the significance of the differences between paired comparisons, for which the Bonferroni correction was used to adjust the P values.
Ethics
Formal approval was obtained from the Ethics and Research Committee of Xiangya School of Nursing, Central South University with Reference Number I2019012. In addition, the approval letter was taken from the Medical Research Ethics Committee (MREC) of Sultan Qaboos University, Sultanate of Oman, as local approval. Also, written informed consent was obtained from all respondents who were willing to participate in the study. All information was confidential and participants were anonymous when recording their data. Participation was voluntary, and no incentives were provided. At any stage, participants could be withdrawn from the study at their will. Other than the time commitment, there were no other potential risks related to the study participants or the information they provided.
RESULTS
Sample characteristics
A total of 426 subjects were investigated in this study, of which majority were in the age groups, 28-37 years (50.0%) and 18-27 years (35.7%). In addition, majority of the subjects were female (57.0%); married (58.5%) or single (39.9%); had secondary (31.5%), diploma (27.2%), or bachelor’s (32.4%) levels of education; and worked in government (28.6%) or private sector (25.4%). Table 1 displays the results.
|
Variable |
Categories |
Frequency |
Percentage |
|
Age |
18-27 |
152 |
35.7 |
|
28-37 |
213 |
50.0 |
|
|
38-47 |
54 |
12.7 |
|
|
48+ |
7 |
1.6 |
|
|
Gender |
Male |
183 |
43.0 |
|
Female |
243 |
57.0 |
|
|
Marital status |
Married |
249 |
58.5 |
|
Single |
170 |
39.9 |
|
|
Divorced |
7 |
1.6 |
|
|
Level of education |
Primary |
9 |
2.1 |
|
Secondary |
134 |
31.5 |
|
|
Diploma |
116 |
27.2 |
|
|
Bachelor |
138 |
32.4 |
|
|
Master |
23 |
5.4 |
|
|
Doctoral |
6 |
1.4 |
|
|
Occupation
|
Government |
122 |
28.6 |
|
Private |
108 |
25.4 |
|
|
Retired |
2 |
.5 |
|
|
Housewife |
68 |
16.0 |
|
|
Self-employed |
16 |
3.8 |
|
|
Student |
74 |
17.4 |
|
|
Unemployed |
36 |
8.5 |
Table 1: Sample characteristics.
Participant’s awareness of BLS
Large proportion of the participants (62.0%) were already aware about Cardio-Pulmonary Resuscitation (CPR), but had never received any CPR training (70.9%). Nevertheless, majority of those who indicated that they had received CPR training (29.1%) specified that they had received the training from Television-Internet-Media (33.1%), at a course given by the trainers of the Ministry of Health (21.0%), CPR education institutions (12.9%) and at school (12.1%). Moreover, the participants who indicated that they had not received CPR training expressed that they intend to attend CPR training in the future (84.8%).
Participants’ level of knowledge of BLS
Generally, larger proportions of the participants responded correctly on how to find out whether collapsed person was conscious [132 (31.0%)]; how to find out if a collapsed person had a pulse [162 (38.0%)]; what to do next as an individual after confirming that the collapsed person was unconscious, not breathing and had no pulse [222 (52.1%)]; what number to call for emergency medical services [328 (77.0%)]; the location for chest compressions for adults [139 (32.6%)]; and what to do first upon witnessing an infant choking while playing with a toy but the infant was unable to cry or cough [241 (56.6%)]. Table 2 shows the results.
|
Question |
Frequency, n |
Percentage |
|
What to do when you see a person collapsed on the road |
||
|
(a) Correct response |
42 |
9.9 |
|
(b) Incorrect response |
384 |
90.1 |
|
How would you find out whether collapsed person was conscious? |
||
|
(a) Correct response |
132 |
31.0 |
|
(b) Incorrect response |
294 |
69.0 |
|
How would you find out if a collapsed person had a pulse |
||
|
(a) Correct response |
162 |
38.0 |
|
(b) Incorrect response |
264 |
62.0 |
|
If You confirm that the collapsed person is unconscious, not breathing and has no pulse. What would you do next? (Note: You are alone) |
||
|
(a) Correct response |
222 |
52.1 |
|
(b) Incorrect response |
204 |
47.9 |
|
What number would you call for emergency medical services? |
||
|
(a) Correct response |
328 |
77.0 |
|
(b) Incorrect response |
98 |
23.0 |
|
What is the location for chest compressions for adults? |
||
|
(a) Correct response |
139 |
32.6 |
|
(b) Incorrect response |
287 |
67.4 |
|
What is the correct rate of chest compression for adults and children? |
||
|
(a) Correct response |
48 |
11.3 |
|
(b) Incorrect response |
378 |
88.7 |
|
What is the correct depth of chest compression for adults |
||
|
(a) Correct response |
33 |
7.7 |
|
(b) Incorrect response |
393 |
92.3 |
|
What is the correct ratio of Cardio-Pulmonary- Resuscitation (Compression: Ventilation Ratio) for an adult when there is a single rescuer? |
||
|
(a) Correct response |
48 |
11.3 |
|
(b) Incorrect response |
378 |
88.7 |
|
What is the correct depth of chest compression for children and infants? |
||
|
(a) Correct response |
8 |
1.9 |
|
(b) Incorrect response |
418 |
98.1 |
|
What is the location for chest compressions in an infant? |
||
|
(a) Correct response |
40 |
9.4 |
|
(b) Incorrect response |
386 |
90.6 |
|
How do you give rescue breaths to infants? |
||
|
(a) Correct response |
29 |
6.8 |
|
(b) Incorrect response |
397 |
93.2 |
|
If you and your friend are having meal and your friend suddenly starts expressing symptoms of choking, what should your first response be? |
||
|
(a) Correct response |
17 |
4.0 |
|
(b) Incorrect response |
409 |
96.0 |
|
If you are witnessing an adult unresponsive victim who has been submerged in fresh water and just removed and just removed from it. He has spontaneous breathing, but he is unresponsive. What is the first step? |
||
|
(a) Correct response |
28 |
6.6 |
|
(b) Incorrect response |
398 |
93.4 |
|
If you witness an infant who suddenly starts to choke while playing with a toy. You have confirmed that he is unable to cry or cough. What should your first response be? |
||
|
(a) Correct response |
241 |
56.6 |
|
(b) Incorrect response |
185 |
43.4 |
Table 2: Public knowledge about BLS.
Distribution of knowledge total scores
Knowledge total scores of the participants were not normally distributed (W (426) = 0.917, P<0.001), with minimum knowledge total score of 0 out of 15, maximum knowledge total score of 13 out of 15, median knowledge total score of 3 out of 15 (IQR: 2 - 4), and mean ± SD knowledge total score of 3.6 ± 1.9. Note that SD stands for Standard Deviation and IQR stands for Inter Quartile Range. In addition, majority of the participants scored 3 out of 15 (27.0%), followed by 4 out of 15 (21.4%), then 2 out of 15 (17.4%). Therefore, majority of the participants had low knowledge about BLS. Figure 1 shows the results.
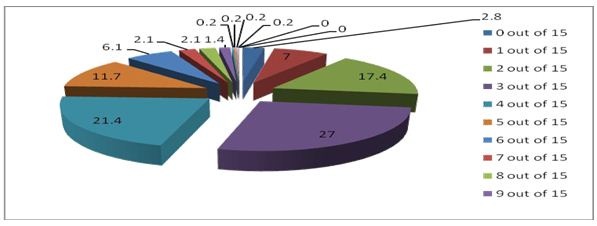 Figure 1: Knowledge total scores.
Figure 1: Knowledge total scores.
Distribution of attitude total scores
Attitude total scores of the participants weren’t normally distributed (W (426) =0.976, P<0.001), with minimum attitude total score of 30 out of 65, maximum attitude total score of 65 out of 65, median attitude total score of 55 out of 65 (IQR: 51 - 58), and mean ± SD attitude total score of 54.5 ± 5.5. Also, item scores, for each attitude item were not normally distributed (W (426) = 0.976, P<0.001). Therefore, majority of the participants had positive attitude towards BLS, which agrees with the results shown in table 3.
|
Item |
1 |
2 |
3 |
4 |
5 |
Median
|
IQR (Q1-Q3)
|
Strength of attitude
|
|
Strongly disagree
|
Disagree |
Uncertain |
Agree |
Strongly agree |
||||
|
1. Basic Life Support training should be mandatory (voluntary) to every citizen of a country. |
0 (0.0%) |
4 (0.9%) |
28 (6.6%) |
131 (30.8%) |
263 (61.7%) |
5 |
4-5 |
Strong positive |
|
2. Basic Life Support can save one’s life when administered timely. |
0 (0.0%) |
3 (0.7%) |
10 (2.3%) |
110 (25.8%) |
303 (71.1%) |
5 |
4-5 |
Strong positive |
|
3. Basic life support should be included in school curriculum. |
0 (0.0%) |
1 (0.2%) |
25 (5.9%) |
123 (28.9%) |
277 (65.0%) |
5 |
4 - 5 |
Strong positive |
|
4. Basic Life Support training should only be made mandatory to those handling casualties regularly such as the policemen, fire-workers, and home guards. |
100 (23.5%) |
136 (31.9%) |
58 (13.6%) |
49 (11.5%) |
83 (19.5%) |
4 |
2 - 4 |
Positive |
|
5. Basic life support training for the general public should be adequate to prepare them for providing basic life support. |
1 (0.2%) |
6 (1.4%) |
28 (6.6%) |
152 (35.7%) |
239 (56.1%) |
5 |
4 - 5 |
Strong positive |
|
6. BLS training increases an individual’s confidence in providing basic life support. |
0 (0.0%) |
2 (0.5%) |
17 (4.0%) |
162 (38.0%) |
245 (57.5%) |
5 |
4 - 5 |
Strong positive |
|
7. Death due to cardiac arrests can be minimized if Automated External Defibrillator (AED) is made available in public places. |
5 (1.2%) |
15 (3.5%) |
61 (14.3%) |
177 (41.5%) |
168 (39.4%) |
4 |
4 - 5 |
Positive |
|
8. Automatic external defibrillators (AED) should be installed in public places. |
7 (1.6%) |
15 (3.5%) |
94 (22.1%) |
165 (38.7%) |
145 (34.0%) |
4 |
3 - 5 |
Positive |
|
9. Basic life support can be provided even to the strangers. |
1 (0.2%) |
11 (2.6%) |
44 (10.3%) |
169 (39.7%) |
201 (47.2%) |
4 |
4 - 5 |
Positive |
|
10. A country-wide emergency medical service (EMS) number is necessary to when responding to emergency situations. |
4 (0.9%) |
2 (0.5%) |
12 (2.8%) |
86 (20.2%) |
322 (75.6%) |
5 |
5 - 5 |
Strong positive |
|
11. Fear of legal actions can hinder you to perform basic life support. |
14 (3.3%) |
45 (10.6%) |
92 (21.6%) |
161 (37.8%) |
114 (26.8%) |
4 |
3 - 5 |
Positive |
|
12. Providing BLS to someone in need is a moral responsibility of every citizen of a country. |
6 (1.4%) |
9 (2.1%) |
33 (7.7%) |
190 (44.6%) |
188 (44.1) |
4 |
4 - 5 |
Positive |
|
13. Only health professionals (eg., nurse, doctors) should provide BLS. |
61 (14.3%) |
153 (35.9%) |
103 (24.2%) |
65 (15.3%) |
44 (10.3%) |
4 |
2 - 4 |
Positive |
Table 3: Item Level Responses for the Attitude Scale.
Distribution of BLS knowledge and attitude across the socio-demographic variables
In order to see whether participants’ knowledge and attitude of BLS differed with respect to the socio-demographic variables, the distributions of the BLS knowledge and attitude total scores were compared between the categories of the socio-demographic variables. Considering that both BLS knowledge and attitude total scores were either not normally distributed, or measured on a smaller number of subjects in the respective categories of the socio-demographic variables, non-parametric tests were used to assess the significance of any difference in distributions across the foregoing socio-demographic variable categories. Therefore, the independent samples Kruskal Wallis H test was used to compare the distributions among more than two categories, whereas the Mann Whitney U test was used to compare the distributions between two categories. The results indicated that, although the participants were generally poor in knowledge about BLS, male participants were more knowledgeable than female participants. In addition, those with Doctoral level of education were more knowledgeable than those who had primary, secondary, master, bachelor, and diploma levels of education. Besides, those with occupation in Government and Private sector were more knowledgeable than housewives and students (Table 4a). However, the level of attitude towards BLS was the same across the categories of the socio-demographic variables (Table 4b).
|
Categories Frequency Knowledge P value total scores Mean ± SD |
||||
|
Age |
18-27 |
152 |
3.5 ± 1.8 |
|
|
28-37 |
213 |
3.7 ± 1.9 |
|
|
|
38-47 |
54 |
3.4 ± 1.8 |
|
|
|
48+ |
7 |
4.3 ± 3.9 |
0.471H |
|
|
Gender |
Male |
183 |
3.9 ± 2.1 |
|
|
Female |
243 |
3.4 ± 1.7 |
0.005U |
|
|
Marital status |
Married |
249 |
3.7 ± 1.9 |
|
|
Single |
170 |
3.4 ± 1.7 |
|
|
|
Divorced |
7 |
4.0 ± 4.0 |
0.105H |
|
|
Level of education |
Primary |
9 |
3.0 ± 1.0 |
|
|
Secondary |
134 |
3.4 ± 1.9 |
|
|
|
Diploma |
116 |
3.8 ± 2.0 |
|
|
|
Bachelor |
138 |
3.5 ± 1.7 |
|
|
|
Master |
23 |
3.9 ± 3.1 |
|
|
|
Doctoral |
6 |
5.3 ± 1.0 |
0.030H |
|
|
Occupation |
Government |
122 |
4.0 ± 2.1 |
|
|
Private |
108 |
4.0 ± 2.2 |
|
|
|
Retired |
2 |
2.5 ± 0.7 |
|
|
|
Housewife |
68 |
2.8 ± 1.2 |
|
|
|
Self-employed |
16 |
3.8 ± 2.4 |
|
|
|
Student |
74 |
3.1 ± 1.6 |
|
|
|
Unemployed |
36 |
3.4 ± 1.3 |
<0.001H |
|
Table 4a: Distribution of BLS knowledge across the socio-demographic variables.
HKruskal Wallis H test; and UMann Whitney U test.
|
Variable |
Categories |
Frequency |
Attitude total scores Mean ± SD |
P value |
|
Age |
18-27 |
152 |
54.1 ± 5.6 |
|
|
28-37 |
213 |
54.6 ± 5.6 |
|
|
|
38-47 |
54 |
55.3 ± 5.0 |
|
|
|
48+ |
7 |
55.3 ± 5.2 |
0.604H |
|
|
Gender |
Male |
183 |
54.3 ± 6.1 |
|
|
Female |
243 |
54.7 ± 5.0 |
0.831U |
|
|
Marital status |
Married |
249 |
54.8 ± 5.3 |
|
|
Single |
170 |
54.0 ± 5.8 |
|
|
|
Divorced |
7 |
56.0 ± 3.8 |
0.466H |
|
|
Level of education |
Primary |
9 |
49.3 ± 9.2 |
|
|
Secondary |
134 |
54.2 ± 5.5 |
|
|
|
Diploma |
116 |
54.8 ± 4.9 |
|
|
|
Bachelor |
138 |
55.1 ± 5.6 |
|
|
|
Master |
23 |
54.4 ± 5.1 |
|
|
|
Doctoral |
6 |
51.7 ± 5.5 |
0.200H |
|
|
Occupation |
Government |
122 |
54.4 ± 6.2 |
|
|
Private |
108 |
54.9 ± 5.4 |
|
|
|
Retired |
2 |
54.5 ± 3.5 |
|
|
|
Housewife |
68 |
53.7 ± 5.0 |
|
|
|
Self-employed |
16 |
56.0 ± 4.4 |
|
|
|
Student |
74 |
54.3 ± 5.6 |
|
|
|
Unemployed |
36 |
55.2 ± 4.9 |
0.471H |
Table 4b: Distribution of BLS attitude across the socio-demographic variables.
HKruskal Wallis H test; and UMann Whitney U test.
DISCUSSION
Level of public awareness towards BLS
Although a cross-sectional survey, which was carried out in 5 cities in the Sultanate of Oman, found that there is low effort in making the general public in Oman aware of the importance of CPR, which was manifested by the 60% of lay people surveyed, who indicated that they did not know how to perform CPR [6], this study found that a large proportion of the participants (62.0%) were already aware about Cardio-Pulmonary Resuscitation (CPR).
Despite having awareness about CPR, 70.9% of this proportion had indicated that they hardly received any CPR training, besides, majority of the participants who indicated that they had not received CPR training expressed that they intended to attend CPR training in the future (84.8%). This result, therefore, suggests that most nonmedical adults in Muscat have the motivation to receive training in CPR. Therefore, it is imperative that awareness campaigns about BLS should be accompanied by training people in the necessary skills for carrying out BLS activities in the study area. Moreover, majority of those who indicated that they had received CPR training (29.1%) specified that they had received the training from Television-Internet-Media (33.1%), at a course given by the trainers of the Ministry of Health (21.0%), CPR education institutions (12.9%) and at school (12.1%). The proportion of those that had received training in this study is much lower than this proportion in a cross-sectional survey, which was carried out between March and May 2014 in 5 cities of the Sultanate of Oman (38.9%) [7], that among an adult sample from a busy street in a city of a western region of Turkey (40.7%) [2], but comparable with 30.0% which was reported in the UK among Greater London residents [8], 35% which was reported in the Japanese general population [9]. Lower rates of individuals attending BLS training were also reported in Singapore [10].
Level of public knowledge toward BLS
Majority of the nonmedical adults did not know to find out whether a collapsed person was conscious (69%), or had a pulse (62%), suggesting that they were very unlikely save an unconscious collapsed person, hence a large proportion of unconsciousness due to collapsing in Muscat may have poor outcomes after referral to the hospital. However, substantial number of the participants indicated that they would activate emergency medical service (52.1%) after confirming that the collapsed person was unconscious, and majority of the participants (77.0%) identified the correct number (9999) to call for emergency medical services. This is an encouraging outcome which still needs strengthening in order to increase the number of people who would effectively activate emergency medical services in the face of an emergency. Furthermore, in this study, only 32.6% of the participants responded correctly on the location of chest compressions during CPR. This proportion is far much lower than that among individuals aged ≥18 years on a busy street in a city of a western region of Turkey (52.0%) [2], but comparable with the proportion of the same among lay public in the Republic of Slovenia (37.6%) [11]. Additionally, a cross-sectional survey, which was carried out in 5 cities in the Sultanate of Oman, found that 60% of the participants had no appreciation of the need for CPR in a hypothetical scenario in an unconscious child who chocked on a piece of fruit [7]. However, in this study, a comparable proportion correctly indicated that, upon witnessing an infant choking while playing with a toy but the infant was unable to cry or cough, they would perform back blows and chest compression of five cycles each, then open the mouth and remove the foreign body only when seen (56.6%). In contrast, another comparable proportion incorrectly indicated that, upon observing a friend expressing symptoms of chocking when having a meal, they would give back blows on the victim (57.7%). Thus, a considerable number of nonmedical adults in Muscat do not have prerequisite knowledge for training in first aid skills for helping individuals experiencing chocking and proper interventions in this regard would be cost efficient among this study population. In relation to helping an adult unresponsive victim who had been submerged in fresh water then was just removed from it and was showing signs of spontaneous breathing, but unresponsive, a larger proportion of the participants (39.4%) responded incorrectly on what they would do first in order to help such an adult person. According to the World Health Organization (WHO), drowning is a serious but neglected public health threat that claims the lives of approximately 372, 000 people per year worldwide [12].
Association between level of public knowledge toward BLS and sociodemographic variables
Although the participants were generally poor in knowledge about BLS, this study found that there was an association between some socio-demographic variables and the level of knowledge toward BLS. Specifically, gender, level of education and occupation were associated with it. For example, males were more knowledgeable than females. Also, those with Doctoral educational level were more knowledgeable than those in other educational level; whereas those working in Government and Private sectors were more knowledgeable than housewives and students.
The study finding of males were more knowledgeable than females is consistent with the findings of some previous study [13]. Moreover, it agrees with the recent findings that the Omani females are much lagging behind in literate life expectancy than the Omani males [14]. Therefore, this finding underscores the need to reduce the gap in BLS knowledge between males and females so that both of these gender groups could confidently and skillfully provide BLS services.
Furthermore, just like in this study, several studies have demonstrated that knowledge of BLS has been poor among the levels of education, such as primary, secondary, and college [15-17]. Although the doctoral level of education group was associated with better knowledge of BLS than the other groups of education, their knowledge was still inadequate. Therefore, this outcome suggests that introducing BLS training in the school’s curriculum at all levels would pay great dividends for the prevention of deaths resulting from cardiac arrest or other emergency life threatening events. Also, that housewives and students demonstrated to have poorer knowledge in BLS than private and government workers in this study is consistent with the findings of other similar studies [4,18]. Thus, the housewives need not be left out when conducting interventions to improve knowledge in BLS among the laypeople of Muscat in Oman. The housewives stay with children at home most of their time and if they do not have adequate skills to provide first aid to fatal accidents involving the kids, then the prevalence of poor outcomes in relation to such type of accidents would increase. Therefore, BLS training for housewives in the study area is warranted just as for the other categories of workers.
PUBLIC ATTITUDE
It was found that all participants had a positive attitude toward BLS. This was an encouraging result, which suggests that many people in this area would be willing to attend training in BLS, should there be an initiative to train them. This finding is consistent with some previous prospective and cross-sectional study on senior undergraduate student-teachers enrolled at a South African university, which found that the student-teachers surveyed displayed poor knowledge and perceptions but positive attitudes with regards to the practice of CPR and BLS, and this suggested that formal CPR training was supposed to be part of the curriculum for teachers [19]. The BLS training increases laypersons' confidence and willingness to perform bystander CPR on a stranger [20,21]. However, laypersons are more willing to perform hands only CPR rather than to perform standard CPR on a stranger regardless of the BLS training. Despite socio-demographic characteristics being associated with the level of knowledge, they were not associated with the level of attitude in this study. This is not a surprising result considering that all the participants had virtually same level of attitude toward BLS, which is a great factor in making BLS training effective among the study population.
LIMITATION
Convenience sampling method was used to obtain participants, which is susceptible to selection bias. However, the large sample size might have minimized the possibility of selection bias due to this sampling method. Second, the cross-sectional design of this study could not establish the causal effect of socio-demographic characteristics on the level of knowledge. Therefore, prospective studies are warranted to confirm the observed associations between socio-demographic characteristics and the level of knowledge. Finally, when performing group comparisons of knowledge and attitude, some groups such as the 48+ years old, the divorced, the primary and doctoral levels of education and the retired groups, had far much smaller numbers of subjects, which might have compromised the statistical power.
CONCLUSION
This study suggested that there is a huge gap between awareness of BLS and having skills in BLS. Also, the level of knowledge about BLS was very low among the study population but there were still differences in the level of knowledge with respect to the socio-demographic characteristics. In contrast, this study proved that all participants had a positive attitude toward BLS. Finally, considering the increasing rate of illnesses and injuries that require BLS measures in Oman, policymakers in Oman should advocate mandatory training in BLS for all nonmedical population in the country. Furthermore, incorporating BLS teaching in the school curriculum would be helpful for ensuring that many students acquire the necessary knowledge and skills to provide BLS services when needed. Also, learning from and using other people’s experiences in other population as regards BLS training would help increase the knowledge and awareness of BLS, hence increasing the chances that more lives would be saved.
ACKNOWLEDGMENT
I would like to express my earnest thanks to my research instructor Professor Gu Can for bestowing valuable suggestions, guidance and support and to the academic and technical support of Central South University to accomplish this article successfully.
FUNDING
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
REFERENCES
- WIKIPEDIA (2011) Basic life support.
- Özbilgin S, Akan M, Hanci V, Aygün C, Kuvaki B (2015) Evaluation of Public Awareness, Knowledge and Attitudes about Cardiopulmonary Resuscitation: Report of Izmir. Turk J Anaesthesiol Reanim 43: 396-405.
- Nadar SK, Mujtaba M, Al-Hadi H, Sadiq M, Al-Riyami A, et al. (2018) Epidemiology, Outcomes and Coronary Angiography Findings of Patients Following Out-of-Hospital Cardiac Arrest: A single-centre experience from Oman. Sultan Qaboos Univ Med J 18: 155-160.
- Al-Mohaissen MA (2017) Knowledge and Attitudes Towards Basic Life Support Among Health Students at a Saudi Women's University. Sultan Qaboos Univ Med J 17: 59-65.
- Patidar AB, Sharma A (2014) Attitude of school children towards basic life support in Punjab, India. Int J Health Sci Res 4: 193-201.
- Al-Shaqsi S, Al-Risi A, Al-Kashmiri A (2018) Do Lay People in Oman Know How to Perform Cardiopulmonary Resuscitation? Oman Med J 33: 178.
- Al Shaqsi S, Al Wahaibi K, Al Risi A (2015) Wasted Potential: Awareness of Basic Cardiopulmonary Resuscitation in the Sultanate of Oman- A Cross-Sectional National Survey. J Eme Med Int Care 1: 105.
- Donohoe RT, Haefeli K, Moore F (2006) Public perceptions and experiences of myocardial infarction, cardiac arrest and CPR in London. Resuscitation 71: 70-79.
- Kuramoto N, Morimoto T, Kubota Y, Maeda Y, Seki S, et al. (2008) Public perception of and willingness to perform bystander CPR in Japan. Resuscitation 79: 475-481.
- Ong MEH, Quah JLJ, Ho AFW, Yap S, Edwin N, et al. (2013) National population based survey on the prevalence of first aid, cardiopulmonary resuscitation and automated external defibrillator skills in Singapore. Resuscitation 84: 1633-1636.
- Rajapakse R, Noc M, Kersnik J (2010) Public knowledge of cardiopulmonary resuscitation in Republic of Slovenia. Wien Klin Wochenschr 122: 667-672.
- World Health Organization (2014) Global report on drowning: Preventing a leading killer. WHO, Geneva, Switzerland.
- Krammel M, Schnaubelt S, Weidenauer D, Winnisch M, Steininger M, et al. (2018) Gender and age-specific aspects of awareness and knowledge in basic life support. PloS one 13: 0198918.
- Islam MM, Khan MHR (2019) Literate Life Expectancy and Its Gender Differentials in Oman. Journal of Reliability and Statistical Studies 12: 21-31.
- Joseph N, Kumar G, Babu Y, Nelliyanil M, Bhaskaran U (2014) Knowledge of first aid skills among students of a medical college in mangalore city of South India. Ann Med Health Sci Res 4: 162-166.
- Aaberg AM, Larsen CE, Rasmussen BS, Hansen CM, Larsen JM (2014) Basic life support knowledge, self-reported skills and fears in Danish high school students and effect of a single 45-min training session run by junior doctors; a prospective cohort study. Scand J Trauma Resusc Emerg Med 22: 24.
- Almesned A, Almeman A, Alakhtar AM, AlAboudi AA, Alotaibi AZ, et al. (2014) Basic life support knowledge of healthcare students and professionals in the Qassim University. Int J Health Sci (Qassim) 8: 141-150.
- Ahmad A, Akhter N, Mandal RK, Areeshi MY, Lohani M, et al. (2018) Knowledge of basic life support among the students of Jazan University, Saudi Arabia: Is it adequate to save a life? Alexandria journal of medicine 54: 555-559.
- Ojifinni K, Motara F, Laher AE (2019) Knowledge, Attitudes and Perceptions Regarding Basic Life Support Among Teachers in Training. Cureus 11: 6302.
- Pehlivan M, Mercan NC, Çinar I, Elmali F, Soyöz M (2019) The evaluation of laypersons awareness of basic life support at the university in Izmir. Turk J Emerg Med 19: 26-29.
- Abolfotouh MA, Alnasser MA, Berhanu AN, Al-Turaif DA, Alfayez AI (2017) Impact of basic life-support training on the attitudes of health-care workers toward cardiopulmonary resuscitation and defibrillation. BMC health services research 17: 674.
Citation: Aldhakhri A, Can G (2020) Evaluation of Public Awareness, Knowledge and Attitudes towards Basic Life Support among Non-Medical, Adult Population in Muscat City, Oman: Cross-Sectional Study. J Non Invasive Vasc Invest 5: 025.
Copyright: © 2020 Aisha Aldhakhri, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.