Journal of Alternative Complementary & Integrative Medicine Category: Medicine
Type: Short Communication
Evaluation of the Efficacy on Patients Suffering from Alzheimer’s Disease of Anti-Radiation Screens and Protective Patches to Preserve them from the Effects of Artificial Electromagnetic Fields and Natural Radiation
*Corresponding Author(s):
Francesca UbertiLaboratory Of Physiology, Department Of Translational Medicine, University Of Piemonte Orientale, Via Solaroli 17, Novara, 28100, Italy
Tel:+39 0323933913,
Email:francesca.uberti@med.uniupo.it
Received Date: Feb 07, 2019
Accepted Date: Feb 12, 2019
Published Date: Feb 26, 2016
Abstract
Today the scientific community is showing a growing interest in the health influence of artificial electromagnetic fields generated by electrical or electronic systems or ionizing natural radiations. Several studies identify the body’s exposure to artificial electromagnetic fields and natural radiation as a common environmental cause of Alzheimer’s disease. In this context, it is very important to prevent exposure for Alzheimer’s patients in order to reduce the risk of rapid disease progression. Currently, some devices are available to shield living organisms from the potential harmful effects of electromagnetic fields and natural ionizing radiation from the ground. The purpose of this study is to study for the first time the benefits of protection from environmental phenomena on patients with Alzheimer’s disease. The aim is to verify if they are no longer stressed by artificial electromagnetic pollutants and natural radiation, and can benefit from them, such as the slowing down of the progression of the disease.
Keywords
Alzheimer’s Disease, Electromagnetic Fields, Natural Radiation
INTRODUCTION
Power lines that carry high voltage electricity are ubiquitous in urban areas of industrialized countries. Similar to what happens for every electrical device, electric lines generate electric and magnetic fields that are called low-frequency Electromagnetic Fields (EMF) and can affect both animal and human health [1-3]. The electromagnetic sources can be classified in natural or artificial electromagnetic sources with static fields, at extremely low, at intermediate and at radio frequency respectively. In recent years, several histological and physiological studies have assessed the effects of electromagnetic fields on health, observing the presence of a variety of adverse effects in vivo such as influencing learning and memory. There are also effects on cardiovascular, reproductive, nervous, endocrine and immune systems. As well as alterations of biological functions in humans and animals [4-9]. Furthermore, electromagnetic fields have been implicated in multiple adverse effects on human health, including increased risk of brain cancer, genotoxicity and neurodegenerative diseases, de novo mutations, amyotrophic lateral sclerosis, depression and Alzheimer’s Disease (AD) [10]. For this reason, the effect of electromagnetic fields on the living organism is considered a complex phenomenon. Another important factor that can induce a high risk of adverse health effects is the natural sources of ionizing radiation, which are ubiquitous in the world. Specific tissues differ significantly in their sensitivity to the electromagnetic field [11]. Although effects on gene expression in tissues and cell lines have been observed, the significance of low dose exposures for cell survival, tissue damage and individual health have not yet been fully understood. In addition, radiation exposure of the human brain has been associated with neurological damage and cognitive impairment: high-dose radiation can cause demyelination and neuronal loss associated with neuronal and cognitive deficiencies [12]. Some of these cognitive alterations have been observed also as a consequence of impaired neurogenesis following exposure to ionizing radiations [13-17]. A recent work suggests that even exposures at relatively low doses, such as from computed tomography, could trigger mechanisms associated with cognitive dysfunction that characterize normal aging and AD [11]. Regardless of the energy source, after the initial transduction event, there is a cascade of biophysical and biochemical events that result in an observable physiological and / or behavioral damage [18]. Evidence has shown that the effects of radiation in the central nervous system are more pronounced; ionizing radiations induces vascular abnormalities, demyelination and alterations in the microenvironment of the brain, shifting the proliferative response of progenitors from neurogenesis to gliogenesis [15,19]. In this context, some organizations such as International Commission on Non- Ionizing Radiation Protection (ICNIRP ) and American Conference of Governmental Industrial Hygienists ( ACGIH ) have established occupational exposure threshold limits for ELF-MF (whole body ceiling exposure limit in 60Hz for ACGIH and ICNIRP: 1 mT). For this reason, ELF-MF is classified as “possibly carcinogenic to humans” agent by the International Agency for Research on Cancer [20-22]. AD is the leading cause of dementia and the fourth leading cause of death. For this reason, it is absolutely crucial to better understand the various contributing factors and the molecular pathogenesis as part of an AD prevention strategy [19]. AD is a progressive irreversible neurodegenerative disease and the initial stage of the pathogenetic mechanism seems to start 10 years or more before the first clinical symptoms [23]. AD is characterized by the accumulation of neuritic plaques and neurofibrillary tangles, which are accumulated in the brain of AD patients, resulting from increased production or reduced clearance, associated with inflammation, oxidative stress, neuronal loss and ultimately results in AD-related cognitive impairment [19,24,25]. Slight AD risk resulting from non-IR exposure (such as extremely low frequency electromagnetic fields - ELF-EMF) has been described [22]. The first epidemiological study on AD was published by Sobel et al., who reported that occupational exposure to ELF-MF above 0.2 mT might elevate the risk for AD [26]. Following this study, more attention was drawn to this disease and further epidemiological studies have been performed [27]. For example, Roosli et al., found a higher AD risk for train drivers and shunting yard engineers, which were highly exposed to 16.7 Hz compared to lower exposed station masters [28].
However, studies that evaluate the effectiveness of protective devices from electromagnetic field on AD patients are still lacking. The purpose of this study was therefore the assessment of the effectiveness of one of these commercial devices in protecting AD patients in order to verify if they are no longer stressed by artificial electromagnetic and can have some benefit using it.
However, studies that evaluate the effectiveness of protective devices from electromagnetic field on AD patients are still lacking. The purpose of this study was therefore the assessment of the effectiveness of one of these commercial devices in protecting AD patients in order to verify if they are no longer stressed by artificial electromagnetic and can have some benefit using it.
MATERIALS AND METHODS
Protective devices
The effectiveness of two commercial hi-tech devices on AD patients was investigated. In particular to carry out this study, Skudo® patches and Geoprotex® anti-radiation screens (both from Edil Natura S.r.l., Novara, Italy) were used. Both devices are designed for the protection of the body from external electromagnetic disturbances but they are not medical devices. In particular, Skudo® patches (patented and certified at European level No. 2073611) protect micro areas of the body, as previously described, whereas Geoprotex® anti-radiation screen protects large areas or particular portions of the environment, which in this study is restricted to the only bed area [29]. Moreover, these screens have been tested/certified by Nuclear Engineering Laboratory of Polytechnic of Milan (for the part concerning X and Gamma ionizing radiations) and the Institute of Nuclear Physics of Italy (for the part concerning radon gas protection). Both devices do not release substance, have no side effect and have no time limitations.
Subject enrolled
In this study, 9 Italian AD patients (4 male and 5 women) were enrolled within the hospital “Residence Alzheimer’s Disease” (Varese) between 70 and 85 years of age, subject to written authorization at the hospital. The approval for this study was conferred by the local Human Investigation Committee. To ensure the homogeneity of the study, the patients enrolled have been diagnosed with AD for at least 2 years and they must be independent in walking and feeding. Patients with autoimmune diseases; skin allergies; hypertension; surgery or critical medical history within the year prior to the study; metallic implants in the body; chronic diseases; contraindications for electrical stimulation were inappropriate for the study. During the clinical experimentation the patients consume at least 2 liters of water per day, to optimize the protection exerted by devices. The drug therapy was not modified in any way. The control of the patient clinical parameters was made each week. At the end of each month (in particular at day 21 of each month) the obtained data were collected and compared with those precedents (6 months total clinical experimentation period), or rather before clinical experimentation.
Parameters analyzed
All tests performed on AD patients were applied by operators, hospital attendants, educators and physiotherapists, which they were able to follow the study and to use the validate scales. In particular Tinetti test to evaluate balance and ambulation, Barthel scale to investigate the independence degree in the functions of daily life, and Mini Mental State Evaluation (MMSE) to verify mental deterioration degree, were applied to AD patients before starting the study and at each month of experimentation (6 total months) [30-32]. The times of measurement were divided in 3 steps: basal (before the investigation), 3 months without devices, 3 months with devices (Skudo® and Geoprotex® applied together). Patches Skudo® was applied to AD patients as previous described and Geoprotex® mats were placed under the mattress of the patients [29].
STATISTICAL ANALYSIS
The raw data were processed using Prism GraphPad statistical software for normalization, peak picking and comparison between groups. The images were produced directly by BFB-Z and Image J. One-way Analysis for Variance (ANOVA) with Tukey’s post hoc tests was carried out for the comparison between groups, and all results were expressed as mean ± SD. Differences were considered to be statistically significant with a p value < 0.05.
RESULTS AND DISCUSSION
People are exposed daily to natural radiation sources as well as human-made sources. Natural radiation comes from many sources including more than 60 naturally-occurring radioactive materials. In addition, people are also exposed to natural radiation from cosmic rays, particularly at high altitude. On average, 80% of the annual dose of background radiation that a person receives is due to naturally occurring terrestrial and cosmic radiation sources. Background radiation levels vary due to geological differences. Exposure in certain areas can be more than 200 times higher than the global average [33]. These electromagnetic signals were found to be able to produce molecular changes due to either ionizing properties of radiation or increased thermal agitation of water. Life is based on water that represents its universal support. Many studies have been carried out on the electromagnetic properties of water and on its behavior when it is exposed to electromagnetic fields [34]. The water molecule, subjected to irradiation, absorbs the energy of the electromagnetic waves, and this absorption results in a vibration of the water molecule. These molecules may be able to interfere with all the metabolic reactions of the cells, from enzymatic activity to protein synthesis, up to the processes of cell replication [29]. In a previous work the effectiveness of the Skudo® patches was demonstrated in protecting the organism from the effects of electromagnetic fields [29]. In particular the effectiveness of patches was manifested in rebalancing the energies of the individuals, preventing the alteration of the body’s water system; Skudo®patches determines a regularization of the bioenergy levels correlated with the water system. Also in this study, Skudo® patches were used to protect the body of the patients. In particular, the selected points were 6CV, 17CV and 3GV which were chosen belong to the conception vessel (Ren Mai) and governor vessel (Du Mai). Ren Mai represents a fundamental level of energetic functioning and controls Sea of Yin meridians and circulates YinQi, including Blood, Essence, and Body Fluids [35]. 6CV and 17CV patches correspond to the lower dantian and the middle dantian, respectively. The third patch was placed on the lower back in the depression below the spinous process of the second lumbar vertebra, which corresponds to the point called Mingmen, the centre of vitality and original life. This area is important to treat heat disorders [35]. In addition, to maximize the protection the Geoprotex® anti-radiation mats were applied to the bed area. The anti-radiation mats consist of a larger screen, to be inserted between the bed and the mattress of the patient’s bed, and a smaller one, to be placed on the headboard of the patient’s bed. Basing on this previous data, in this study, the effects of Geoprotex® and Skudo® patches against magnetic fields applied together on AD patients were evaluated. The AD patients were selected as the optimal experimental model to evaluate the progress of the general state of health. This disease provides a constant and progressive decay due to the malfunctioning of the metabolism of nerve cells. Therefore every factor able to influence positively the neuronal metabolism is easily observable. The experiments were performed starting from analyzing the basal level without devices, as reported in figure 1; in particular the analysis of Barthel scale (panel A) showed 6 patients with low level of autonomy and 3 in normal values for AD condition. In addition, Tinetti test (panel B) reported that all patients (n=9) were in normal range value for AD condition and MMSE proved that 8 patients were in normal range and only one was in most compromised mental condition. These observations were important to explore the conditions of AD patients before applied the devices in order to verify each modifications after devices. These data are common to all AD patients at 2 years from diagnosis. Skudo® patches and Geoprotex®mates were applied to all participants (n=9) for 3 months and monitored each month. At the end of this period the results obtained from Barthel scale, Tinetti test and MMSE were investigated (Figure 1). Barthel scale showed a non linear trend during this period with a tendency to improve the daily functionality compared to basal condition: at 3 months 4 patients showed a better profile compared to 3 of the basal condition. Similarly Tinetti test reported an increase on the balance ambulation parameters about 5% compared to basal condition; indeed 5 patients had improved their condition. Finally, MMSE test confirmed the improvement observed by other tests: 3 patients had a better profile compared to baseline.
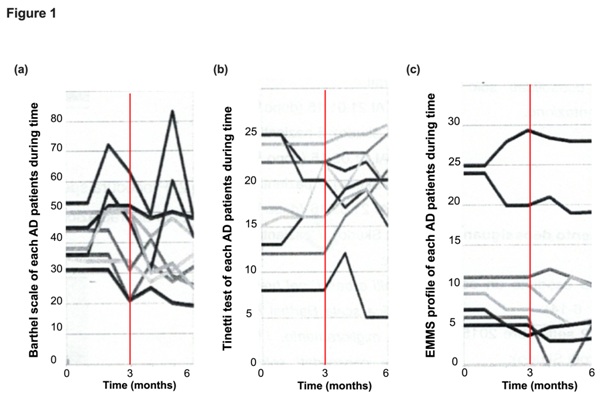
Figure 1: Analysis of the measurements with or without Skudo® and Geoprotex® devices on AD patients.
In (a) the Barthel scale, in (b) Tinetti test and in (c) MMSE observed during time on n=9 AD patients.
Moreover the graphic trend of all tests used was not linear, the data reported unexpected improvement in all parameters which could be further increase or stabilized during time. This demonstrates that Skudo®protection system, applied in specific acupuncture points, and the Geoprotex® mats, able to protect from artificial electromagnetic fields and soil magnetic fields, prevent environmental perturbations and their interaction with the body exacerbating a pre-existing disease.
In (a) the Barthel scale, in (b) Tinetti test and in (c) MMSE observed during time on n=9 AD patients.
Moreover the graphic trend of all tests used was not linear, the data reported unexpected improvement in all parameters which could be further increase or stabilized during time. This demonstrates that Skudo®protection system, applied in specific acupuncture points, and the Geoprotex® mats, able to protect from artificial electromagnetic fields and soil magnetic fields, prevent environmental perturbations and their interaction with the body exacerbating a pre-existing disease.
CONCLUSION
The study was carried out on patients suffering from a chronically degenerative pathology such as Alzheimer’s disease, from which it is possible to expect a worsening or at most maintenance of basic skills. The improvements observed on patients after the second month of application of the devices thus highlight the impact of environmental factors on the course of the disease. The results collected showed for the first time that subtracting the influences of radiation, the indicators of disease progression were significantly reduced. Therefore it can be hypothesized that the metabolism of the nervous system of these patients has improved by the application of Skudo® and Geoprotex® devices. The results of this study must be considered as preliminary data since they are obtained from a small number of participants. In the future it would be appropriate to study a larger number of subjects, adding the evaluation of some indicators specific for cerebral metabolism.
DATA AVAILABILITY
All data reported have been obtained from experiments carried out in RSA, Gerenzano (VA)
CONFLICTS OF INTEREST
The authors declare that they have no conflicts of interest.
ACKNOWLEDGMENT
The authors thank Edil Natura S.r.l. for the valuable help and for donation of Skudo® patches and Geoprotex® mats (European Patent n° 2073611).
REFERENCES
- Shaban E, Azab AE, Albasha MO, Albishti N (2016) The biological effects of electromagnetic fields on human and experimental animals. International Research Journal of Natural and Applied Sciences 3: 106-121.
- Zaghloul MS (2009) Histological study on the effects of electromagnetic field on the liver of albino rats. Egypt J Histol 32: 165-172.
- Abo-Neima SE, Motaweh HA, Ragab MF (2015) Effects of electric field on histopathological study, electrical properties and enzymes function of liver of albino rats. Inter J Eng Sci 4: 25-37.
- Khayyat LI (2011) The histopathological effects of an electromagnetic field on the kidney and testis of mice. Eurasia J Biosci 5: 103-109.
- Hashem MA, El-Sharkawy NI (2009) Hemato-biochemical and immunotoxicological effects of low electromagnetic field and its interaction with lead acetate in mice. Iraqi J Veter Sci 23: 105-114.
- Zare S, Alivandi S, Ebadi AG (2007) Histological studies of the low frequency electromagnetic fields effect on liver, testes and kidney in guinea pigs. World Appl Sci J 2: 509-511.
- Szemerszky R, Zelena D, Barna I, Bárdos G (2010) Stress-related endocrinological and psychopathological effects of short- and long-term 50Hz electromagnetic field exposure in rats. Brain Res Bull 81: 92-99.
- Ahlbom A (2001) Neurodegenerative diseases, suicide and depressive symptoms in relation to EMF. Bioelectromagnetics 5: 132-143.
- Hossmann KA, Hermann DM (2003) Effects of electromagnetic radiation of mobile phones on the central nervous system. Bioelectromagnetics 24: 49-62.
- Sobel E, Dunn M, Davanipour Z, Qian Z, Chui HC (1996) Elevated risk of Alzheimer’s disease among workers with likely electromagnetic field exposure. Neurol 47: 1477-1481.
- Lowe XR, Bhattacharya S, Marchetti F, Wyrobek AJ (2009) Early brain response to low-dose radiation exposure involves molecular networks and pathways associated with cognitive functions, advanced aging and Alzheimer’s disease. Radiat Res 171: 53-65.
- Abayomi OK (2002) Pathogenesis of cognitive decline following therapeutic irradiation for head and neck tumors. Acta Oncol 41: 346-351.
- Rola R, Sarkissian V, Obenaus A, Nelson GA, Otsuka S, et al. (2005) High-LET radiation induces inflammation and persistent changes in markers of hippocampal neurogenesis. Radiat Res 164: 556-560.
- Mizumatsu S, Monje ML, Morhardt DR, Rola R, Palmer TD, et al. (2003) Extreme sensitivity of adult neurogenesis to low doses of X-irradiation. Cancer Res 63: 4021-4027.
- Monje ML, Mizumatsu S, Fike JR, Palmer TD (2002) Irradiation induces neural precursor-cell dysfunction. Nat Med 8: 955-962.
- Yin E, Nelson DO, Coleman MA, Peterson LE, Wyrobek AJ, et al. (2003) Gene expression changes in mouse brain after exposure to low-dose ionizing radiation. Int J Radiat Biol 79: 759-775.
- Lowe XR, Marchetti F, Lu X, Wyrobek AJ (2009) Molecular stress response in the CNS of mice after systemic exposure to interferon-alpha, ionizing radiation and ketamine. Neurotoxicology 30: 261-268.
- Binhi VN, Prato FS (2016) A Physical Mechanism of Magnetoreception: Extension and Analysis. Bioelectromagnetics 38: 41-52.
- Begum N, Wang B, Mori M, Vares G, et al. (2012) Does ionizing radiation influence Alzheimer’s disease risk? J Radiat Res 53: 815-822.
- World Health Organization (2016) Electromagnetic fields and public health. World Health Organization, Geneva, Switzerland.
- Ahlbom IC, Cardis E, Green A, Linet M, Savitz D, et al. (2001) Review of the epidemiologic literature on EMF and Health. Environ. Health Perspect 109: 911-933.
- García AM, Sisternas A, Hoyos SP (2008) Occupational exposure to extremely low frequency electric and magnetic fields and Alzheimer disease: a meta-analysis. Int J Epidemiol 37: 329-340.
- Sperling RA, Aisen PS, Beckett LA, Bennett DA, Craft S, et al. (2011) Toward defining the preclinical stages of Alzheimer’s disease: recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement 7: 280-92.
- Wyss-Coray T, Rogers J (2012) Inflammation in Alzheimer disease-a brief review of the basic science and clinical literature. Cold Spring Harb Perspect Med 2: 006346.
- Nunomura A, Perry G, Aliev G, Hirai K, Takeda A, et al. (2001) Oxidative damage is the earliest event in Alzheimer disease. J Neuropathol Exp Neurol 60: 759-767.
- Sobel E, Davanipour Z, Sulkava R, Erkinjuntti T, Wikstrom J, et al. (1995) Occupations with exposure to electromagnetic fields: a possible risk factor for Alzheimer’s disease. Am J Epidemiol 142: 515-524.
- Jalilian H, Teshnizi SH, Röösli M, Neghab M (2018) Occupational exposure to extremely low frequency magnetic fields and risk of Alzheimer disease: A systematic review and meta-analysis. Neurotoxicology 69: 242-252.
- Röösli M, Lörtscher M, Egger M, Pfluger D, Schreier N, et al. (2007) Mortality from neurodegenerative disease and exposure to extremely low-frequency magnetic fields: 31 years of observations on Swiss railway employees. Neuroepidemiology 28: 197-206.
- Molinari C, Stoppa I, Limardo N, Uberti F (2018) Evaluation of the Effectiveness of Protective Patches on Acupoints to Preserve the Bioenergetic Status against Magnetic Fields. Evid Based Complement Alternat Med 2018: 4732130.
- Kato-Narita EM, Nitrini R, Radanovic M (2011) Assessment of balance in mild and moderate stages of Alzheimer's disease: implications on falls and functional capacity. Arq Neuropsiquiatr 69: 202-207.
- Li M, Lyu JH, Zhang Y, Gao ML, Li WJ, et al. (2017) The clinical efficacy of reminiscence therapy in patients with mild-to-moderate Alzheimer disease: Study protocol for a randomized parallel-design controlled trial. Medicine (Baltimore) 96: 9381.
- Fritz NE, Kegelmeyer DA, Kloos AD, Linder S, Park A, et al. (2016) Motor performance differentiates individuals with Lewy body dementia, Parkinson’s and Alzheimer’s disease. Gait Posture 50: 1-7.
- Sacks B, Meyerson G, Siegel JA (2016) Epidemiology Without Biology: False Paradigms, Unfounded Assumptions, and Specious Statistics in Radiation Science (with Commentaries by Inge Schmitz-Feuerhake and Christopher Busby and a Reply by the Authors). Biol Theory 11: 69-101.
- Rola R, Raber J, Rizk A, Otsuka S, VandenBerg SR, et al. (2004) Radiation-induced impairment of hippocampal neurogenesis is associated with cognitive deficits in young mice. Exp Neurol 188: 316-330.
- Maciocia G (2014) The Foundations of Chinese Medicine (3rd edn). Elsevier, Churchill Livingstone, London, UK.
Citation: Olivieri M, Molinari C, Ruga S, Nardi GM, Limardo N, et al. (2019) Evaluation of the Efficacy on Patients Suffering from Alzheimer’s Disease of Anti-Radiation Screens and Protective Patches to Preserve them from the Effects of Artificial Electromagnetic Fields and Natural Radiation. J Altern Complement Integr Med 5: 059.
Copyright: © 2016 Marina Olivieri, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
© 2026, Copyrights Herald Scholarly Open Access. All Rights Reserved!