Evidence-Based Approach and Discussion of ‘Bioceramic Resonance’ to Induce Altered States of Consciousness with Illusory Perception: Possible Application as a Complementary and Alternative Therapy
*Corresponding Author(s):
Ting-Kai LeungDepartment Of Radiology, Taoyuan General Hospital, Ministry Of Health And Welfare, Taoyuan, Taiwan, Graduate Institute Of Biomedical Materials And Tissue Engineering, College Of Biomedical Engineering, Taipei Medical University, Taipei, Taiwan, College Of Health Care And Management, Kainan University, Taoyuan, Taiwan
Tel:886 20336997213101,
Email:hk8648@tmu.edu.tw
Abstract
Background: Our previous study had shown Bioceramic Resonance (BR) induced an altered state of consciousness with illusory perception.
Methods: We designed questionnaires to assess subjective descriptions in the application of BR on mentally healthy participants to observe different types of illusory perception, which are based on previous brain stimulation research.
Results: We found that 61.3% of the participants recorded different positive illusory perceptions with a statistically significant difference. It was demonstrating different subjective descriptions of BR treatment, with different categories of acute effect of stimulation, with different ratios from low to high levels of illusory perception based on their subjective descriptions and experiences induced by BR treatment.
Conclusion: By combing these results and our previous objective data of electroencephalographic brain wave activity and the locations of brain activation during 3T functional MRI scanning, we hypothesis that the phenomenon observed in this study mimics the psychotherapeutic effects of transcranial brain stimulation, which may probably explain by induction of cerebral electrical discharge and change of synchronous neuronal activity. We discussed the possibility of complementary and alternative therapy on different psychiatric and neurological disorders.
Keywords
Altered states of consciousness; Bioceramic Resonance; Cerebral electrical discharge; Illusory perception; Transcranial brain stimulation; Synchronous neuronal activity
Abbreviations
LTP: Left Temporal Pole
LPHG: Left Parahippocampal Gyrus
LRO: Left Rolandic Operculum
LIFG: Left Inferior Frontal Gyrus
LPG: Left Precentral Gyrus
LHC: Left Hippocampus
LMFG: Left Middle Frontal Gyrus
LIS: Left Insula
LTL: Left Thalamus
Introduction
The term ‘Altered States of Consciousness (ASC) is usually applied to physiological assessment or neurological scoring, relate to the change of subject's mental condition from the baseline state. However, the definition of ASC can also apply to the operation of high-level mind–brain complex. Amongst the modes, lucid dream, hypnosis, meditation, and various hallucinatory states are also some examples of non-ordinary experiences that referred as ASC [1]. On the other hand, physiologists have recognized dozens of senses in humans, the five basic organs of perception that receive stimuli from our environment are: eyes (visual sensation), ears (auditory sensation), nose (olfactory sensation), taste (gustatory sensation) and touch (tactile sensation). In specific situations, such as electric brain stimulation may provoke human’s simple or complex sensations that similar to real basic organs of perception.
For example, Arzy S et al., had reported the phenomenon of focal electric stimulation of left temporaoparietal junction of the cerebrum that induction of specific Illusory Perceptions (IP) and was repeatable [2]. This is a misinterpretation of a real external or sensory experience and may also have been described as reception of information not gained through the recognized physical senses, but constructed by the brain [3].
Such perceptions maybe qualitatively as real as actual cognized perceptions or illusory. Furthermore, certain medical experiments indicate that different kinds of sensory phenomena could be evoked through Transcranial Brain Stimulation (TBS), such as transcranial electricity or magnetic stimulations of the brain [4,5]. Bioceramic technology involves a physical-biological application, based on the use of a bioceramic material, which has been proven to weaken hydrogen bonds and alter the characteristics of liquid water [6]. Furthermore, significant effects of bioceramic in various cell experiments, animal experiments, and human trials, particularly in the promotion of microcirculation and change of skin conductance, as well as other physiological responses have been reported and can be reproduced [7-13]. Bioceramic Resonance is the technology of combining sound waves using specific frequency beats in conjunction with our proprietary bioceramic material, which offers a new kind of clinical application of bioceramic technology [8-13], especially in improving psychologically related sleep disturbance and alleviating drug overdose withdrawal symptoms [9,10]. Using fMRI, we could demonstrate stimulation of the brain with corresponding cerebral and cerebellar areas of activation and deactivation, under the operation of BR (described below). Our previous study had also shown the phenomenon of Bioceramic Resonance (BR) induced ASC with IP [14]. In this study, we were further investigating and quantify the different levels of ASC with IP by referring to previous literature, as well as explaining the possible mechanism.
Methods
Bioceramic Resonance (BR)
The bioceramic powder [6-14] used in this study (obtained from the Bioenergy laboratory, Taoyuan, Taiwan) was composed of micro-sized particles produced from several different elemental oxides. Using 10% of fine bioceramic powder mixed with silicone rubber by the ratio of 1:10 and then produced a sheet membrane with a sponge-like density at 1.2g/cm3. The BIOCERAMIC sheet is capable of sound transmission (Figure 1a) [6-14]. BR was achieved using this material with an energy field that can be varied by sound wave frequencies [8-12]. We also used BR to produce different beats of tempo measured in beats per second (bps) (e.g. 10 bps), which helped amplify the effect of the bioceramic material. There are two characteristics of the technology of BR that include: (i) by clinical observation, we found the BR effect can fully propagate and pass through the whole length of the body (e.g. from foot to head) [12], which was proved and already put into clinical application. We had described how BR apply from posterior neck/body, the palm of bilateral hands and feet (similar to Figure 1b), and successful to affect brain function by alleviating drug withdrawal symptoms of amphetamine and hypnotic drugs [10]; (ii) Technically, the energy field is too weak to be measured directly, but the effect could only measure indirectly by the effect of in-vitro bimolecular and in-vivo measurement on a human being (such as skin conductance, corona discharge, Electroencephalographic Activity (EEG) parameter, fMRI and clinical observations) [7-10,12-13].
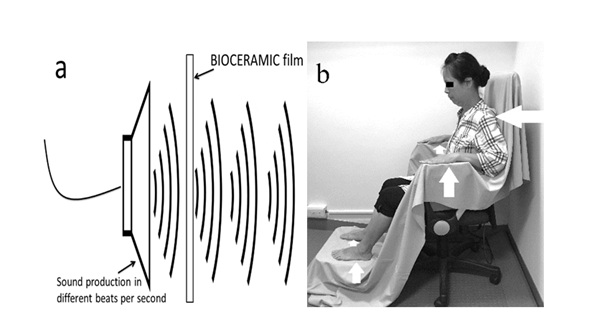 Figure 1a-b: Conceptual figure of BR is the device to produce beats of tempo sound which propagate through BIOCERAMIC film setting at 10 cycles per second with an overall output of 100 dB (1a, left): Sources of BR treatments on posterior neck/body trunk, bilateral hands and bilateral feet (white solid arrows)(1b, right).
Figure 1a-b: Conceptual figure of BR is the device to produce beats of tempo sound which propagate through BIOCERAMIC film setting at 10 cycles per second with an overall output of 100 dB (1a, left): Sources of BR treatments on posterior neck/body trunk, bilateral hands and bilateral feet (white solid arrows)(1b, right).
Safety
The effect of bioceramic material belongs to non-ionized radiation, so far, no relevant evidence of a negative effect on human health [15]. Besides, participants were received of below 100 dB of sound level and last for 20 minutes while BR treatments. This sound the pressure level is acceptable, as compared with the altitude as high as 130 dB while receiving MRI image scanning in hospital, which usually last for over 30-45 minutes [15].
Study participants
The human volunteers that participated in the clinical trials were sourced using poster advertisements placed on bulletin boards near practice waiting rooms. There were 165 adults of both sexes (female: 96; male: 69) who consented to participate in these experiments, aged between 21 to 62 years. The participants were randomly assigned to control and experimental groups. The case number of the control group were 10 participants (female: 5; male:5) who received usual sound beats set at 10 cycles per second with an output of 100 dB. The case number of the experimental group were 155 adults of both sexes (female: 91; male: 64) Participants with the minor physical disorder (such as arthritis, urolithiasis or chronic pancreatitis) could be accepted for this research, but the major mental disease is excluded. Participants were screened and none were found with neurological or psychiatric disorders or with any indications of drug abuse or sleep deprivation that warranted exclusion from the study. The study was conducted at the Taoyuan General Hospital, in the northern part of Taiwan. The study protocol was approved by the Human Subjects Ethics Committee (approval no.: TYGH106015). In our experimental model of questionnaire collection, the volunteers received indirect brain stimulation of using BR through skin conduction on posterior neck/body trunk, palms of bilateral hands, and ventral sides of bilateral feet (Figure 1b). The sound beats were set at 10 cycles per second with an output of 100 dB interested readers may refer to our published paper discussing the concept behind sound stimulation [12].
Questionnaire assessment of subjective descriptions with the bioceramic resonance system
At the beginning, volunteer participants were sat alone in the experimental room for about 5 minutes (as control condition). And then, the control group and the experimental group received the experiment a protocol using the usual sound and BR system for 20 minutes respectively. Participants were asked to pay attention and record to any change and all sensations that they may experience before and after the BR experiment. A questionnaire (Figure 2) was designed to quantify the different levels of perceptions (Q1-Q5) by referring to a previous brain stimulation research [16], that our participants experienced in their subjective response to the BR system. The participants were asked to perform self-assessment on a questionnaire with 5 different questions. Those participants who selected ‘Q1’ or ‘Q2’ on the questionnaire of BR effect, were categorized as negative of ‘ASC with IP’ (NAI) group and the ones selected ‘Q3’, ‘Q4’ and ‘Q5’ were categorized as positive of ‘ASC with IP’ (PAI) group. The participants who belong to the PAI group were further required to perform a self-assessment on an ASC with an IP chart (Table 1) according to the descriptions which most closely matched what they experienced system. The participants were asked to perform a self-assessment on a questionnaire with 5 different questions. Those participants who selected ‘Q1’ or ‘Q2’ on the questionnaire of BR effect, were categorized as negative of NAI group, and the ones selected ‘Q3’, ‘Q4’ and ‘Q5’ were categorized as positive of PAI group. The participants who belong to PAI group were further required to perform a self-assessment on ASC with PI chart (Table 1) according to the descriptions which most closely matched what they experienced. Thus, we reconfirmed and categorized groups of participants as type 1 to type 3, based on their highest level of subjective descriptions and experiences after receiving a session of BR treatment (Table 1).
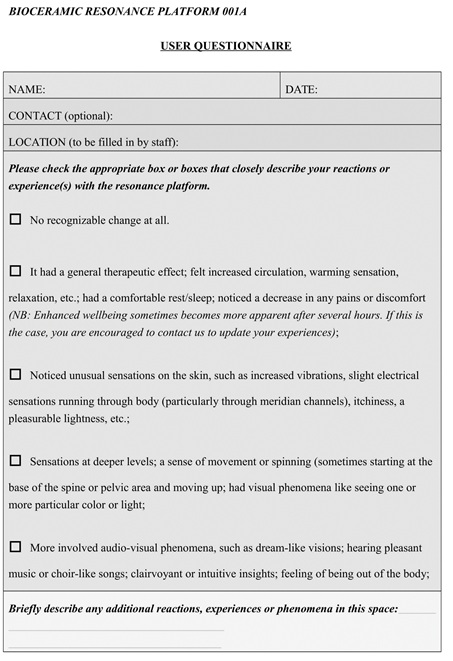
Figure 2: Questionnaire designed to quantify the different levels of perceptions (Q1-Q5).
|
Types of ASC with IP under BIOCERAMIC Resonance stimulation |
Different descriptions (reference and guideline from review study of ‘brain stimulation’ by Selimbeyoglu & Parvizi) |
|
Type 1(Q3) |
Somatosensory sensations of paresthesia in various parts of the body; Perception on the skin, such as increased vibrations, itchiness, slight electrical sensations running through surface of body (without real skin stimulation) |
|
Type 2(Q4) |
Sensations at deeper levels; a sense of movement or spinning, sometimes starting at the base of the spine or pelvic area and moving up; had visual phenomena like seeing one or more particular color or light (without real visual stimulation) |
|
Type 3(Q5) |
Déjà vu, feeling of unreality; Feeling of levitation; Auditory hallucination (e.g., hearing human voices); Feelings of being somewhere else or someone else Visual hallucinations (e.g., seeing geometric shapes, flashing lights) or seeing a face) (candidates were left alone in experimental room) |
Table 1: Subjective descriptions of different types of BR treatment, to help qualify participants’ ASC with IP.
Statistical analysis
Statistical evaluation between NAI and PAI groups were determined by ‘The Chi-Square Goodness of fit' test, the test is to compare the observed sample distribution with the expected probability distribution, to determine how well theoretical distribution fits the empirical distribution. By calculation, p-value less than 0.05* or 0.001** is considered significant or highly significant difference respectively.
Results
There were 10 questionnaires (n=10) gathered for the control using the usual sound system, we found all of the 10 participants belong to ‘Q1’ (Figure 2). This result indicates usual sound stimulation could not enhance the general therapeutic effect and ASC with IP effect. There were 155 questionnaires (n=155) gathered for the experiments using the BR system, we found 50 and 10 participants belong to ‘Q1’ and ‘Q2’ respectively (NAI group) (Figures 2 & 3). There were 61.3% of participants (Q3’, Q4’ and ‘Q5’) categorized as PAI group (figure 2 & 3). By using ‘The Chi-Square Goodness of fit’ test, there is a highly significant statistical difference between the groups of NAI and PAI (as p<0.001**). Since our participants were all excluded from past history of major mental disease of neurological or psychiatric disorders drug abuse and sleep deprivation, this statistical result leaves us a question on how to explain BR can evoke a high percentage of ASC with IP effect on mentally healthy participants. Besides, amongst the PAI group (‘Q3’, ‘Q4’ and ‘Q5’) (Figures 3 & 4), 76.84% of the PAI group were determined to be type 1(Q3) in sensory processing or perception. There were 13.68% of the PAI group belonged to type 2 (Q4) (Deeper sensorial illusions), and 9.47% were evaluated as the unusual and distinct ASC with IP of type 3 candidates. Type 3 (Q5) category is included complex visual hallucinations, auditory hallucination, the rotatory sensation of the body parts, the illusion of body parts moving, mental relaxation and feeling empty, feeling of unreality, feeling of levitation, and crying uncontrollably without the sensation of sadness. The corresponding incidence of different descriptions is shown in table 2. Since each participant may report more than one description of ASC with IP, the incidence rate is more than the number of participants (Table 2).
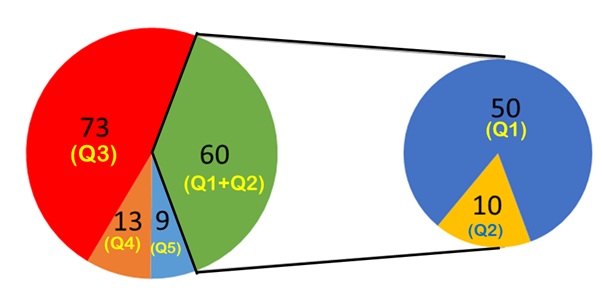 Figure 3: shows different case number of participants belongs to ‘Q1-Q5’ of BR effect; left pie chart is arise from the portion of (Q1+Q2) from right ‘Q1-Q5’ of BR effect.
Figure 3: shows different case number of participants belongs to ‘Q1-Q5’ of BR effect; left pie chart is arise from the portion of (Q1+Q2) from right ‘Q1-Q5’ of BR effect.
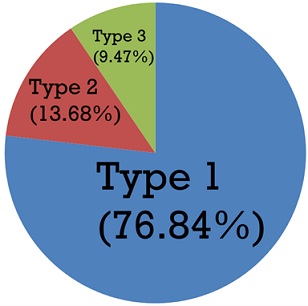 Figure 4: Ratio from low to high levels (type 1-3) of ASC with IP, based on their subjective descriptions and experiences induced by BR treatment.
Figure 4: Ratio from low to high levels (type 1-3) of ASC with IP, based on their subjective descriptions and experiences induced by BR treatment.
|
Different perceptions induced by BR |
Different descriptions |
Categories of acute effect of brain stimulation |
Brain location(s) |
Incidence |
|
Type 1: Sensorial illusions
|
Regional pain (non BR dependent site) |
Sensory |
Temporoinsular junction |
36 |
|
Regional paraesthesia; Body tingling |
Sensory |
Posterior cingulate cortex;
Inferior parietal lobe |
25 |
|
|
Pulsate on skin |
Sensory |
Frontal gyrus |
11 |
|
|
Itching |
Sensory |
Frontal gyrus |
15 |
|
|
Flow sensation along specific route of skin |
Sensory |
Frontal gyrus |
25 |
|
|
Effect on Gastrointestinal tract: Change of bowel habit; Evoke epigastric sensation or hunger; Hiccup |
Autonomic |
Insula;
Orbitofrontal and ventromedial frontal cortex;
Anterior cingulate cortex |
11 |
|
|
Type 2: Deeper sensorial illusions
|
Somatosensory sensations (e.g., warmth or paresthesia) in various parts of the body or along specific route deep inside body
|
Sensory |
Insula |
14 |
|
Visual sensations (e.g., seeing simple patterns, white or black spots or colors) |
Sensory |
Temporal pole/gyrus;
Striate cortex;
Peristriate cortex;
Superior occipital gyrus;
Parietooccipital junction
|
13
|
|
|
Type 3: Delusion of unreality and unusualness
|
Complex visual hallucinations (e.g., seeing a face or people) |
Sensory |
Temporal pole/gyrus;
Temporooccipital junction |
4 |
|
Auditory hallucination (e.g., hearing human voices) |
Sensory |
Hippocampus;
Temporooccipital junction |
4 |
|
|
Rotatory sensation of the body parts(eg. head); Illusion of body parts moving |
Sensory; Motor |
Temporal pole/gyrus;
Dorsomedial parietal and precuneus;
Supplementary motor area of frontal lobe;
Motor area of frontal lobe;
Cingulate cortex
|
5 |
|
|
Mental relax and feeling empty; feeling of unreality; |
Cognitive; insula |
Parahippocampal region of temporal lobe |
2 |
|
|
Feeling of levitation. |
Sensory |
Dorsomedial parietal and precuneus of parietal lobe |
3 |
|
|
Crying uncontrollably without sensation of sadness |
Motor; Emotional |
Internal capsule;
Subthalamic nucleus |
2 |
Table 2: Incidence of different subjective descriptions of BR treatment (reference and guideline from review study of ‘brain stimulation’ by Selimbeyoglu & Parvizi).
Discussion
In this study with BR treatments, as high as 61.3% proportion of the participants had experienced different levels of positive ASC with IP. By literature review, we found a cognitive neuroscientific study on hallucinations is not restricted to the domain of psychiatry and may not necessarily indicate a mental disorder [17]. The external effect of DBS of electricity or magnetism may also provoke hallucination. Herein, we reviewed publications on TBS that could induce an ASC with IP. There were previous studies of quantitative measurements on their effects. In a common procedure for such surgical stimulation, the median currents from the inserted electrodes are about 1.0 - 2.0 milliampere (mA), 2 to 12 voltage (V), with duration of about 1-5 seconds (s) and with biphasic pulses at 50 Hz. This brain stimulation was found to provide equivalent to about 10% of all neurons in the cortices of the hemisphere involved [18-20]. Different intensities of magnetic field stimulation on the outer cortex of the brain that produce anomalous cognitive experiences are found to be intensity-dependent. The periods of response to different intensities from 1-2 tesla to 1000nT, which provoke an ‘instant’ effect, a ‘soon after application’ effect, or a ‘latent’ effect [17-20]. There was a previous review study [16] that reported subjective experiential phenomena and behavioral changes in patients during deep surgical temporal lobe stimulation by electrodes and by volunteers exposed to weak magnetic fields applied externally across the temporoparietal lobes. Both sources of experiences are congruent with electrical stimulation of the cerebral cortex or sub cortical nuclei in awake and conscious human participants [16,18-20]. It was reported that magnetic stimulation of the brain could provoke changes in EEG. Moreover, a simple form of the pulsed magnetic field applied to the brain could result in brief bursts of brain waves measured by EEG [18-20]. A previous study using echo-planar imaging of 3-Tesla MRI with a pulsed sequence of the Blood-Oxygenation-Level-Dependent (BOLD), was measured for signal changes in cortical and subcortical motor regions during TBS of repetitive magnetic stimulation. It was found that the cortical effects of TBS may not be localized to the site of stimulation but spread out to distant areas. They reflect the capability of TBS to target both local and distant brain regions as tightly connected constituents of a cortical and subcortical network [21]. Another study using functional-MRI guided TBS to provoke stimulation of left superior temporal sulcus, which affects the perceptual phenomenon of the McGurk effect [22]. McGurk effect is a perceptual phenomenon of interaction between hearing and vision in speech perception, which is an illusion that occurs when the auditory component of one sound is paired with the visual component of another sound, leading to the ‘perceptual illusion’ of a third sound that is not available [22-23].
We previously showed how BR can transiently alter brain wave activity in a specific spectrum with statistical significance [9]. We also used 3T-fMRI on eight participants without (control group) for 5 minutes and with BR effect (experimental group) for another 5 minutes. Figure 5 shows the result of the BR effect under BOLD fMRI on different participants, the locations of brain activation including left temporal pole, left parahippocampal gyrus, left rolandic operculum, left inferior frontal gyrus, left precentral gyrus, left hippocampus, left middle frontal gyrus and left thalamus. Based on this result, we compared the neuroanatomical location of direct brain stimulation to the corresponding ASC with IP (Table 3) [16]. By comparison, we found some common forms of experiences evoked using BR stimulation that mimics electrical brain stimulation are the subjective descriptions of ‘deeper sensorial illusions’ and ‘delusion of unreality and unusualness’. The common descriptions are including auditory illusions, visual hallucinations, somatosensory sensations (e.g., warmth or paresthesia) in various parts of the body, the rotatory sensation of the body parts (eg. head), the illusion of body parts moving, urge to cry, and feeling of unreality, etc (e.g., locomotion, eye and head-turning, body swinging, olfactory sensation, and thrusting). The locations of brain activation explored by both BR and TBS including the temporal pole, parahippocampal gyrus, inferior frontal gyrus, hippocampus, middle frontal gyrus, insula, and thalamus [16,21-22]. To explain the phenomenon of ASC with IP induced by BR, some hypotheses have been suggested to explain, for example, the genesis of visual hallucinations. They could be categorized as: psychophysiological (i.e., as a disturbance of brain structure), psychobiochemical (as a disturbance of neurotransmitters), and psychodynamic (as an emergence of the unconscious into consciousness) [24]. Visual or other hallucinations caused by the effect on cerebral electrical discharge, change of synchronous neuronal activity of the brain, or induction of seizure episode have been described and could be induced by TBS [24-26]. As a method of the complementary and alternative therapeutic method, the possible risk of TBS to induce different hallucination associate with seizure may limit its wide application [27,28]. In the case of the BR effect, there is no single case seizure induction, collected. Together with our previous reports of BR effects on the elevation of specific EEG spectrum and cerebral tissue activations of fMRI, we suggest the phenomenon of BR inducing ASC with IP could also be explained by the similar mechanism of the effects on cerebral electrical discharge and change of synchronous neuronal activity of the brain. Up to now, the clinical application of TBS on different psychiatric and neurological disorders have shown good results on depression, schizophrenia anxiety disorders, obsessive-compulsive disorder, substance or food craving, stroke, Alzheimer's disease and different movement disorders [29,30]. Some of these clinical applications had also reported in our previous reports [9-11,13].
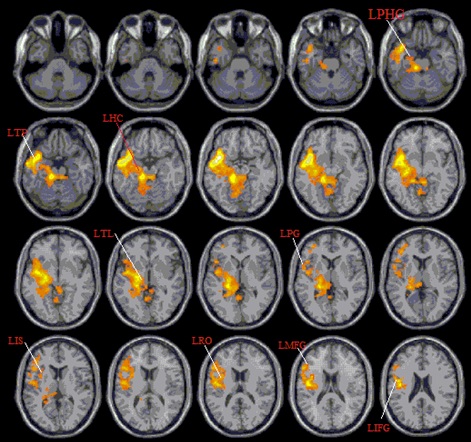 Figure 5: It shows participants received fMRI of 5 minutes without (control group) and another 5 minutes with BR effect (experimental group). Activation m aps depicting the effects of BR (experimental - control) on the areas of brain where the contrasts overlap is shown in orange and yellow.
Figure 5: It shows participants received fMRI of 5 minutes without (control group) and another 5 minutes with BR effect (experimental group). Activation m aps depicting the effects of BR (experimental - control) on the areas of brain where the contrasts overlap is shown in orange and yellow.
|
Activation of Brain location by BR detected by fMRI |
Brodmann Area |
Acute effect of electrical stimulation on sensory, motor, autonomic, emotional or cognitive effects (review study by Selimbeyoglu&Parvizi, 2010) [16]
|
|
Temporal pole |
38 |
Auditory hallucination (e.g., hearing human voices), auditory illusions, visual hallucinations related to past experiences, or-alimentary automatisms, fear, sadness or happiness
|
|
Para-hippocampal gyrus |
28, 34, 35, 36 |
Olfactory sensations, automatisms (e.g., chewing), nonsensical speech, mirth, feeling of unreality or memory recall (remembering past experience) |
|
Rolandico-perculum |
Nil |
Not mentioned |
|
Frontal gyrus |
44,45 |
Oro-alimentary automatisms, speech arrest, impaired reading prose and recitation of lyrics and singing or writing |
|
Precentral gyrus |
Nil |
Not mentioned |
|
Hippocampus |
NIL |
Auditory hallucinations (e.g., hearing “water dripping”, “hammer and nail”, voices), gustatory hallucinations, gestural or simple movements, change in facial expression or voice tone, oro-alimentary automatisms, urge to cry, anxious o happy |
|
Middle frontal gyrus |
8, 10, 46 |
Motor response (e.g., locomotion, eye and head turning, body swinging and thrusting), speech arrest or acalculia |
|
Insula |
13, 14, 15, 16 |
Unpleasant sensation of suffocation, bilateral or ipsilateral noxious (e.g., burning, stinging, and electrical shock) sensation, somatosensory sensations (e.g., warmth or paresthesia) in various parts of the body, olfactory sensation, gustatory sensation, auditory symptoms, viscero-sensory responses with or without pain, epigastric sensations, vestibular responses (e.g., vertigo), automatisms, dysarthria speech or speech arrest, nausea, sensation of unreality, fear or anxiety |
|
Thalamus |
Nil |
Disruption in verbal/nonverbal memory processing, misnaming and omissions in language tasks, disruption in verbal/nonverbal memory processing or misnaming and omissions in language tasks |
Table 3: Base on our previous fMRI finding of BR stimulation provoke neuroanatomical location, compare with the direct brain stimulation and ASC with IP.
Study Limitations
The major limitations of this study are: (i) Because of limitation on funding resource, we only allowed 10 participants assigned to the control group in this study. (ii) Our results are based on subjective perceptions of different candidates; (iii) the lack of objective detecting device for data collection; and (iv) The descriptions of their perceptions were not standardized and were variable; this was because of their different educational backgrounds.
Conclusion
As far as we know, this is a pioneer study of using a considerable non-invasive method that resulted in a high proportion of the participants with inductions of ASC with IP. By article review, we found a high degree of similarity between DBS and BR treatment reported with positive EEG findings and locations of brain activation depicted by fMRI. We suggested that the possible explanation of the cause-and-effect relationship of ASC with IP provoked by both DBS and BR, are induction of cerebral electrical discharge and change of synchronous neuronal activity. Since BR provide similar effects of TBS, with additional advantages of noninvasive and convenience of using, we expect more application on psychiatric and neurological disorders. It is worthy of further investigation, and to explore more of the underlying mechanism.
Acknowledgement
This study was supported by a grant (MOHW109-HSO-M-211-000001) from Ministry of Health and Welfare, Taiwan. Authors also express grateful to Prof. Ming-Tse Lin and Dr. Mimmo Gasberri on the contributions to this study.
Conflict of Interest
The authors declare no conflict of interest, including any financial, personal, or other relationships with other people or organizations that could inappropriately influence their work.
Reference
- Móró L (2010) Hallucinatory Altered States of Consciousness. Phenomenol Cogn Sci 9: 241-252.
- Arzy S, Seeck M, Ortigue S, Spinelli L, Blanke O (2010) Induction of an illusory shadow person. Nature 443: 287.
- Rouder JN, Morey RD, Province JM (2010) A Bayes factor meta-analysis of recent extrasensory perception experiments: comment on Storm, Tressoldi, and Di Risio. Psychol Bull 139: 241-247.
- Mégevand P, Groppe DM, Goldfinger MS, Hwang ST, Kingsley PB, et al. (2014) Seeing scenes: topographic visual hallucinations evoked by direct electrical stimulation of the parahippocampal place area. J Neurosci 34: 5399-5405.
- Schutter DJ, Kammers MP, Enter D, van Honk J (2006) A case of illusory own-body perceptions after transcranial magnetic stimulation of the cerebellum. Cerebellum 5: 238-240.
- Leung TK, Lin SL, Chan WP (2014) The influence of ceramic far-Infrared ray (cFIR) irradiation on water hydrogen bonding and its related chemo-physical properties. Hydrol Current Res 5: 174.
- Leung TK (2015) In vitro and in vivo studies of biological effects of BIOCERAMIC (material of emitting high performance far-infrared ray) Irradiation. Chin J Phys 58: 147-155.
- Zhang L, Chan P, Liu ZM, Gasbarri M, Lin MT, et al. (2016) Evaluation of reflexology by "Bioceramic Resonance" operation producing weak force field during simultaneous acupoint stimulation of urinary bladderpoint on subject's ear resulting in electric current change on urinary bladder reflex point on subject's hands, and related new research finding. Acupunct Electrother Res 41: 207-224.
- Zhang L, Chan P, Liu ZM, Tseng YL, Chen CW, et al. (2017) A technology developed from concept of acupuncture and meridian system, the clinical effect of BIOCERAMIC Resonance on psychological related sleep disturbance with findings on questionnaire, EEG and fMRI. J Trad Complem Med J Tradit Complement Med 8: 289-296.
- Leung TK, Lee CM, Gasbarri M, Chen YC (2019) Base on concept of traditional Chinese medicine: experimental studies on efficacy of BIOCERAMIC Resonance to alleviate drug withdrawal symptoms. J Trad Complem Med 10: 95-103.
- Leung TK, Yang TS, Lin RF, Tsai DM, Chou CM (2020) Evaluate clinical efficacy of bioceramic technology on psychopathically related spasmodic torticollis using motion measurements, computerized analysis of facial emotions and speech signal features. Biomed Eng Appl Basis 32: 2050021.
- Leung TK, Lee PT (2015) Bioceramic resonance effect on meridian channels: a pilot study. Evid Based Complement Alternat Med 2015: 769546.
- Zhang L, Chan P, Liu ZM, Hwang LL, Lin KC, et al. (2016) The effect of Photoluminescence of BIOCERAMIC (PLB) irradiation on Middle Cerebral Arterial occlusion (MCAO) in Rats. Evid Based Complement Alternat Med 2016: 7230962.
- Leung TK (2020) Bioceramic resonance induced extrasensory perception or altered state of consciousness: A pilot study of Taiwan. Chula Med J 64: 291-298.
- Foster JR, Hall DA, Summerfield AQ, Palmer AR, Bowtell RW (2000) Sound-level measurements and calculations of safe noise dosage during EPI at 3 T. J MagnReson Imaging 12: 157-63.
- Selimbeyoglu A, Parvizi J (2010) Electrical stimulation of the human brain: perceptual and behavioral phenomena reported in the old and new literature. Front Hum Neurosci 4: 46.
- Braithwaite JJ (2010) Neuromagnetic Effects on Anomalous Cognitive Experiences a A Critical Appraisal of the Evidence for Induced Sensed presence and Haunt?type Neuro Quantology 8: 517?530.
- Braithwaite JJ (2004) Magnetic Variances Associated with Haunt-type’ Experiences: A Comparison Using Time-Synchronised Baseline Measurements. European Journal of Parapsychology 19: 3-28.
- Braithwaite JJ (2008) Putting magnetism in its place: a critical examination of the weak-intensity magnetic field account for anomalous haunt-type experiences. Journal of the Society for Psychical Research 72: 890.
- Braithwaite JJ (2010) Neuromagnetic effects on anomalous cognitive experiences a critical appraisal of the evidence for induced sensed presence and Haunt?type Neuro Quantology 8: 517?530.
- Bestmann S, Baudewig J, Siebner HR, Rothwell JC, Frahm J (2004) Functional MRI of the immediate impact of transcranial magnetic stimulation on cortical and subcortical motor circuits. Eur J Neurosci 19: 1950-1962.
- Beauchamp MS, Nath AR, Pasalar S (2010) fMRI-Guided transcranial magnetic stimulation reveals that the superior temporal sulcus is a cortical locus of the McGurk effect. J Neurosci 30: 2414-2417.
- Nath AR, Beauchamp MS (2012) A neural basis for interindividual differences in the McGurk effect, a multisensory speech illusion. NeuroImage 59: 781-
- Teeple RC, Caplan JP, Stern TA (2009) Visual hallucinations: differential diagnosis and treatment. Prim Care Companion J Clin Psychiatry 11: 26-32.
- Erickson TC (1940) Spread of the epileptic discharge: an experimental study of the after-discharge induced by electrical stimulation of the cerebral cortex. Arch Neurol Psychiatry 43: 429-452.
- Fox JE, Bikson M, Jefferys JG (2004) Tissue resistance changes and the profile of synchronized neuronal activity during ictal events in the low-calcium model of epilepsy. J Neurophysiol 92:181-188.
- Cogné M, Gil-Jardiné C, Joseph PA, Guehl D, Glize B (2017) Seizure induced by repetitive transcranial magnetic stimulation for central pain: Adapted guidelines for post-stroke patients. Brain Stimul 10: 862-864.
- Cullen KR, Jasberg S, Nelson B, Klimes-Dougan B, Lim KO, et al. (2016) Seizure Induced by Deep Transcranial Magnetic Stimulation in an Adolescent with Depression. J Child Adolesc Psychopharmacol 26: 637-641.
- Burke MJ, Fried PJ, Pascual-Leone A (2019) Transcranial magnetic stimulation: Neurophysiological and clinical applications. Handb Clin Neurol 163: 73-92.
- Liu A, Vöröslakos M, Kronberg G, Henin S, Krause MR, et al. (2018) Immediate neurophysiological effects of transcranial electrical stimulation. Nat Commun 30: 5092.
Citation: Leung T-K, Huang Y-C (2021) Evidence-Based Approach and Discussion of ‘Bioceramic Resonance’ to Induce Altered States of Consciousness with Illusory Perception: Possible Application as a Complementary and Alternative Therapy. J Altern Complement Integr Med 6: 147.
Copyright: © 2021 Ting-Kai Leung, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.