Feeding Aversion in Children with Neurodisability and its Assessment Using CEBQ: A Tertiary Feeding Clinic Experience
*Corresponding Author(s):
Kulshrestha RRobert Jones And Agnes Hunt Orthopaedic Hospital Nhs Trust, Gobowen, Oswestry, United Kingdom
Tel:+44 1691404378,
Email:richakulshrestha@nhs.net
Abstract
Objective: The aim of this study was to define the spectrum of aversive feeding behaviours seen in children with neurodisability and assess the usefulness of Child Eating Behaviour Questionnaire (CEBQ) to systemically delineate eating behaviours amongst these children.
Methods: This study was done in two phases. In phase one 38 case notes of patients attending the multidisciplinary feeding clinic were analyzed retrospectively for a period of six months. The details of description of their feeding problems, use of antireflux medications and gastrostomy were recorded. In phase two we prospectively used the CEBQ assessment tool on 16 patients showing aversion to food and feeding. Mean sub-domain scores of CEBQ were compared to population norms.
Results: In phase one 50% (19/38) patients had feeding difficulties unrelated to oropharyngeal structural or motor problems. The behavioural feeding problems were described as aversion to food and feeding, selective eating, drinking excess fluids, poor oral intake, dislike for solids, disinterest in feeding, slow feeding and aversion for fluids. In phase two 16 patients with aversion to food or feeding and other such behaviours were assessed using CEBQ. Significant group differences in mean CEBQ sub domain scores compared to population norms were noted for food responsiveness (mean CEBQ score 1.75 vs. population mean 2.20), desire to drink (1.92 vs. 2.60), emotional overeating (0.78 vs. 1.90), satiety response (2.5 vs. 3) and enjoyment of food (2.8 vs. 3.5). Subdomain scores were reflective of non-rewarding experience of feeding in this group.
INTRODUCTION
Background
AIM
The aim of this study was to define the spectrum of aversive feeding behaviours seen in children with neurodisability and assess the usefulness of Child Eating Behaviour Questionnaire (CEBQ) to systemically delineate eating behaviours amongst these children.
METHOD
This study was conducted in multidisciplinary tertiary gastroenterology clinic. The team consisted of gastroenterologist, neurologist, speech and language therapist and dietician. In phase one of the study case notes for a period of six months were retrospectively reviewed. Feeding behaviours of all children seen in clinic were reviewed in the context of diagnosis and clinical examination. Patients were divided into two groups: with and without aversive feeding behaviours. Feeding behaviors of the former group were described. Use of anti reflux treatment and gastrostomy was compared between the two groups.
Phase two of this study was done prospectively. Children attending the clinic who were showing aversive feeding behaviors were assessed by using CEBQ completed by the parents. Patients with oromotor or structural abnormality were excluded from this assessment. CEBQ is a validated tool for assessing eight eating styles in children [14]. It is a parent rated questionnaire about rewarding (like food responsiveness, enjoyment of food, emotional overeating and desire to drink) and aversive (like slowness in eating, satiety response, fussiness and emotional under eating) feeding styles. It has 35 items with a score of 1-5. The results of all domains of the questionnaire were analyzed using Microsoft excel and scores compared to the normal population. This study was approved by the audit department for baseline service evaluation. Formal ethical approval was not obtained.
RESULTS
Phase one
| Group 1: Children with feeding aversion | |||
| Patient | Diagnosis | Comorbidity | Feeding difficulties unexplained by oromotor difficulties |
| 1 | Russel silver syndrome | Poor growth | Not interested in voluntary feeding |
| 2 | Russell silver variant | - | Not interested in feeding |
| 3 | Russell Silver Syndrome | - | Aversive feeding behaviour |
| 4 | Congenital CMV infection | Bilateral hearing loss | Aversion to feeding |
| 5 | Expreterm | Chronic lung disease, atrial septal defect | Slow to feed |
| 6 | Expreterm | - | Not interested in feeding |
| 7 | Expreterm | - | Aversion to feeding |
| 8 | Expreterm | - | Selective eating |
| 9 | Expreterm, maternal parvovirus infection | - | Drinks excess of fluids |
| 10 | Expreterm | Epilepsy, visual impairment | Selective eating |
| 11 | Developmental delay | Epilepsy, swallowing difficulty | Aversion for fluids |
| 12 | Developmental delay | - | Reluctant to try solids |
| 13 | Developmental delay, post extradural haematoma evacuation | Constipation | Aversion to feeding |
| 14 | Repaired encepahlocele | Developmental delay, VP shunt | Not like solids |
| 15 | Cerebral palsy | Epilepsy | Reduced oral intake |
| 16 | Cerebral palsy | Epilepsy | Aversion to feeding |
| 17 | Ataxic cerebral palsy | - | Aversion to feeding |
| 18 | Goldenhar syndrome | Oromotor dysfunction | Takes very little by mouth |
| 19 | Costello syndrome | Developmental delay | Aversion to feeding |
| Group 2: Children with oromotor difficulties | |||
| Patient | Diagnosis | Co-morbidities | Oro-motor difficulties |
| 1 | Cerebral palsy | Epilepsy | Struggle to swallow solids |
| 2 | Cerebral palsy | None | Yes |
| 3 | Chromosome 18q deletion | Eczema | Yes |
| 4 | Developmental delay | Epilepsy | Aspiration with thin fluids |
| 5 | Cerebral palsy | Epilepsy | Yes |
| 6 | Pierre Robin sequence with repaired cleft palate | None | Yes |
| 7 | Klippel Feil syndrome | Hydrocephalus | Aspiration with liquids |
| 8 | Cerebral palsy | None | Yes |
| 9 | Smith Lemli Optiz syndrome | None | Yes |
| 10 | Cerebral palsy | None | Yes |
| 11 | Cerebral palsy | Epilepsy | Yes |
| 12 | Micrognathia | None | Yes |
| 13 | Developmental delay | Epilepsy | Yes |
| 14 | Ex-preterm | Hydrocephalus and epilepsy | Yes |
| 15 | Criduchat syndrome | None | Yes |
| 16 | Hypoxic ischemic encephalopathy | None | Yes |
| 17 | Cerebral palsy | None | Yes |
| 18 | Cerebral palsy | Movement disorder | Yes |
| 19 | Cerebral palsy | Epilepsy | Yes |
Phase two
| Patient | Age in years | Sex (M: Male, F: Female) | Diagnosis | Description of feeding behaviours |
| A | 2 | M | Not recorded | Food refusal of solids, intermittently, once a month. Will still be drinking milk during these time. |
| B | 4 | M | Down's syndrome with feeding gastrostomy. Cleft lip and palate repaired. | Feeding aversion, gradually improving |
| C | 4 | M | Lissencephaly, epilepsy, visual impairment | Aversive behavior for food and feeding. |
| D | Not recorded | M | Cerebral palsy | Aversive behavior to food, gradually improving. |
| E | 8 | M | Expreterm, chronic lung disease | No signs of hunger, no oral intake |
| F | 10 | M | Leigh's syndrome | Takes long time to feed and reduced fluid intake |
| G | 8 | M | Wolf-Hirschhorn syndrome | Feeding aversion may put a banana and enjoys chocolate mousse. |
| H | 3 | F | Expreterm | Aversion to solid foods, can manage some pureed foods. |
| I | 2 | F | Cardiac rhabdomyoma and global developmental delay | Fussy eater, likes to chew on textured objects like cardboard. |
| J | 3 | F | Hypoxic ischaemic encephalopathy | Only tolerates smooth textures like pureed foods. |
| K | 4 | M | Russel Silver syndrome | Aversion to feeds only has juices and soft textured foods. |
| L | 2 | M | Aicardi Goutieres syndrome | Refusal of oral feeds |
| M | 8 | M | Unconfirmed genetic syndrome | Feeding aversion, now resolving. |
| N | 19 | M | Cerebral palsy, epilepsy, ventriculoperitoneal shunt and global developmental delay. | Refuses to eat, keeps food in mouth for long periods before swallowing. |
| O | 6 | M | Global developmental delay, tracheostomy for trachea-bronchomalacia. | Aversion to food and feeding. |
| P | 3 | F | Global developmental delay and visual impairment. | Refusal of all solid meals. |
| Mean of study group | Standard deviation | Population mean | Standard deviation | P value | |
| SR | 2.55 | 1.16 | 3.0 | 0.7 | 0.02 |
| SE | 2.61 | 1.25 | 3.0 | 0.8 | 0.07 |
| EU | 2.92 | 1.39 | 2.7 | 0.8 | 0.334 |
| FU | 2.66 | 0.8 | 3.0 | 0.8 | 0.107 |
| FR | 1.75 | 0.85 | 2.2 | 0.7 | 0.017 |
| EF | 2.87 | 1.16 | 3.5 | 0.8 | 0.005 |
| DD | 1.92 | 1.02 | 2.6 | 1.1 | 0.019 |
| EO | 0.78 | 0.74 | 1.9 | 1.9 | 0.001 |
Table 3: Results of CEBQ, mean of study in each subdomain compared with the population mean.
SR: Satiety Response; SE: Slowness of Eating; EU: Emotional Undereating;
FU: Fussiness; FR: Food Responsiveness; EF: Enjoyment of Food;
DD: Desire to Drink; EO: Emotional Overeating
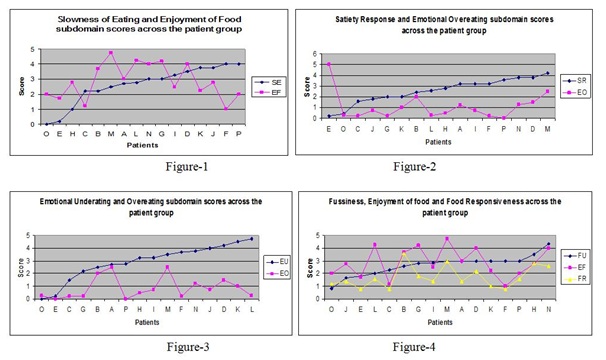 Figure 1-4: Scores of each subdomain are compared between the rewarding and aversive behaviours.
Figure 1-4: Scores of each subdomain are compared between the rewarding and aversive behaviours.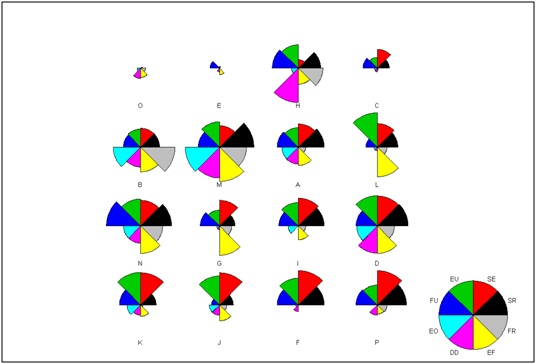 Figure 5: Stars plot of patient group, upper and lower half of the plot represents undereating and overeating scores respectively.
Figure 5: Stars plot of patient group, upper and lower half of the plot represents undereating and overeating scores respectively.DISCUSSION
Our clinical experience at a tertiary hospital feeding clinic for children with neurodevelopmental conditions suggests that children who are labelled as having "feeding aversion" can show a spectrum of behaviours like some had sensory aversion to food and feeding whereas others showed lack of food seeking. In our study we have described the spectrum of these behaviours. Irrespective of the behavior phenotype management was with multidisciplinary approach with support of dietician, speech and language therapist and gastroenterologist. The burden of care is high amongst these patients as 47% patients needed gastrostomy for supporting calorie and fluid intake.
The intrinsic component to the feeding behaviour is not always recognized in these children characterized by undereating. There may be fruitless attempts at identifying a structural abnormality, ascription of the problem to normal structural variants (tongue-tie), or to poor parenting. There is little research to describe in detail the patterns of deficient eating seen in these children with neurodevelopmental disorders. This is in marked contrast to the well-studied overeating behavioural phenotype characteristic of Prader-Willi syndrome, which is often taken as a model of intrinsic appetite control and obesity in normal population [15]. In addition there is little controlled research to evaluate interventions, which can partly be due to the lack of consistency amongst different workers, from different professional disciplines, in use of terminology and outcome measures. Speech and language therapist observation is essential in all these children but it is not readily quantified or can be used in large scale studies and remains subjective.
Different assessment tools are developed like behaviour assessment procedure [9], semi structured interviews of parents and video tape of lunch times [16], Child Eating Behaviour Inventory (CEBI) [17], Dutch Eating Behaviour Questionnaire [18] and CEBQ [14]. There are more research based tests for classifying children further although not used for clinical purposes such as 6-n-propylthiouracil (PROP) testing of supertasters, fungiform papillae counting [19,20]. As none of the tools capture the entire spectrum of feeding problem "multidimensional approach" to assessment taken by Archer and Szatman 1990 [21] in a child with "food aversion" need to be considered. This includes parental report, excluding gastro-oesophageal reflux, video fluoroscopy, and speech and language therapy assessment. We used CEBQ which captures feeding styles seen in our practice essentially a tool, which with other measures, would contribute for multidimensional assessment of this cohort of children with feeding aversion.
CEBQ has 35 items and was easy to complete in the clinic setting and only mean of 6 items remained unanswered. Amongst the rewarding eating styles of emotional overeating, desire to drink, food responsiveness and enjoyment of food the scores of study cohort were significantly low. This reinforces our observation that for our study population feeding is not identified as a rewarding experience. CEBQ scores add objectivity to this observation but also identify the subdomains where the interventions can be targeted and the response can be monitored. It was not possible to cluster patients into separate groups based on scores across subdomains. Three patients B, D and M who had already shown clinical improvement did not reflect in their subdomain scores and similarly patient E with no sign of hunger had comparable scores to others. This could be attributed to the complexity of underlying medical diagnosis, previous interventions and the heterogeneity of motor, sensory, cognitive and behaviour co-morbidities which all impact on feeding. A cross sectional view of this study is the limiting factor that did not demonstrate correlation with the clinical phenotype.
Our study has been helpful in showing the spectrum of aversive feeding behaviours and CEBQ can have a potential role in multidimensional assessment of feeding aversion amongst children with neurodisability. Its role in longitudinal follow up and response to strategies is yet to be proven.
CONCLUSION
This study identifies that feeding difficulties not related to oropharyngeal structural or motor impairment can be complex to assess and manage needing feeding gastrostomy. CEBQ has affirmed non-rewarding experience of feeding in this group and with its limitations can be helpful assessment of feeding aversion.
CONFLICT OF INTEREST
The authors declare no conflict of interest.
REFERENCES
- Rudolph CD (1994) Feeding disorders in infants and children. J Pediatr 125: 116-124.
- Stevenson RD (1995) Feeding and nutrition in children with developmental disabilities. Pediatr Ann 24: 255-260.
- Palmer S, Horn S (1978) Feeding problems in children. In: Palmer S, Ekvall S (eds.). Pediatric Nutrition in Developmental Disorders. Charles C Thomas Publisher, USA. Pg no: 613.
- Perske R, Clifton A, McClean B M, Stein JI (1977). Mealtimes for severely and profoundly handicapped persons: New concepts and attitudes. University Park Press, Baltimore, US, 142.
- Burklow KA, Phelps AN, Schultz JR, McConnell K, Rudolph C (1998). Classifying complex pediatric feeding disorders. J Pediatr Gastroenterol Nutr 27: 143-147.
- Linscheid TR (1992) Eating problems in children. In: Walker CE, Roberts MC (eds.). Handbook of clinical child psychology. J Wiley & Sons, New York, USA. Pg no: 1145.
- Riordan MM, Iwata BA, Finney JW, Wohl MK, Stanley AE (1984) Behavioural assessment and treatment of chronic food refusal in handicapped children. J Appl Behav Anal 17: 327-341.
- Field D, Garland M, Williams K (2003) Correlates of specific childhood feeding problems. J Paediatr Child Health 39: 299-304.
- Munk DD, Repp AC (1994) Behavioural assessment of feeding problems of individuals with severe disabilities. J Appl Behav Anal 27: 241-250.
- Marjorie MP, Melvin BH (1993) Assessment and treatment of sensory- versus motor- based feeding problems in very young children. Infants & Young Children 6: 67-73.
- Chatoor I, Eagan J, Getson P, Menvielle E, O'Donnell R (1988) Mother-infant interactions in infantile anorexia nervosa. J Am Acad Child Adolesc Psychiatry 27: 535-540.
- Pliner P, Hobden K (1992) Development of a scale to measure the trait of food neophobia in humans. Appetite 19: 105-120.
- Giuseppe S (2002) Effects of conditioned food aversions on nutrional behaviour in humans. Send toNutr Neurosci 5: 158-188.
- Wardle J, Guthrrie AC, Sanderson S, Rapoport L (2001) Development of children's eating behaviour questionnaire. J Child Psychol Psychiatry 42: 963-970.
- Sarimski K (1996) Specific eating and sleeping problems in Prader-Willi and Williams-Beuren syndrome. Child Care Health Dev 22: 143-150.
- Douglas J, Harris B (2001) Description and evaluation of a day-centre based feeding behavioural programme for young children and their parents. Clinical Child Psychology and Psychiatry 6: 241-256.
- Archer LA, Rosenbaum PL, Streiner DL (1991) The children's eating behavior inventory: reliability and validity results. J Pediatr Psychol 16: 629-642.
- Braet C, Van Strien T (1997) Assessment of emotional, externally induced and restrained eating behaviour in nine to twelve-year-old obese and non-obese children. Behav Res Ther 35: 863-873.
- Delwiche JF, Buletic Z, Breslin PA (2001) Relationship of papillae number to bitter intensity of quinine and PROP within and between individuals. Physiol Behav 74: 329-337.
- Tepper B, Nurse R (1998) PROP taster status is related to fat perception and preference. Ann N Y Acad Sci 855: 802-804.
- Archer LA, Szatman P (1990) Assessment and treatment of food aversion in a four year old boy: a multidimensional approach. Can J Psychiatry 35: 501-505.
Citation: Kulshrestha R, Dalzell M, Kumar R (2018) Feeding Aversion in Children with Neurodisability and its Assessment Using CEBQ: A Tertiary Feeding Clinic Experience. J Gastroenterol Hepatology Res 3: 017.
Copyright: © 2018 Kulshrestha R, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.