Growth Hormone Secreting Ectopic Pituitary Adenoma: Case Report and Literature Review
*Corresponding Author(s):
Houssein DarwishDepartment Of Neurosurgery, American University Of Beirut Medical Center, Beirut, Lebanon
Tel:+961 3628753,
Email:hd17@aub.edu.lb
Marwan Najjar
Department Of Neurosurgery, American University Of Beirut Medical Center, Beirut, Lebanon
Tel:+961 3043704,
Email:Mn12@aub.edu.lb
Abstract
Background: Pituitary adenomas are common primary brain tumors that occur in the sella turcica where the pituitary gland resides. However, rare condition where separate hormone secreting ectopic pituitary tissue can be present elsewhere in the brain.
Case: A 68-year-old female patient presented to our institution with growth hormone secreting pituitary adenoma. MRI showed normal sellar pituitary gland. A lesion was later identified eroding the sella, sphenoid bone, clivus, and dorsum sellae. Histopathological studies showed growth hormone secreting pituitary tissue.
Conclusion: Hormone secreting ectopic pituitary tissue can be present elsewhere in the brain and should be suspected in any patient with abnormally high levels of pituitary hormones with normal sellar MRI images.
Introduction
Pituitary Adenomas (PA) represent 10% to 15% of all reported brain tumors, being among the most prevalent intracranial growths [1]. They are seen in 1 out of 865 to 2688 individuals [2]. Embryologically, the pouch of Rathke proliferates to form the anterior pituitary lobe, which, in turn, may abnormally replicate and grow into PA [3]. According to their size, pituitary adenomas fall under two categories. When the tumor size is 10 mm or more, PAs are called macroadenomas and they account for about 50% of all PAs, while the other half are microadenomas [4]. Another classification is based on their glandular function. About 44% of PAs are called functional PAs due to their hormonal secretion ability [5]. Normally, PA are found in the Sella Turcica (ST). A quite rare form of pituitary adenomas with roughly 100 cases documented in the literature are called EPA, or ectopic pituitary adenomas. EPA are not connected in any way to the normal pituitary gland and are always found outside the ST [6]. In previous studies, it has been shown that females are at risk of developing EPA twice as frequently as males [7,8]. A large percentage of EPA are benign, although a minority of cases can develop into malignant tumors [9]. Ectopic pituitary adenomas can produce any type of major pituitary hormones [10]. They can be GH, ACTH, PRL or TSH secreting tumors. Growth hormone secreting ectopic pituitary adenomas are extremely rare. Excessive GH secretion by sellar pituitary adenomas account for 98% of all cases. Less than 2% is secreted by NET and the rest are produced by EPAs [11]. Only 11 cases of GH-secreting ectopic pituitary adenomas have been confirmed by histopathology and reported in the literature so far [12].
In this article, we report an additional rare case of growth hormone-secreting ectopic pituitary adenoma in the sphenoid sinus with a review of the literature.
Case Description
We present the case of a 68-year-old female patient who is known to have paroxysmal atrial fibrillation who presented to our institution with acromegaly symptoms. History goes back to 5 months prior to her presentation when the patient started complaining of fatigue and shortness of breath. Investigations were done which showed paroxysmal atrial fibrillation, hyperthyroidism and cardiomyopathy. MRI brain showed a sphenoid lesion extending to the sellar floor. The patient noticed an increase in shoe size and size of her hand and fingers. On exam, wide MCP joints were apparent. Hormonal profile showed elevated IGF levels. CT sinuses, done as part of pre-op planning, showed soft tissue mass eroding the floor of the sella, sphenoid bone and clivus. There is soft tissue mass in the right aspect of the sella, measuring approximately 1.2cm and the rest of the sella is seen empty (Figure 1). There is soft tissue lesion eroding the floor of the sella, eroding the sphenoid bone, the clivus and dorsum sellae, it is measuring approximately 3.2cm in its AP diameter and 1.4cm in its supero-inferior dimension (Figure 2). Anteriorly there is erosion of the anterior wall of the sella, significant thinning of the left sphenoid sinus. Intra-op, the tumor was apparent in the sphenoid sinus and the arachnoid membrane was bulging into the sinus. A grayish friable lesion was identified. Using ring curette and suction, the lesion was smoothly suctioned and dissected in all directions. Pathology showed growth hormone secreting pituitary adenoma.
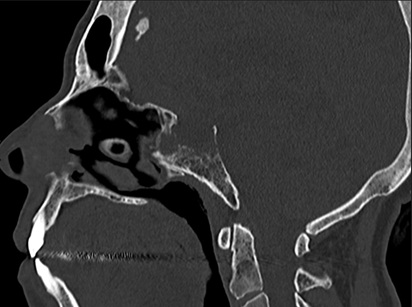 Figure 1: CT brain bone window showing soft tissue lesion eroding the floor of the sella, eroding the sphenoid bone, the clivus and dorsum sellae, it is measuring approximately 3.2cm in its AP diameter and 1.4cm in its supero-inferior dimension.
Figure 1: CT brain bone window showing soft tissue lesion eroding the floor of the sella, eroding the sphenoid bone, the clivus and dorsum sellae, it is measuring approximately 3.2cm in its AP diameter and 1.4cm in its supero-inferior dimension.
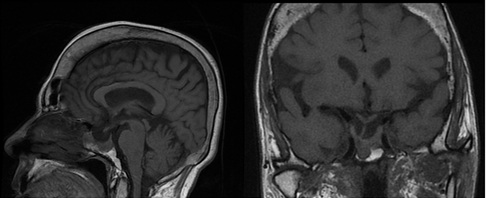 Figure 2: Soft tissue mass in the right aspect of the sella, measuring approximately 1.2cm and the rest of the sella is seen empty.
Figure 2: Soft tissue mass in the right aspect of the sella, measuring approximately 1.2cm and the rest of the sella is seen empty.
Discussion
Only a few previous studies have tackled the origin of ectopic pituitary adenomas. Normally, the main pituitary gland divides into Sellar and pharyngeal sections around the eighth week of pregnancy. A pharyngosellar pituitary is an uncommon pituitary deformity that is caused by the disruption of this division. Many individuals often have a Pharyngeal Pituitary (PhP) as part of their anatomy. However, compared to the Sellar pituitary, PhP produces pituitary hormones around 4 to 10 weeks later. Pharyngeal pituitary can manifest as extracranial pituitary adenomas originating in the nasopharynx, clivus or the sphenoid sinus. These adenomatous pituitary masses may also result from the remaining pituitary tissue fragments in the craniopharyngeal canal that is present in 0.42% of asymptomatic people [13]. Sphenoid sinus is the most common site of EPA. In the past 26 years, ectopic pituitary adenomas of the sphenoid sinus have been reported in 7 out of 15 cases that we have collected for the literature review (Table 1). The finding of a pituitary mass inside the sphenoid sinus does not necessarily indicate the presence of an ectopic pituitary adenoma. It can be explained by a tumor inside the sella eroding the sellar wall and protruding to the sinus with the dura extending downwards [12,14]. Alternatively, a diagnosis of EPA cannot be excluded if there is invasion of the Sella Turcica [15]; although most of the cases reported previously demonstrated an intact sella and dura (Table 1). In our patient, MRI imaging revealed a mass occupying the sphenoid sinus, eroding the clivus and the sellar wall. The mass was not found to be occupying the sella or protruding inferiorly into the sinus; thus, the diagnosis of ectopic pituitary adenoma was made based on the imaging and intra-op findings where part of the tumor was encountered inside the sphenoid sinus independently of the sellar pituitary. Furthermore, the patient presented to our hospital with signs of acromegaly, therefore, GH-secreting EPA was confirmed by high levels of serum IGF-1 along with the pathology results. Growth hormone secreting ectopic pituitary adenoma in the sphenoid sinus was first written about by Erdheim [16]. Through the review of literature (Table 1), we have identified 6 GH-secreting ectopic pituitary adenomas out of 15 cases reported in the past few years. Ectopic pituitary adenomas can stem from various sites including sphenoid sinus, superior orbital fissure, temporal lobe, third ventricle, and nasal cavity [17].
Literature reviews of EPA by Kepes and Fritzlen in 1964 identified a case of nonfunctional ectopic pituitary adenoma in the sphenoid sinus [18]. In 1975, Ortiz-Suarez and Erickson reported a case of ACTH-secreting EPA in the superior orbital fissure [19]. From 1909 until 1993, ectopic pituitary adenomas were most reported inside the SS [17]. 0.48% of all cases of ectopic pituitary adenomas are seen in the SS of which 25% are necrotic [17]. A case was described by Neilson and de Chadarevian in 1987 shows an ectopic pituitary adenoma in the temporal lobe [20]. Another case was identified in the third ventricle in 1990 by Kleinschmidt [21]. In 2004, a case of EPA was discovered in the cavernous sinus and reported by Mitsuya and Nakasu [22]. Ectopic pituitary adenoma in the sphenoid sinus extended to the nasal cavity through the craniopharyngeal canal was first reported by Kaushik in 2010 [23]. In addition, a case of parapharyngeal space was first documented in 2014 by Xiaofeng Wu using CT brain [10]. Despite highly developed imaging techniques, ectopic pituitary adenomas are still often misdiagnosed or diagnosed after some delay due to their rarity and complexity, therefore, can resemble many tumors of the skull base. However, EPA should always be kept in the differential diagnoses in patients with abnormally elevated levels of one of the major anterior pituitary hormones with an intact Sella turcica on MRI.
|
Author |
Age/Sex |
Associated Signs and Symptoms |
Type of EPA |
Location |
Imaging Findings |
Management |
|
Li et al. [9] |
47/F |
Hematuria Epistaxis Headache Dizziness |
ACTH-secreting |
Sphenoid sinus and clivus |
Non-contrast CT: Hypodense mass in the sphenoid sinus and clivus with intact Sella |
Surgical removal followed by radiation therapy |
|
Wu et al. [10] |
59/F |
Gradually enlarging painless lump on the neck No neurological or endocrine symptoms |
GH-secreting |
Right parapharyngeal space |
Contrast- enhanced CT: Heterogenous density mass in the carotid sheath area |
Tumor resection from the parapharyngeal space. The mass was totally removed along the vagus nerve inside the carotid sheath |
|
Ramirez et al. [11] |
45/F |
Menstrual abnormalities Feet and hands enlargement Fatigue Sleep apnea Dental spacing Acanthosis nigricans |
GH-secreting |
Sphenoid sinus |
Gadolinium enhanced T1W: Hyperintense mass in the sphenoid sinus with an intact Sellar turcica and dura |
Octreotide-LAR 20 mg for 4 months followed by surgical resection Transsphenoidal approach |
|
Appel et al. [12] |
50/F |
Generalized muscle and joints pain Headache Enlargement of face, hands and feet |
GH and PRL secreting |
clivus |
Gd-enhancing T1W: hypointense lesion on the right side of PG |
Endoscopic transsphenoidal surgery confirmed a mass inside the clivus with an intact Sellar floor, dura and PG |
|
Mitsuya et el. [22] |
55/F |
Enlargement of the hands, feet and hands |
GH-secreting |
Cavernous sinus |
Gd-enhanced T1W: Mass surrounding the right ICA in the right cavernous sinus with an intact pituitary gland |
Transsphenoidal surgery. Bromocriptine Gamma-knife surgery since bromocriptine treatment was unsuccessful |
|
Kaushik et al. [23] |
76/M |
Right upper extremity weakness |
PRL-secreting |
Sphenoid sinus |
TW1: Hypointense mass in the sphenoid sinus extending to the nasopharynx with intact Sella |
Endoscopic transsphenoidal resection |
|
Pojskic et al. [24] |
65/F |
Headache Nasal stuffiness |
ACTH-secreting |
Sphenoid sinus |
Gadolinium- enhanced T1W: heterogeneously enhancing lesion in the sphenoid sinus with intact Sellar turcica |
Transsphenoidal resection |
|
Wang et al. [25] |
66/M |
Double vision Right proptosis |
Inactive |
Spheno-orbital region |
Gadolinium- enhanced T1W: Enhancing tumor in the spheno-orbital region with intact pituitary gland inside the Sellar Turcica |
Frontotemporal craniotomy with total tumor resection |
|
Mudd et al. [26] |
78/M |
Blurry vision Leftward gaze double vision Headache |
Inactive |
Clivus |
T2W: Lytic lesion inside the clivus with central enhancement. Intact Sellar turcica |
Trans nasal endoscopic resection |
|
Ferraz-Filho et al. [27] |
30/F |
Signs and symptoms of acromegaly |
GH- secreting |
Clivus and Sphenoid Sinus |
T1/T2W: Enhancing mass in both Sphenoid sinus and clivus with an intact pituitary gland in the Sellar Turcica |
Only pharmacological (Octreotide) since the patient refused surgery |
|
Erdogan et al. [28] |
50/F |
Breathing difficulties |
TSH and PRL secreting |
Nasopharynx |
Gd-enhanced T1W: Heterogeneously enhancing mass in the nasopharynx with a normal PG in the ST |
Endoscopic surgery through the nasopharynx |
|
Bobeff et al. [29] |
64/F |
Left-sided hearing loss |
GH-secreting |
Sphenoid Sinus |
Gd-enhanced T1W: Irregularly enhancing lesion in the Sphenoid Sinus protruding to the lest Choana |
Subtotal resection via transnasal approach |
|
Hata et al. [30] |
24/F |
Double vision Unable to open her left eye Mydriasis Absence of light reflex Fixed downward and lateral ocular position on the left side No signs of endocrinological abnormalities |
ACTH-secreting |
Cavernous sinus |
T1W: well-enhancing mass in the left CS extending to the adjacent subdural space with intact PG inside the ST |
Left orbito-zygomatic approach. Total resection through the Parkinson`s triangle. |
|
Horiuchi et al. [31] |
75/M |
Double vision on the left lateral gaze |
ACTH-secreting |
Sphenoid sinus |
CT: Mass in the posterior wall of the SS with left clivus destruction |
Transsphenoidal approach. Removal of 80% of the tumor. Sellar floor, dura and PG were intact |
|
Aykel et al. [32] |
2/M |
Diminution of vision |
_ |
Persistent craniopharyngeal canal near the mamillary body |
T1W: hyperintense Lesion at the median eminence, anterior to the mammillary body |
_ |
Table 1: Ectopic pituitary adenomas of the sphenoid sinus have been reported in 15 cases.
Conclusion
Pituitary adenomas represent 10-15% of all brain tumors and are normally found in the sella turcica. However, the presence of ectopic pituitary gland tissue was reported in other areas of the brain and was found to be a separate entity from the original pituitary gland with hormone secreting capabilities. Ectopic pituitary adenomas are twice more common in females than males with a large percentage being benign adenomas. Therefore, due to the capability of such tumors to be located elsewhere, normal sellar CT or MRI scans in a patient with elevated pituitary hormones should be suspected of having ectopic pituitary adenoma.
References
- Karras CL, Abecassis IJ, Abecassis ZA, Adel JG, Bit-Ivan EN, et al. (2016) Clival ectopic pituitary adenoma mimicking a chordoma: Case report and review of the literature. Case Rep Neurol Med 2016: 8371697.
- Daly AF, Rixhon M, Adam C, Dempegioti A, Tichomirowa MA, et al. (2006) High prevalence of pituitary adenomas: A cross-sectional study in the province of Liege, Belgium. J Clin Endocrinol Metab 91: 4769-4775.
- Nishio S, Mizuno J, Barrow DL, Takei Y, Tindall GT (1987) Pituitary tumors composed of adenohypophysial adenoma and Rathke's cleft cyst elements: A clinicopathological study. Neurosurgery 21: 371-377.
- Raverot G, Jouanneau E, Trouillas J (2014) Management of endocrine disease: Clinicopathological classification and molecular markers of pituitary tumours for personalized therapeutic strategies. Eur J Endocrinol 170: 121-132.
- Askitis D, Tsitlakidis D, Müller N, Waschke A, Wolf G, et al. (2018) Complete evaluation of pituitary tumours in a single tertiary care institution. Endocrine 60: 255-262.
- Balasa AF, Chinezu R, Teleanu DM, Pascanu MI, Chinezu L, et al. (2017) Ectopic intracavernous corticotroph microadenoma: Case report of an extremely rare pathology. Rom J Morphol Embryol 58: 1447-1451.
- Anand VK, Osborne CM, Harkey HL (1993) Infiltrative clival pituitary adenoma of ectopic origin. Otolaryngol Head Neck Surg 108: 178-183.
- Tovi F, Hirsch M, Sacks M, Leiberman A (1990) Ectopic pituitary adenoma of the sphenoid sinus: Report of a case and review of the literature. Head Neck 12: 264-268.
- Li Y, Zhu J, Li Q, Zhu X, Tian J (2023) Ectopic invasive ACTH-secreting pituitary adenoma mimicking chordoma: A case report and literature review. BMC Neurol 23: 81.
- Wu X, Wen M (2015) CT finding of ectopic pituitary adenoma: Case report and review of literature. Head Neck 37: 120-124.
- Ramírez C, Hernández-Ramirez L, Espinosa-de-los-Monteros A, Franco JM, Guinto G, et al. (2013) Ectopic acromegaly due to a GH-secreting pituitary adenoma in the sphenoid sinus: A case report and review of the literature. BMC Res Notes 6: 411.
- Appel JG, Bergsneider M, Vinters H, Salamon N, Wang MB, et al. (2012) Acromegaly due to an ectopic pituitary adenoma in the clivus: Case report and review of literature. Pituitary 15: 53-56.
- Hori A, Schmidt D, Kuebber S (1999) Immunohistochemical survey of migration of human anterior pituitary cells in developmental, pathological, and clinical aspects: A review. Microsc Res Tech 46: 59-68.
- Hong J, Ding X, Wang S (2012) Coexistence of ectopic pituitary adenoma and empty sella in a patient with acromegaly: A case report and review of literature. Neurol India 60: 304.
- Langford L, Batsakis JG (1995) Pituitary gland involvement of the sinonasal tract. Ann Otol Rhinol Laryngol 104: 167-169.
- Erdheim J (1909) About a pituitary tumor of unusual location. Beitr Path Anat 46: 233-240.
- Hou L, Harshbarger T, Herrick MK, Tse V (2002) Suprasellar adrenocorticotropic hormone-secreting ectopic pituitary adenoma: Case report and literature review. Neurosurgery 50: 618-625.
- Kepes JJ, Fritzlen TJ (1964) Large invasive chromophobe adenoma with well-preserved pituitary gland; Report of a case. Neurology 14: 537-541.
- Ortiz-Suarez H, Erickson DL (1975) Pituitary adenomas of adolescents. J Neurosurg 43: 437-439.
- Neilson K, de Chadarévian J (1987) Ectopic anterior pituitary corticotropic tumour in a six-year-old boy: Histological, ultrastructural and immunocytochemical study. Virchows Arch A Pathol Anat Histopathol 411: 267-273.
- Kleinschmidt-DeMasters BK, Winston KR, Rubinstein D, Samuels MH (1990) Ectopic pituitary adenoma of the third ventricle. Case report. J Neurosurg 72: 139-142.
- Mitsuya K, Nakasu Y, Nioka H, Nakasu S (2004) Ectopic growth hormone-releasing adenoma in the cavernous sinus-Case Report. Neurol Med 44: 380-385.
- Kaushik C, Ramakrishnaiah R, Angtuaco EJ (2010) Ectopic pituitary adenoma in persistent craniopharyngeal canal: Case report and literature review. J Comput Assist Tomogr 34: 612-614.
- Pojskic M, Zbytek B, Beckford NS, Boop FA, Arnautovic KI (2017) First report of coexistence of two ectopic pituitary tumors: Rathke cleft cyst and silent adrenocorticotropic hormone adenoma. World Neurosurg 104: 1048.
- Wang H, Yu W, Zhang Z, Xu W, Zhang F, et al. (2010) Ectopic pituitary adenoma in the spheno-orbital region. J Neuroophthalmol 30: 135-137.
- Mudd PA, Hohensee S, Lillehei KO, Kleinschmidt-Demasters BK (2012) Ectopic pituitary adenoma of the clivus presenting with apoplexy: Case report and review of the literature. Clin Neuropathol 31: 24-30.
- Ferraz-Filho JRL, Torres US, Teixeira ACV, Castro MLS, Dias MAF (2012) Ectopic growth hormone-secreting pituitary adenoma involving the clivus treated with octreotide: Role of magnetic resonance imaging in the diagnosis and clinical follow-up. Arq Neuropsiquiatr 70: 744-745.
- Erdogan N, Sarsilmaz A, Boyraz EI, Ozturkcan S (2012) Ectopic pituitary adenoma presenting as a nasopharyngeal mass: CT and MRI findings. Clin Neurol Neurosurg 114: 414-416.
- Bobeff EJ, Wisniewski K, Papierz W, Stefanczyk L, Jaskólski DJ (2017) Three cases of ectopic sphenoid sinus pituitary adenoma. Folia Neuropathologica 55: 60-66.
- Hata N, Inoue T, Katsuta T, Iwaki T (2003) Ectopic pituitary adenoma in the cavernous sinus causing oculomotor nerve paresis-Case report. Neurol Med Chir 43: 399-403.
- Horiuchi T, Tanaka Y, Kobayashi S, Unoki T, Yokoh A (1997) Rapidly-growing ectopic pituitary adenoma within the sphenoid sinus-Case report. Neurol Med Chir 37: 399-402.
- Akyel NG, Alimli AG, Demirkan TH, Sivri M (2018) Persistent craniopharyngeal canal, bilateral microphthalmia with colobomatous cysts, ectopic adenohypophysis with Rathke cleft cyst, and ectopic neurohypophysis: Case report and review of the literature. Childs Nerv Syst 34: 1407-1410.
Citation: Kawtharani S, Ali B, Horanieh E, El Housheimy M, Darwish H, et al. (2024) Growth Hormone Secreting Ectopic Pituitary Adenoma: Case Report and Literature Review. J Otolaryng Head Neck Surg 10: 089.
Copyright: © 2024 Sarah Kawtharani, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.