Hand Grip Strength in Post-COVID-19 Individuals: Comparison of two Approaches in Occupational Therapy
*Corresponding Author(s):
Elisabete RoldãoOT, Polytechnic Institute Of Leiria, School Of Health Sciences, CiTechCare, Leiria, Portugal
Email:elisabete.roldao@ipleiria.pt
Abstract
Handgrip strength reflects the strength of the upper limbs and is used as an indicator of health and functionality. COVID-19 causes great loss of strength and functionality in hospitalized patients. This study focuses on Occupational Therapy intervention to achieve gains in hand grip strength, in post-COVID-19 individuals, who have been in an inpatient situation. The goal of the study is to show that both types of intervention (conventional Occupational Therapy or using the Biometrics E-link® G200 dynamometer with game interface) reveal gains in hand grip strength in post-COVID-19 individuals and counts with two participants, randomly inserted into the intervention types. The Disabilities of the Arm, Shoulder (DASH) was used to assess the functionality of the upper limb. The Dynamometer G200 of the Biometrics E-Link® as used to assess the hand grip strength with the American Society of Hand Therapists Evaluation Protocol. Witch participant receives one type of intervention, one using the G200 Dynamometer gaming interface and the other through a conventional Occupational Therapy rehabilitation program. The results allowed us to realize the gains that the OT intervention can have with post-COVID-19 individuals. Thus, we believe that this study can be a first step towards something to be developed in the future.
Keywords
COVID-19; Handgrip strength; Occupational therapy
Introduction
COVID-19
COVID-19 is a disease that spread worldwide at the end of 2019. In March 2020, the World Health Organization reported that we were going through a pandemic because SARS-CoV-2 spread in more than 185 countries, becoming highly contagious [1,2]. The highest transmission rate of SARS-CoV-2 occurs in the first three days of incubation of the virus, but may vary between 2 and 14 days, until symptoms are manifestation. The most common symptoms are dry cough, fever, and shortness of breath. The less common symptoms are runny nose, headaches and muscle pains, tiredness, and sore throat. In the most severe cases of COVID-19, individuals may have renal and other organ failure, pneumonia, and acute respiratory failure [3].
COVID-19 may be asymptomatic or symptomatic. Being symptomatic, the clinical picture can be classified as mild, severe, or critical. Regardless of age, any individual may have a critical clinical condition [1]. The main change in individuals who have been diagnosed with a severe clinical case of COVID-19 is the onset and development of pulmonary fibrosis. In addition, they may also present lesions at the myocardial level, cognitive decline, such as memory changes, attention, and loss of speed of information processing associated with it. Other sequelae are fatigue and decreased muscle strength [4,5].
This study aims to verify if different interventions, such as a conventional approach in Occupational Therapy, or a game interface with the use of Biometrics E-link® Dynamometer D200, have results, in post-COVID-19 patients.
Hand grip strength
According to studies conducted, hand grip strength is higher in men than in women, and in dominant hand. It progressively increases until the third decade of life and decreases after, as age advances [6,7]. It is a measure of muscle strength, which can be used as a screening in the measurement of hand and forearm strength, and as a mean of assessing the physical conditions of the upper limb [8]. The hand grip strength reflects the isometric strength of the upper limbs and is related to other muscle groups, so it is regularly used as an indicator of general health. Is known that the commitment of hand grip strength causes incapacity to perform daily activities [9,10]. Hand grip strength is directly related to quality of life since it makes individuals more physically independent. Therefore, if this force is not affected, the person has a functional capacity to perform his Activities of Daily Living autonomously and the occurrence of changes at the social and psychological level is also prevented [11].
Occupational Therapy in hand grip strength
The main objective of Occupational Therapy is to restore or compensate for lost functions, to prevent the future development of functional complications, and to improve or maintain occupational performance and performance skills, according to the health status of the person, thus promoting autonomy and involvement in occupations throughout the lives of individuals [12].
The Occupational Therapy process consists of assessment, intervention and its results followed by a reassessment. It is this process that will define how professionals work with their patients, and there needs to be constant cooperation with the therapist [12].
Users hospitalized in the Intensive Care Unit are subject to a constant immobilization, due to their state of health or because of it, which leads to the need to act early, so that the person does not completely lose the functionality of the limbs. Therefore, therapists have the role of increasing the quality of life of each of these people, through the establishment of intervention plans for the increase and maintenance of muscle strength. This intervention may include increased muscle strength through mobilizations, Activities of Daily Life training, follow-up, and family training, as well as prescription and training of the use of assistive technology products. This intervention should be performed during hospitalization because rehabilitation in this period is crucial to prevent complications in the quality of life of these people [13].
In outpatient intervention, it will be necessary to carry out a new evaluation, to build an appropriate rehabilitation plan, focusing on occupation and functionality. Since one of the most persistent symptoms of COVID-19 is fatigue, it is important for the user, the implementation of energy conservation techniques in the performance of their daily activities, the adaptation of the environment and the adequacy of posture during the performance of the activities. Thus, to avoid a high energy expenditure, a routine should be structured, considering all the factors that can lead to this energy expenditure during the performance of the activities [13]. In addition to fatigue, COVID-19 affects muscle strength, not only as a sequel due to virus infection, but also due to the long period of hospitalization and inactivity. This strength can be increased using significant activities using various therapeutic materials [13]. Technology has also been offering greater possibilities in all areas, including health and gains in strength, and therapists promote the introduction of the most relevant technologies for the intervention of each person, in order to provide more independence and autonomy [14].
Methods and Materials
An exploratory cross-sectional study of double cases was conducted, in which the participants were people in post-COVID-19. The inclusion criteria, considered, were aged between 20 and 55 years, who have been hospitalized in Intensive Care Unit or COVID ward and residents in Portugal. Pregnant women or individuals with previously neurological and/or musculoskeletal disorders, which directly affected the upper limb, diagnosed, would be excluded from the study.
The research was announced in the social media and the sample was obtained from the outpatient of a local Hospital. The characterization was made through a questionnaire collecting age, gender, clinical condition, and hospitalization situation.
To assess strength was used the Dynamometer G200 do Biometrics E-link® that measures strength from 0.1 kg up to 90 kg and can be applied in people with acute hand injuries or debilitating chronic diseases. In this study, it was used for the hand grip strength test, performing 3 attempts in each hand, and the software will issue a table with these three results and the average of them [15]. The American Society of Hand Therapy Protocol was used [16]. The DASH questionnaire was used to assess the functionality of the upper limbs. It is a self-assessment instrument with a measurement window of the last week, so each activity should be evaluated based on what the individual performed in the last week before its application [17]. This study is approved by the Ethics Committee of the Polytechnic of Leiria, with the number CE/IPLEIRIA/01/2022.
In the first contact with the participant’s, informed consent was presented, with all the information about the study, and all the doubts were clarified. All data collected throughout the study were used exclusively for research purposes. During data collection, an alphanumeric encoding was used, so the identity of each participant remained confidential. The characterization questionnaire was completed followed by the application of the DASH questionnaire and finally, the hand grip strength was evaluated using the dynamometer.
Cases
Participant 01
History of the patient: Right-handed male with 34 years old. Lives with his wife and two children. Was a Marine in the Navy for 8 years and is currently an electronics technician. He has always been healthy, performs physical exercise frequently and was diagnosed with COVID-19 in August 2021, being hospitalized for 10 days in a COVID ward. He never received any kind of rehabilitation intervention during the hospitalization.
Participant 02
History of the patient: Female, right-handed with 33 years old. Lives with his partner and daughter. She is, at the moment, an operator at a supply pump. She has always been a healthy person, with no diagnosed pathologies. Six years ago, she was diagnosed with bilateral pneumonia, was in a coma for 28 days, recovered without any diagnosed injuries. In January 2022 she was infected by SARS-CoV-2, and was hospitalized for 20 days, 11 of them in an induced coma. During this time, she received rehabilitation treatments in Physiotherapy and the same happened after discharge from an outpatient clinic, in addition to Physiotherapy was also indicated for speech therapy treatments.
Intervention
The interventions were performed at the Assistive Technology and Occupational Performance Laboratory of the Polytechnic Institute of Leiria. The participants in the study were submitted to 15 sessions of intervention, in one case 3 times a week in the other 2 times a week, with a minimum duration of 40 minutes, individually. Before and after these sessions the assessment protocol was implemented. The last session was the same as the initial session, and the initial questionnaire was not applied again.
Intervention with Participant 01 consisted in 15 sessions of different strength gain exercises and conventional rehabilitation materials were used. There was a focus on a muscle strengthening program, some of the materials used in the interventions were elastic band, finger exercisers, rubber resistance network, springs, silicone, and others. The times in the performance of each exercise were timed and increased with the course of the intervention and the capacity of the participant.
Intervention with Participant 02 consisted in 15 sessions using the games available in the Biometrics E-link® software. The program was also muscle strengthening, using the dynamometer and the pinchmeter. The performance times of each exercise were timed directly by the software and there was the possibility of increasing strength intervals in each game, so these were increased by the during the interventions.
Results
Participant 01
The results of the initial and final evaluation of Participant 01 regarding the DASH questionnaire are presented in table 1.
|
Responses |
to Assessment |
Reassessment |
|
Unable |
1 |
0 |
|
Very difficult |
3 |
0 |
|
Some Difficulty |
6 |
1 |
|
Little Difficulty |
10 |
9 |
|
No Difficulty |
10 |
20 |
|
Total |
30 |
30 |
Table 1: DASH assessment and reassessment results - Participant 01.
The results of the initial and final assessment of Participant 01 regarding the DASH questionnaire - Optional Module Work, are in table 2.
|
Responses |
to Assessment |
Reassessment |
|
Unable |
0 |
0 |
|
Very difficult |
1 |
0 |
|
Some Difficulty |
3 |
3 |
|
Little Difficulty |
0 |
1 |
|
No Difficulty |
0 |
0 |
|
Total |
4 |
4 |
Table 2: DASH assessment and reassessment results, regarding the Work-related Module - Participant 01.
Participant 01, in the initial assessment, although minimally functional, at the level of the upper limbs, reports not presenting difficulties only in 10 items of the DASH questionnaire. After the 15 intervention sessions, of conventional Occupational Therapy interventions, identified no difficulties in 20 of the 30 items, doubling the number of activities in which it does not identify difficulties.
In the optional work module of the DASH, the participant answer, "Very Difficult" only in one item, and "Some Difficulty" in 3 items. In the reassessment he does not identify items in which it has "Very Difficult" and identifies 3 in which it has "Some difficulty" and 1 in which it has "Little Difficulty". So, he identifies 4 items in both assessments but decreases the level of difficulty he felts during the realization of the correspondent activities.
In relation to the hand grip strength assessment, it was assessed with the dynamometer of the Biometrics E-Link® that automatically register the result of witch one of the trials, calculate the average and the percentage of Coefficient of Variation. The position of the handle of the dynamometer is the Position 2, as recommended by the American Society of Hand Therapy. The results obtained are presented in figure 1. 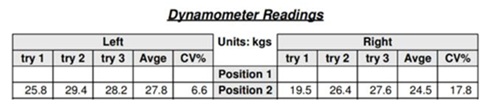
Figure 1: Hand Grip Strength Assessment -Participant 01.
After the 15 intervention sessions, the hand grip strength was measured again, following the same protocol as the initial assessment (Figure 2). There were significant improvements in the medium of the hand grip strength with an increase of almost 20 kilograms on the left hand and 23 kilograms on the right hand.
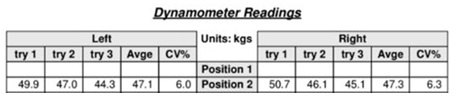 Figure 2: Hand Grip Strength Reassessment -Participant 01.
Figure 2: Hand Grip Strength Reassessment -Participant 01.
Participant 02
The results of the initial and final assessment of Participant 02 regarding the DASH can be viewed in table 3 to perceive the functionality of the upper limbs. The optional module of the work was not applied to this participant, since she is on sick leave. Examining the table, its understood that Participant 02 had as the most frequent response "Some Difficulty", with 13 items selected in the assessment and 12 in the reassessment. Less frequent was the classification "Unable", with 1 selected item in the assessment and none in the reassessment. There were 8 responses with "No Difficulty" in the assessment having reduced to 6 responses in the reassessment.
|
Responses |
to Assessment |
Reassessment |
|
Unable |
1 |
0 |
|
Very difficult |
4 |
2 |
|
Some Difficulty |
13 |
12 |
|
Little Difficulty |
4 |
6 |
|
No Difficulty |
8 |
10 |
|
Total |
30 |
30 |
Table 3: DASH assessment and reassessment results - Participant 02.
Regarding the hand grip strength, the procedures were the same as Participant 01 and the results obtained are presented in figures 3 and 4. There were significant improvements in the medium of the hand grip strength with an increase of approximately 9 kilograms on the left and on the right hand.
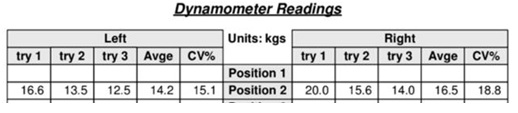 Figure 3: Hand Grip Strength Assessment -Participant 02.
Figure 3: Hand Grip Strength Assessment -Participant 02.
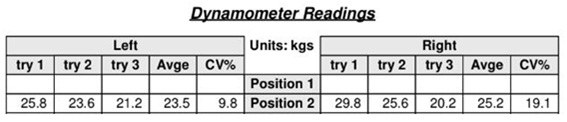 Figure 4: Hand Grip Strength Reassessment -Participant 02.
Figure 4: Hand Grip Strength Reassessment -Participant 02.
Discussion
After 30 days of COVID-19 infection and discharged from the hospital, sequelae such as shortness of breath, cough, fatigue, muscle weakness and limitations in daily activities may appear, which will affect occupational performance throughout the day. According to a study conducted by Thomas et al., most individuals with post-COVID-19 sequelae are on sick leave, thus bringing them feelings of impotence and affecting economic components and psychological health, resulting in a rupture of their habits and routines. According to this same study, consisting of 30 post-COVID-19 participants hospitalized, most of the symptoms listed were neuropathy, followed by muscle weakness and, finally, the difficulties in performing activities of daily living. Those who found themselves hospitalized longer, presented more sequelae and some were even dependent on the help of another person or totally dependent on the performance of daily activities [18].
Users who are hospitalized in the Intensive Care Unit should receive constant rehabilitation, so there is a better evolution of their condition. The cares performed by occupational therapists are: change of positioning, to prevent the appearance of pressure ulcers and facilitate breathing; performance of occupations and training of Activities of Daily Living, to avoid a great loss of functionality; realization of mobilizations, in order to prevent the loss of range of motion and in the realization of adaptations and graduation of activities, using energy conservation techniques, due to the interference that COVID-19 has at the respiratory and muscular level. After this intervention within hospitalization, recovery becomes easier and faster, the hospitalization time is reduced, and the person obtains greater independence, well-being, and quality of life after hospitalization. Therefore, the fact that post-COVID-19 people who are hospitalized have received or not rehabilitation, will influence the hand grip strength and the speed of recovery [19].
In the present study, there are no significant differences in the ages of the participants, however one is female and the other male. According to previous studies, individuals of opposite genders have significant differences in hand grip strength, and the female gender has lower values than males [20].
According to the study implemented by Thomas et al., regarding changes in the upper limbs, the majority presented as the most affected limb, after COVID-19, the right upper limb or both members. There were only 13.3% of the participants with the left upper limb affected and 23.3% without any affected members. In addition, participants with changes in the upper limbs are more dependent on Activities of Daily Living [18].
In a study conducted with the Spanish population, it was possible to verify that men, in the 30-39 years old, have as average of hand grip strength of 50.9 kilograms in the dominant hand, and 41.2 in the non-dominant hand. The women have on average 28.2 kilograms in the dominant hand and 23.5 kilograms of hand grip strength in the non-dominant hand. Since there are no studies conducted on the normative values of the hand grip strength in the Portuguese population, this study considers the values of the Spanish population, since it is the most similar culturally and genetically [20].
After analysing the results of this study, it was noticed that both cases obtained significant improvements, since Participant 01 increased 22.8 kilograms of strength in the right hand (47.3-24.5) and 19.3 kilograms in the left hand (47.1-27.8). Participant 02 increased 8.7 kilograms of strength in the right hand (25.2-16.5) and 9.3 kilograms in the left hand (23.5-14.2). Both cases get closer to the normative mean values of hand grip strength of the Spanish population. The increase in hand grip strength may have been influenced by external variables that we did not control. Also, their intrinsic motivation and resistance to exertion could influence the results. Comparing the data to the study conducted by Thomas et al., both participants, 01 and 02, had an initial hand grip strength higher than the mean of the study, and the most affected limb was also the right upper limb [18].
Regarding the completion of DASH, in relation to Participant 01, the results after the 15 sessions have significative differences, with an increase in the functionality of the upper limbs. Participant 02, only filled the DASH of 30 items, obtaining an initial score of 35 points and in the reassessment a score of 30 points, there were improvements in the functionality of the upper limbs, although not significant.
Conclusion
We were able to verify that both types of intervention in Occupational Therapy obtained results. We recommend the Occupational therapy interventions in patients post COVID-19 with decreasing hand grip strength. We also recommend that studies be conducted with a larger number of participants to verify which of the two approaches has the best results. We suggest that these be made only in one of the genres and with more restricted inclusion criteria to make more conclusive statements in relation to the results.
Acknowledgment
The authors disclosed receipt support for the research of this article: This work was supported by the Center for Innovative Care and Health Technology (ciTechCare), Polytechnic Institute of Leiria, Leiria, Portugal, and the financial support provided by the Portuguese Foundation for Science and Technology (FCT) to their research unit (REF UIDB/05704/2020).
Conflicts of Interest
Authors declare no conflict of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
- Souto XM (2020) COVID-19: aspectos gerais e implicações globais. Ciência e Tecnologia 2: 2674-9270.
- ERS (2020) informação de monitorização Impacto da pandemia COVID-19 no Sistema de Saúde – período de março a junho de 2020. Entidade Reguladora de Saúde, Portugal.
- World Health Organization (2019) Coronavirus Disease 2019 Q&As. World Health Organization, Geneva, Switzerland.
- World Health Organization (2021) Clinical management of COVID-19 rehabilitation: for patients with lung impairment after COVID-19 illness. World Health Organization, Geneva, Switzerland.
- Nogueira TL, Silva SDAD, Silva LHD, Leite MVS, Rocha JFAD, et al. (2021) Pós covid-19: as sequelas deixadas pelo Sars-Cov-2 e o impacto na vida das pessoasacometidas. Archives of Health 2: 457-471.
- Feix T, Romero J, Schmiedmayer BH, Dollar MA, Kragic D (2016) The Grasp Taxonomy of Human Grasp Types. IEEE Transactions on Human-Machine Systems 46: 66-77.
- Roldão E, Pascoal AG (2018) Manual Grip Force of the Adult Population and its Relation to Health Conditions – A Possible Protocol. Res Net Health 4: 1-9.
- Litchfield ER (2013) Grip Strength - What is it? What does it mean? Human Sciences Extension and Outreach Publications 38.
- Carreira H, Amaral FT, Silva CB, Oliveira MB, Borges N (2010) Força de preensão da mão numa amostra de crianças dos 11 aos 14 anos. Acta Med Port 23: 811-818.
- Kimura GB, Zago NN, Grecco AM, Fernandes FL, Rodrigues M (2017) Avaliação da força de preensão e funcionalidade após fratura distal de rádio. Revista Interinstitucional Brasileira de Terapia Ocupacional 1: 490-498.
- Gadelha BV, Sardeli VA, Santos MW, Ribeiro PC, Moraes FD, et al. (2017) Importância da força muscular para a qualidade de vida de idosos sedentários. Revista Brasileira de Qualidade de Vida 9: 153-164.
- Gomes MD, Teixeira L, Ribeiro J (2021) Enquadramento da Prática da Terapia Ocupacional: Domínio & Processo 4aEdição. Escola Superior de Saúde, Politécnico de Leiria.
- Carlo MMD, Ferraz ACG, Rezende G, Buin L, Moreira D, et al. (2020) Diretrizes para a assistência da terapia ocupacional na pandemia da COVID-19 e perspectivas pós-pandemia. Medicina (Ribeirão Preto) 53: 332-369.
- Rocha E, Castiglioni M (2005) Vista do Reflexões sobre recursos tecnológicos: ajudas técnicas, tecnologia assistiva, tecnologia de assistência e tecnologia de apoio.
- Biometrics Ltd (2022) E-LINK for Hand Therapy. Biometrics Ltd, USA.
- Fess EE, Moran C (1981) Clinical assessment recommendations. American Society of Hand Therapists, USA.
- Cheng SMH (2006) Disabilities of the arm, shoulder, and hand - dash: análise da estrutura fatorial da versão adaptada para o portugués. Master’s thesis, Escola de Educação Física, Fisioterapia e Terapia Ocupacional da Universidade Federal de Minas Gerais.
- Thomas C, Brandão P, Andrade P, Oliveira A, Comin M (2022) Avaliação de preensão palmar em pacientes Pós-Covid-19 com disfunção em membro superior e seu impacto na funcionalidade 22: 107-122.
- Carmo GP, Nascimento JS, Santos TR, Coelho PS (2020) Therapeutic-occupational interventions for patients with COVID-19 in ICU. Revista Interinstitucional Brasileira de Terapia Ocupacional – REVISBRATO 4: 397-415.
- Nascimento M, Benassi R, Caboclo F, Salvador A, Gonçalves L (2010) Valores de referência de força de apreensão manual em ambos os gêneros e diferentes grupos etários. Um estudo de revisão. Efdeportes Com 1-10.
Citation: Roldão E, Bastos B, Almeida M, Ventura O (2022) Hand Grip Strength in Post-COVID-19 Individuals: Comparison of two Approaches in Occupational Therapy. J Altern Complement Integr Med 8: 273.
Copyright: © 2022 Elisabete Roldão, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.