Hemiepiphysiodesis via the Bowen Method for Genu Valgum in Adolescents
*Corresponding Author(s):
Hanel Watkins EberlyPenn State College Of Medicine, Hershey, Pennsylvania, United States
Tel:+1 6267716948,
Email:haneljune@gmail.com / hwatkins@pennstatehealth.psu.edu
Abstract
Objective
Surgical techniques using bone blocks, screws, plates and staples have been described to biologically manipulate the growth plate to correct leg length inequality, genu varum and genu valgum. This study aimed to evaluate adolescents undergoing percutaneous hemiepiphysiodesis for correction of genu valgum.
Methods
An IRB-approved retrospective review was conducted for 26 patients who underwent percutaneous hemiepiphysiodesis for genu valgum correction. Hemiepiphysiodesis, was performed at the medial physis of the tibia +/- femur. Patients were followed for measurement of Intermalleolar (IM) gap and Femorotibial (FT) angle correction. Seventeen females and 9 males were studied.
Results
The average age at time of surgery was 12.6 years. The average net IM distance and FT angle correction was 9.9 cm and 10.1º. Fourteen patients (54%) underwent femoral and tibial growth plate manipulation; correction rate for IM distance was 0.7cm/month and FT angle was 1.1º/month. Ten patients (38%) underwent tibial growth plate manipulation; correction rate for IM distance was 0.7 cm/month and FT angle was 1.3º/month. Patients with closed Distal Phalanx (DP) growth plates on bone age radiographs, indicating pending skeletal maturity, were more likely to undergo FT physis manipulation.
Conclusion
Percutaneous hemiepiphysiodesis is a safe and effective method to correct genu valgum. The success rate was 92%. No patients required completion of the hemiepiphysiodesis. The timing of the procedure is based on skeletal maturity by bone age.
Keywords
Genu valgum; Hemiepiphysiodesis; Orthopedics; Pediatric; Percutaneous
Introduction
Genu valgum is part of a normal physiologic process in children. During development, the Femorotibial (FT) angle progresses in a varus to valgus fashion. Before 1 year, an infant may reach up to 15º of varus. At 2 years of age, children approach neutral. By 3 years old, children can progress to maximum valgus before spontaneously correcting to approximately 6º before age seven [1]. Persistent genu valgum may be unilateral or bilateral in nature, with persistent genu valgum most often bilateral in nature. Etiologies such as growth plate disorders, skeletal dysplasias and idiopathic usually present bilaterally. Trauma to the knee or infections can lead to unilateral genu valgum. Indications for surgery have included: 1) unacceptable cosmesis; 2) genu valgum >15º after age seven; 3) asymmetry; 4) Intermalleolar (IM) distance greater than 7.5cm; 5) altered gait; 6) pain and 7) decreased participation in physical activity [2,3].
Various surgical approaches have been described in the literature as effective treatments for patients with angular deformities of the lower extremity [4-9]. Physeal manipulation has the advantage of decreased morbidity when compared to more invasive methods such as an osteotomy [10,11]. Phemister described growth arrest by physeal manipulation in 1933 by rotation of the epiphyseal plate 90° to create a bony bridge [12]. Blount and Clarke described controlling physeal growth in 1949 through epiphyseal stapling [13]. Temporary hemiepiphysiodesis can be obtained using tension-band plating, percutaneous transphyseal screws and stapling [14-16].
A method described by Bowen, percutaneous hemiepiphysiodesis, however, offers the advantage of minimally invasive surgery without return to the or for hardware removal. In the Bowen technique, a selected area of the growth plate is identified and ablated leading to growth inhibition and gradual limb correction [17,18]. Timing of when to perform hemiepiphysiodesis for optimal physeal ablation and deformity correction is key to successful outcome and is guided by bone age radiographs [19-21].
In this study, we analyzed the outcomes of twenty-six children with idiopathic genu valgum undergoing percutaneous hemiepiphysiodesis of the proximal tibia or proximal tibia and distal femur in order to report outcomes, safety and efficacy.
Methods
This study was approved by the medical school Institutional Review Board (IRB). A retrospective study was conducted of 26 patients and 51 limbs with idiopathic genu valgum between the years of 2006-2017. Clinical patient demographics recorded included: gender, age and chief complaint. Additional radiographic demographics recorded were: bone age radiographs of open or closed Distal Phalanx (DP) joint (Figure 1A and 1B), location of hemiepiphysiodesis and initial presentation to surgery length. Patients included in this study were 1) 16 years or younger; 2) male or female gender; 3) diagnosed with genu valgum and 4) recipients of percutaneous hemiepiphysiodesis.
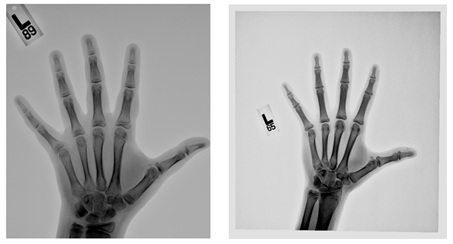 Figure 1: Anteroposterior radiograph of the L hand and wrist displaying open (A) and closed (B) DP growth plates in two different patients with genu valgum.
Figure 1: Anteroposterior radiograph of the L hand and wrist displaying open (A) and closed (B) DP growth plates in two different patients with genu valgum.
In order to determine the degree of deformity, IM distance measurements were made with the patient supine, legs flat and touching of the medial femoral condyles. An IM distance greater than 7.5cm was considered abnormal [2,3]. The FT angle was measured clinically preoperatively with AP radiographs and a goniometer to help guide the surgical procedure (Figure 2). Indications for surgery included pre-operative IM distance greater than 7.5cm and FT angles greater than 12º in addition to patient symptomatology.
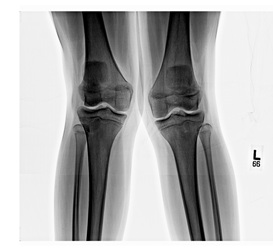 Figure 2: Preoperative anteroposterior radiograph of bilateral knees displaying genu valgum.
Figure 2: Preoperative anteroposterior radiograph of bilateral knees displaying genu valgum.
The surgical technique was based on the original described by Bowen and Johnson [9]. A tourniquet was used. The limb was prepped and draped in a sterile fashion. The physis was identified with a metal marker over the skin and a C-arm (GE OEC 9900 Elite). A 10-mm incision was made with a No. 15 scalpel on the medial aspect of the physis. A 2mm K-wire was placed into the physis to a depth of about 40% (Figure 3A). A 10mm cannulated reamer was placed over the K-wire to ream the physis (Figure 3B). Wire-guided hemiepiphysiodesis was performed by reaming the medial physis. A curved curette was used to curette in all directions to cause a nice hemiepiphysiodesis effect (Figure 3C). Patients received tibial manipulation only or both femoral and tibial manipulation. Patients received tibial and/or femoral manipulation based on bone age, clinical deformity and discussion with the patients and guardians on the risks and benefits of each procedure.

Figure 3: Intra-operative anteroposterior view of K-wire (A), 10-mm reamer (B) and curette (C) in percutaneous hemiepiphysiodesis of the proximal tibia.
Postoperative FT angles were recorded for each patient on subsequent visits in a similar fashion to preoperative measurements. The average net FT angle correction, correction rate and time to final correction were recorded. The average postoperative IM distance net correction and correction rate were also recorded.
The net IM distance and net FT angle correction rate for tibial manipulation only was compared to patients who received tibial and femoral manipulation. Relationship between DP physis closure and receiving the combined procedure was estimated. Statistical analyses were performed using R version 3.4.2 [1,2].
Results
There were 26 total patients and 51 limbs analyzed in this study. Seventeen (65%) patients were female and 9 (35%) were male. The most common chief complaint recorded was a cosmetic complaint followed closely by complaints of pain along the anterior knee joint and feelings of patellar instability. There were a total of 10 patients (20 limbs) with closed DP growth plates; no patients had closure at the distal radius on bone age films. Of the limbs undergoing percutaneous hemiepiphysiodesis, 28 (55%) received proximal tibia and distal femur manipulation, 20 (39%) received proximal tibia manipulation, 2 (4%) received femoral manipulation only and 1 (2%) patient received unilateral proximal tibia manipulation.
The average preoperative IM distance for all patients was 17.2(+/-5.4)cm and postoperative was 7.3(+/-6.8)cm. The average net IM correction for all patients was 9.9(+/-4.7)cm. The average preoperative FT angle for all limbs was 17.4(+/-4.7)º and postoperative was 7.3(+/-4.2)º. The average net FT angle correction for all patients was 10.1(+/-4.5)º. Patients were followed on average for 16.9(+/-11.9) months after surgery. The average tourniquet time for all surgeries was 20.6(+/-10) minutes. There were 4 limbs (7.8%) that were under-corrected and required a later return to the or for correction with osteotomy (Table 1). Both of these patients had preoperative IM distances of greater than 20cm and FT angles greater than 25º bilaterally.
|
Average Pre-op IM Dist. (SD) |
17.2 (5.4) cm |
|
Average Post-op IM Dist (SD) |
7.3 (6.8) cm |
|
Average Net IM Correction (SD) |
10 (4.7) cm |
|
Average Pre-op FT Angle (SD) |
17.2 (4.8) deg |
|
Average Post-op FT Angle (SD) |
7.3 (4.2) deg |
|
Average Net FT Angle Correction (SD) |
11 (4.5) deg |
|
Average Follow-up time (SD) |
16.9 (11.9) months |
|
Tourniquet Time (SD) |
20.6 (10.0) min |
|
Under-correction |
4 limbs |
Table 1: Average preoperative, postoperative and net IM and FT angle measurements.
The average age of males and females undergoing the combined procedure was 14 years and 13.3 years, respectively. The average age of males and females undergoing proximal tibia manipulation was 12.3 and 11.3 years, respectively. The correction rates for IM distance and FT angle for patients undergoing bilateral proximal tibia or femoral and tibial manipulation were also analyzed. Measurements included in these results reflect measurements taken at the first year of follow-up. The average IM distance and FT angle correction rate for patients undergoing proximal tibia manipulation were 0.7cm/month and 1.3º/month with net corrections of 10.4cm and 9.6º, respectively. For patients undergoing both femoral and tibial manipulation, the average IM distance and FT angle correction rate were 0.7cm/month and 1.1º/month, with net corrections being 9.8cm and 9.9º, respectively. Patients with closed DP growth plates were more likely to undergo the combined procedure than patients with open DP growth plates (7.14; 95% CI 1.88-27.16) (Table 2).
|
IM Distance |
||
|
Tib Manipulation Only (n=8) |
Fem/Tib Manipulation (n=9) |
|
|
Correction rate (cm/month) |
0.66 |
0.67 |
|
Net correction |
10.4 |
9.8 |
Table 2: IM distance correction rate and net correction.
Discussion
Medial hemiepiphysiodesis by drilling and curetting under fluoroscopic imaging is an effective way to manage adolescents with idiopathic genu valgum. The average postoperative net IM correction was 9.9cm with an average IM distance correcting from 17.2cm to 7.3cm. The average postoperative net FT angle correction was 10.1º, with an average postoperative FT angle of 7.3º. When analyzing patients undergoing the combined procedure or tibial manipulation only, we saw similar results with other studies. Inan [19], achieved successful valgus correction utilizing percutaneous hemiepiphysiodesis in patients with preoperative deformities of 12º to postoperative valgus measurements of 4º. Ferrick [22], demonstrated an average mechanical axis correction of 10º, with a correction rate for FT manipulation of 1.1º per month over a one-year period, similar to our study that showed a correction rate of 1.1º for combined manipulation in the first year. Bowen [18], demonstrated an average net FT angle correction of 4.4º per physis and in another study [17], demonstrated 11.8º of net FT angle valgus correction using percutaneous hemiepiphysiodesis, similar to our average of 10.1º for all patients.
There were 2 patients out of 26 that were under-corrected. Both patients were indicated for an osteotomy. Of note, both patients had a preoperative IM distance greater than 20cm and had severe valgus deformities in one or both lower extremities with preoperative FT angles greater than 25º. Two other patients had continued bilateral patellar instability and were managed with a brace. Genu valgum has been demonstrated to lead to lateralization of the patella making patients more susceptible to instability [23]. Patients who do not receive correction of their valgus deformity may be at risk for unsuccessful outcomes due to persistent genu valgum and its significant association with patellar instability [24].
In the current study, the average age of all patients at the time of the combined procedure was 13.4 years compared to 11.9 years in patients undergoing proximal tibia manipulation only. The measured correction rates of these patients were equal. Patients undergoing FT manipulation were more skeletally mature than patients undergoing tibial manipulation only. The current study demonstrates that patients more skeletally mature may need both femoral and tibial growth plate manipulation due to a slow-down in growth as they reach skeletal maturity.
One key to percutaneous hemiepiphysiodesis is appropriate operative timing. Lower limb growth has been demonstrated to cease approximately 2 years and 6 months after fusion of the distal phalangeal joint in children [25,26]. This may be an optimal time for patients to undergo permanent hemiepiphysiodesis as their remaining growth period begins to decline and therefore relying on guided growth techniques may not be sufficient. No patient in this study was overcorrected, nor did any patient require completion of the hemiepiphysiodesis. Other studies analyzing timing of permanent hemiepiphysiodesis have suggested proceeding with the procedure within 1-2 years of growth remaining with close follow-up [22].
Troy et al. evaluated percutaneous epiphysiodesis using drill/curettage versus transphyseal screws [27], in 115 adolescents with Leg-Length Discrepancy (LLD). Both procedures demonstrated equal efficiency in resolving LLD, with similar operative times and Length of Hospital Stay (LOS). However, the advantage of drill/curettage is that it typically does not require a return to the operating room for subsequent hardware removal [28,29].
Permanent percutaneous hemiepiphysiodesis offers several advantages compared to other methods of temporary epiphysiodesis. Bowen’s method does not require a second return to the or for hardware removal. No patients experienced any evidence of postoperative infections in our study. No rebound phenomena occur. Cosmetically, the procedure is performed percutaneously and there is minimal scarring. Hardware is not needed [5,15,30]. Limitations of the current study include retrospective design, small sample size and a single surgeon cohort.
Conclusion
Percutaneous hemiepiphysiodesis is a safe and effective method to correct genu valgum in adolescents. The procedure was 92% successful. No patient in this study was over-corrected. The optimal time for the combined femorotibial procedure is when the distal phalanx physis begins to close. In the rare case of under-correction, osteotomy may be indicated.
Acknowledgement
This study was exempted by the Penn State College of Medicine Institutional Review Board. This work was performed at Penn State College of Medicine and Penn State Hershey Medical Center. The authors have no conflicts of interest to report. No funding was involved. There were no proprietary interests in the materials described in the article.
References
- Salenius P, Vankka E (1975) The development of the tibiofemoral angle in children. J Bone Joint Surg Am 57: 259-261.
- Kling TF, Hensinger RN (1983) Angular and torsional deformities of the lower limbs in children. Clin Orthop Relat Res 176: 136-147.
- Howorth B (1971) Knock knees. With special reference to the stapling operation. Clin Orthop Relat Res 77: 233-246.
- Ballal MS, Bruce CE, Nayagam S (2010) Correcting genu varum and genu valgum in children by guided growth: Temporary hemiepiphysiodesis using tension band plates. J Bone Joint Surg Br 92: 273-276.
- Nouh F, Kuo LA (2004) Percutaneous epiphysiodesis using transphyseal screws (PETS): Prospective case study and review. J Pediatr Orthop 24: 721-725.
- Burghardt RD, Herzenberg JE (2010) Temporary hemiepiphysiodesis with the eight-Plate for angular deformities: Mid-term results. J Orthop Sci 15: 699-704.
- Fraser RK, Dickens DR, Cole WG (1995) Medial physeal stapling for primary and secondary genu valgum in late childhood and adolescence using transphyseal screws (PETS). J Bone Joint Surg Br 77: 733-735.
- Scott AC, Urquhart BA, Cain TE (1996) Percutaneous vs. modified phemister epiphysiodesis of the lower extremity. Orthopedics 19: 857-861.
- Bowen RJ, Johnson WJ (1983) Percutaneous Epiphysiodesis. Clin Orthop Relat Res 190: 170-173.
- Maase P, Zreik H (1985) Can one determine the age at which epiphysiodesis should be performed in the treatment of genu valgum in the adolescent? Rev Chir Orthop Reparatrice Appar Mot 71: 319-325.
- Metaizeau JP, Wong-Chung J, Bertrand H, Pasquier P (1998) Percutaneous Epiphysiodesis using Transphyseal Screws (PETS). J Pediatr Orthop 18: 363-369.
- Phemister DB (1933) Operative arrestment of longitudinal growth of bones in the treatment of deformities. J Bone Joint Surg Am 15: 1-15.
- Blount WP, Clarke GR (1949) Control of bone growth by epiphyseal stapling: A preliminary report. J Bone Joint Surg Am 31: 464-478.
- Park H, Park M, Kim SM, Kim HW, Lee DH (2018) Hemiepiphysiodesis for idiopathic genu valgum: Percutaneous transphyseal screw versus tension-band plate. J Pediatr Orthop 38: 325-330.
- Brauwer VD, Moens P (2008) Temporary hemiepiphysiodesis for idiopathic genua valga in adolescents: Percutaneous Transphyseal Screws (PETS) versus stapling. J Pediatr Orthop 28: 549-554.
- Gottliebsen M, Rahbek O, Hvid I, Davidsen M, Hellfritzsch MB, et al. (2013) Hemiepiphysiodesis: Similar treatment time for tension-band plating and for stapling: A randomized clinical trial on guided growth for idiopathic genu valgum. Acta Orthop 84: 202-206.
- Bowen RJ, Torres RR, Forlin E (1992) Partial epiphysiodesis to address genu varum or genu valgum. J Pediatr Orthop 12: 359-364.
- Bowen JR, Leahey JL, Zhang ZH, MacEwen GD (1985) Partial epiphysiodesis at the knee to correct angular deformity. Clin Orthop Relat Res 198: 184-190.
- Inan M, Chan G, Bowen JR (2007) Correction of angular deformities of the knee by percutaneous hemiepiphysiodesis. Clin Orthop Relat Res 456: 164-169.
- Blair VP, Walker SJ, Sheridan JJ, Schoenecker PL (1982) Epiphysiodesis: A problem of timing. J Pediatr Orthop 2: 281-284.
- R Core Team (2018) R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria.
- Ferrick MR, Birch JG, Albright M (2004) Correction of non-Blount’s angular knee deformity by permanent hemiepiphyseodesis. J Pediatr Orthop 24: 397-402.
- McWalter EJ, Cibere J, Macintyre NJ, Nicolaou S, Schulzer M, et al. (2007) Relationship between varus-valgus alignment and patellar kinematics in individuals with knee osteoarthritis. J Bone Joint Surg Am 89: 2723-2731.
- Frosch KH, Schmeling A (2016) A new classification system of patellar instability and patellar maltracking. Arch Orthop Trauma Surg 136: 485-497.
- Dimeglio A (2001) Growth in pediatric orthopaedics. J Pediatr Orthop 21: 549-555.
- Kelly PM, Diméglio A (2008) Lower-limb growth: How predictable are predictions? J Child Orthop 2: 407-415.
- Troy M, Shore B, Miller P, Mahan S, Hedequist D, et al. (2018) A comparison of screw versus drill and curettage epiphysiodesis to correct leg-length discrepancy. J Child Orthop 12: 509-514.
- Volpon JB (1997) Idiopathic genu valgum treated by epiphyseodesis in adolescence. Int Orthop 21: 228-231.
- Zuege RC, Kempken TG, Blount WP () Epiphyseal stapling for angular deformity at the knee. J Bone Joint Surg Am 61: 320-329.
- Pistevos G, Duckworth T (1977) The correction of genu valgum by epiphyseal stapling. J Bone Joint Surg Br 59: 72-76.
Citation: Monahan K, Eberly HW, Pan T, Anagnostakos J, Konopitski A, et al. (2021) Hemiepiphysiodesis via the Bowen Method for Genu Valgum in Adolescents. Archiv Surg S Educ 3: 017.
Copyright: © 2021 Kevin Monahan, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.