High IgG4 in a Patient with, Diabetes Mellitus, Ulcerative Colitis, Liver Cirrhosis with Papillary Thyroid Cancer
*Corresponding Author(s):
Makki H FayadhAdvanced Center For Day Care Surgery, Abu Dhabi, United Arab Emirates
Tel:+971 6227700,
Email:makkihf@yahoo.com
Abstract
Objectives: As increased serum concentrations of IgG4 have been observed in several diseases with aberrant immunological condition such as malignant tumors, autoimmune diseases especially rheumatoid arthritis and allergic.
We describe a patient with high IgG4, liver cirrhosis, the ulcerative colitis, diabetes mellitus, prostatitis, venous thrombosis and thyroid cancer.The relationship between elevated IgG4 and these diseases is discussed.
Case study: A 56 years old male with diabetes mellitus on insulin, ulcerative colitis on azathioprine & adalimumab developed deep skin pigmentation and liver enzymes elevation with portal hypertension and liver cirrhosis followed by portal vein thrombosis with persistently elevated IgG4, azathioprine & adalimumab were stopped. Golimumab started but after 3 infusions,papillary thyroid cancer developed, total thyroidectomy followed by radio iodine.
Ulcerativecolitis was treated with vedolizumab with good response. Liver disease progressed with bleeding varices and portal vein thrombosis with factor Leiden V mutation. IgG4 was high which may high direct or indirect relation to liver cirrhosis, diabetes mellitus and thyroid cancer. The safety of immunosuppressive & biologic agents in patients with high IgG4 need to be reviewed. Awareness is needed about the relationship between high IgG4 and multiple complex diseases is needed
Conclusion: A patient with elevated IgG4, liver cirrhosis, diabetes mellitus, and ulcerative colitis developed skin pigmentation and papillary thyroid cancer, the role of IgG4 is questioned.
Keywords
Diabetes mellitus; Diseases; IgG4; Liver cirrhosis; Thyroid cancer
BACKGROUND
IgG4-Related Disease (IgG4 RD) is a clinical entity including a wide variety of diseases, formerly diagnosed as Mikulicz’s disease, Autoimmune Pancreatitis (AIP), interstitial nephritis, prostatitis andretroperitoneal fibrosis [1-4].
Characteristics common to all forms of IgG4-RD include elevated serum IgG4 concentration and tissue infiltration by IgG4-positive plasma cells, accompanied by tissue fibrosis and sclerosis.
As increased serum concentrations of IgG4 have been observed in several diseases with aberrant immunological condition unrelated to IgG4-RD, such as malignant tumors, autoimmune diseases especially rheumatoid arthritis and allergic diseases, increased IgG4 concentration is not a specific marker for IgG4-RD [2].
Since this complex multisystem disease represented a single pathogenetic disorder manifesting in a variety of target organs, the diagnosis of IgG4-RD is largely based on biopsy results showing enhanced infiltration by IgG4-positive plasma cells, storiform fibrosis, obliterative phlebitis and moderate eosinophilia, all of which are frequently observed in the affected tissues of these patients [1-8].
A high number of IgG4-positive plasma cells in tissue is a hallmark of IgG4-RD, even when serum IgG4 concentrations are below the cut-off level [4]. IgG4-RD tends to be both under diagnosed and over diagnosed [1-8].
Each criterion contains organ-specific clinical symptom and characteristic radiological findings of IgG4-RD, even with steroidal trial in some.
We reportedour initial experience in the United Arab Emirate on high IGG4 associated with pachymenigitis, inflammatory bowel diseases, celiac disease, thyroiditis, retroperitoneal fibrosis, auto immune pancreatitis & sclerosing cholangitis [6].
CASE STUDY
A Male 55 years old with BMI 25, with strong family history of diabetes mellitus & myocardial infarctions in brothers and father.
His diabetes mellitus started 1997 treated with oral hypoglycemic with poor control, insulin started 2005, and developed left sided ulcerative colitis 2015 treated with mesalazine 3.2 g, azathioprine 200mg and courses of budesonide 9 mg.
Frequent relapses of colitis with positive ameba and another relapse with positive clostridium difficile infection treated with metronidazole successfully (Figures 1&2).
 Figure 1: Colonoscopy 2016 left sided ulcerative colitis.
Figure 1: Colonoscopy 2016 left sided ulcerative colitis.
 Figure 2: Gastroscopy early esophageal varices
Figure 2: Gastroscopy early esophageal varices
January 2016 because of the colitis frequent relapses, adalimumab started but 6 months later developed recurrent deep vein thrombosis lower limbs and discovered to have factor V Leiden mutation, treated with oral anti-coagulants.
Hematuriadeveloped, ultrasound showed small bilateral kidney stones with large prostate. 2018 because of darkening of the skin and elevation of the liver enzymes with portal vein thrombosis and cirrhotic liver with splenomegaly, azathioprine was stopped and continued on adalimumab.
Because of frerquent relapses with adalimumab, golimumab infusions was started July 2018.Only 3 doses given but the patient developed thyroid swelling, biopsy confirmed papillary thyroid cancer (Figure 3).
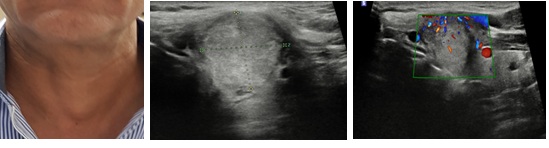 Figure 3: Neck swelling develope after 3 infusions of golimumab.
Figure 3: Neck swelling develope after 3 infusions of golimumab.
Golimumab was stopped, total thyroidectomy followed by radio iodine therapy after which developed severe sialoadenitis that resolve on steroids. His IgG4 was repeatedly elevated high over 250- 300 (normal 84). In 2018 September, Vedozilumab started for his active ulcerative colitis.
March 2019 developed severe anemia hemoglobin dropped to 7 grams; urgent gastroscopy showed grade 4 esophageal varices with duodenal inflammatory polyp, variceswere band ligated (Figure 4).
 Figure 4: Gastroscopy 2019 extensive varices with duodenal inflammatory poly.
Figure 4: Gastroscopy 2019 extensive varices with duodenal inflammatory poly.
Currently stable with hepatosplenomegaly, esophageal varices, portal vein thrombosis on oral anti-coagulants, insulin and vedozilumab, last IgG4 was 214 ( N 86).
DISCUSSION
IgG4 RD is increasingly recognized entity and canbe associated with a variety of gastrointestinal and hepatobiliary manifestations including autoimmune pancreatitis, sclerosing cholangitis, and inflammatory bowel diseases more with ulcerative colitis than Crohns disease, celiac disease in addition to involvement of salivaryand thyroid glands.
Under diagnosis is due to a lack of recognition of this disease, and over diagnosis results from the well intentioned enthusiasm of physicians and/or pathologists who recognize IgG4-RD and diagnose similar conditions as IgG4-RD.
A definite diagnosis of IgG4-RD by CD criteria requires all three diagnostic characteristics: Clinical evidence, high (>135 mg/dl) serum igg4 and pathological certification (>10 igg4+ cells/hpf and igg4+/igg cell ratio >40%).
Some patients may not satisfy these specific serological and /or histopathological criteria because of the difficulty of obtaining biopsies, and therefore cannot be diagnosed with definite IgG4-RD [1-8]. Several Japanese medical societies, including those for gastroenterology, pancreas, biliary tract, rheumatology, ophthalmology and respiratology, have published organ specific criteria for IgG4-RD [1].
In our patient he has persistently elevated IgG4 with multiple pathologies including diabetes mellitus: ulcerative colitis, liver cirrhosis, thyroid cancer and recurrent venous thrombosis with poor response to most available treatments.
The relation to the high IgG4 could becausative or an associated phenomena and further studies to clarify the link. Awareness is needed to check for this association especially in complex multi organ involvements.
SUMMARY AND CONCLUSION
A male patient with diabetes mellitus, ulcerative colitis with persistently raised IgG4, developed liver cirrhosis, prostatitis & papillary thyroid cancer. His progressive diseases including diabetes mellitus, ulcerative colitis, liver damage that progressed in spite of optimal treatments with immunosuppressive and biologic agents and the persistently elevated IgG4 raised many questions about the possible deleterious effect of IgG4.
His thyroid cancer and the high IgG4 again put questions of the role of IgG4 and neoplasia. His poorly controlled diabetes and l raise the question if it causative or an associated phenomena and the prognostic significance of the elevated value. The safety of biologic agents in patients with elevated IgG4 need to be studied the reaction to radio iodine with sialoadenitis may also be related to high IgG4. The infection with clostridium difficle and associated colitis make it difficult to manage and need further observations.
Finally, in complex diseases like this with diabetes, liver cirrhosis with portal hypertension and ulcerative colitis and thyroid cancer, if he need liver transplant in the future, would it be a cluster transplant, liver, pancreas with colectomy and would high IgG4 affect the scenario?
The important question is that IgG4 may be related to his multiple diseases. More data is needed on the role of IgG4 and these multiple and complex diseases. Awareness is needed on the relationship of elevated IgG4 and complex multi organ diseases.
CONCLUSION
IgG4 RD is increasingly recognized entity and can be associated with a variety of gastrointestinal and hepatobiliary manifestations including auto immune pancreatitis, sclerosingcholangitis, inflammatory bowel diseases, celiac disease in addition to involvement of salivary and thyroid glands.
In our patient he has elevated Igg4 with multiple pathologies including:, diabetes mellitus, ulcerative colitis ,liver cirrhosis and venous thrombosis,thyroidcancer and infections including clostridium difficle. Awareness is needed to check for IgG4 in multiple organ involvements.
REFERENCES
- Stone JH, Zen Y, Deshpande VN (2012) IgG4-related disease. N Engl J Med 366: 366:1643-1647.
- Kamisawa T, Zen Y, Pillai S, Stone JH (2015) IgG4-related disease. Lancet 385:1460-1471.
- Shimosegawa T, Kanno A (2009) Autoimmune pancreatitis in Japan: Overview and perspective. J Gastroenterol 44: 503.
- Falhammar H, Juhlin CC, Barner C,Catrina SB, Karefylakis C,Calissendorff J (2018) Riedel’s thyroiditis: clinical presentation, treatment and outcomes. Endocrine 60:185-192.
- Kuwata G1, Kamisawa T, Koizumi K, Tabata T, Hara S, et al. (2014) Ulcerative colitis and immunoglobulin G4. Gut Liver 8: 29-34.
- Makki H Fayadh et al., (2019) Overview of the common and rare gastro intestinal diseases in UAE. 2:10
- Miyabe K, Zen Y, Cornell LD, Rajagopalan G, Chowdhary VR, et al. (2018) Gastrointestinal and Extra-Intestinal Manifestations of IgG4-Related Disease. Gastroenterology 155: 990-1003.
- Yu KH, Chan TM, Tsai PH, Chen C-H, Chang Pi-Y (2015) Diagnostic performance of serum IgG4 Levels in patients with IgG4-related disease. Medicine (Baltimore) 94: 1707.
Citation: Fayadh MH, Awadh S (2019) High IgG4 in a Patient with, Diabetes Mellitus, Ulcerative Colitis, Liver Cirrhosis with Papillary Thyroid Cancer. J Clin Stud Med Case Rep 6: 072.
Copyright: © 2019 Makki H Fayadh, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.